


The global SARS-CoV-2 pandemic has generated concern about contagion, especially among healthcare workers who are on the front line.
ObjectiveTo design and analyse the evidence of content validity, internal structure and reliability of a measure of concern about the spread of COVID-19 among Peruvian healthcare workers.
Material and methodsQuantitative study and instrumental design. The scale was administered to 321 health science professionals (78 males and 243 females), whose ages ranged from 22 to 64 years (38.12 ± 9.61).
ResultsAiken’s V-coefficient values were statistically significant. An exploratory factor analysis was performed which indicated the existence of a single factor, and confirmatory factor analysis (CFA) confirmed a satisfactory six-factor model. The CFA solution obtained adequate fit indices (RMSEA = 0.079; P = .05; TLI = 0.967; IFC = 0.980; GFI = 0.971, and AGFI = 0.931), and showed good internal consistency based on Cronbach's alpha coefficient (α = 0.865; CI 95%, 0.83−0.89).
ConclusionsThe scale of concern for COVID-19 infection is a valid and reliable brief measure that can be used for research and professional purposes.
La pandemia mundial producida por el SARS-CoV-2 ha generado preocupación por el contagio, sobre todo en el personal de salud que está en primera línea.
ObjetivoDiseñar y analizar las evidencias de validez de contenido, estructura interna y confiabilidad de una medida de preocupación por el contagio de COVID-19 en personal de salud peruano.
Material y métodosEstudio cuantitativo y diseño instrumental. La escala se aplicó a 321 profesionales de ciencias de la salud (78 varones y 243 mujeres) con edades comprendidas entre los 22 y los 64 (38,12 ± 9,61) años.
ResultadosLos valores del coeficiente V de Aiken fueron estadísticamente significativos. Se realizó un análisis factorial exploratorio, que indicó la existencia de un solo factor. El análisis factorial confirmatorio (AFC) confirmó un modelo satisfactorio de 6 ítems en 1 solo factor. La solución del AFC obtuvo índices de ajuste adecuados (RMSEA = 0,079; P = ,05; TLI = 0,967; CFI = 0,980; GFI = 0,971 y AGFI = 0,931); además; mostró una buena consistencia interna según el coeficiente alfa de Cronbach (α = 0,865; IC95%, 0,83−0,89).
ConclusionesLa escala de preocupación por el contagio de la COVID-19 es una medida breve válida y confiable que se puede utilizar para fines de investigación y función profesional.
The World Health Organization declared the disease caused by the 2019 novel coronavirus SARS-CoV-2 (COVID-19) a public health emergency.1 This situation caused repercussions for the global population, with healthcare personnel, who are on the front line of the response to the COVID-19 pandemic and are considered a population that is at greater risk of infection2 and nosocomial spread, deserving a special mention.3
Even with the proper personal protective equipment (PPE), health workers caring for infected patients can still be infected with the SARS-CoV-2 virus.4 As some reports from China uncover, this population has also been faced with implications for their mental health due to factors such as work overload, which makes them emotionally vulnerable.5 For this reason, in a large number of the hospitals in the Chinese city of Wuhan, a system of work shifts had to be established so that healthcare personnel could rest and avoid being constantly exposed.6
It is in view of this situation that the need arose for the occupational exposure of this type of population to be addressed carefully. For this reason, one of the strategies for the control and prevention of this disease in health institutions is the surveillance and treatment of exposed personnel.7 However, factors such as inadequate protective equipment, insufficient diagnostic tests, work overload and prolonged exposure to infected patients are a cause of risk of infection.8,9 As an example of the seriousness of the circumstances, once the pandemic started, supply of single-use N95 respirators became scarce, leading to recycling to extend the limited stocks of healthcare providers and facilities.10
Consequently, this global crisis has fuelled concern about the spread of COVID-19 among health workers, since the last thing they want is to harm co-workers, close family members and friends. This has been evidenced in research that has found that the most common concern among healthcare personnel causing them stress and anxiety, rather than becoming infected themselves, is transmitting the infection to family and friends.11 Despite these circumstances, it is evident in various contexts that healthcare personnel continue to perform their duties even when they are in a continuous survival mode to protect everyone around them.12
In this scenario in Peru, a number of researchers designed, adapted, and validated tests to assess important aspects of the impact of COVID-19. Thus, a brief scale was created to measure the level of basic knowledge about the coronavirus (KNOW-P-COVID-19)13 composed of nine items distributed in two dimensions. Other researchers designed a scale to assess fatalism in the face of the possibility of infection of the disease (F-COVID-19),14 which is composed of eight items distributed in two factors. A scale has also appeared to measure fear and the magnitude of the problem (MED-COVID-19)15 composed of 13 items distributed in three factors. Lastly, Ruiz Mamani et al.16 validated a scale of concern about infection for Peruvian adults, which consists of six items in one single factor (EPCov-19).
As seen up to this point, emphasis has been placed on the design of instruments for the general population. However, there are no specific tests for healthcare personnel, which constitutes the main motivation to undertake this research by virtue of filling this gap in the scientific literature. In addition, although healthcare workers are responsible for managing the crisis in healthcare centres, they are not immune to the psychological consequences, hence the need to develop instruments to assess concern about the spread of COVID-19 and thus generate evidence on the subject. Therefore, the objective of this research is to design and analyse the evidence of content validity, internal structure, and reliability of a measure of concern about the spread of COVID-19 in Peruvian healthcare personnel.
MethodsStudy design and participantsA cross-sectional instrumental study was carried out.17 Non-probabilistic, intentional criterion sampling was used. A total of 321 professionals of both sexes (78 men and 243 women; aged 22–64 [38.12 ± 9.61] years) from the healthcare area (Medicine, Dentistry, Nursing, Nutrition, Psychology, Obstetrics) in the Puno Region in southern Peru, who wished to participate were included.
Initial selection of itemsA review of the literature was carried out in different sources of scientific information: Google Scholar, PubMed/MEDLINE and SciELO, with the following search terms: “2019-nCoV”, “COVID-19”, “SARS-CoV-2”, “2019 novel coronavirus”, “coronavirus disease 2019”, “novel coronavirus”, “new coronavirus”, “coronavirus 2019”, “concern”, “infection” and “health-care workers”. Then the first draft of the instrument was written, which was reviewed and approved by all the authors.
Technical and methodological informationThe scale of concern about the possibility of infection by COVID-19 (EPPC-Cov19) measures the emotional state that involves fear, restlessness, anxiety and immobility that begin with unknown and negative events, constructed by the cognitive system; in other words, the natural psychological reaction to the unknown, as is the case with COVID-19, which is a new disease that causes uncertainty in healthcare workers. The evidence of the content validity of the scale was analysed. The judgement of eight experts (different from the developers of the scale) was requested, who took into account four criteria for the evaluation of the items (from 0 = not at all relevant/representative/clear to 3 = totally relevant/representative/clear).
ValidationThe evidence of the content validity of the scale was analysed, and the judgement of eight experts (different from the developers of the scale) was requested, who took into account four criteria for the evaluation of the items (from 0 = not at all relevant/representative/clear to 3 = totally relevant/representative/clear). These expert professionals are epidemiologists and intensive care physicians, psychiatrists, clinical psychologists, and intensive care nurses. To quantify the degree of relevance, representativeness and clarity, the Aiken V coefficient and its 95% confidence intervals (95% CI) were used. A V ≥ 0.70 with 95% CI ≥ 0.59 indicates a positive evaluation of the item.18 Then the online survey was applied with Google Forms. Before completing the survey, the participants were told about the objective of the research and informed consent was requested. Participation was voluntary and anonymous.
Data analysisThe analysis was carried out in several stages. In the first, the descriptive statistics (mean ± standard deviation, skewness and kurtosis) of the eight items of the scale were analysed; the value taken into account for skewness and kurtosis was >±1.5 according to Pérez et al.19 In the second phase, an exploratory factor analysis (EFA) was performed following the criteria of Kaplan et al.,20 considering the Kaiser-Meyer-Olkin (KMO) coefficient and the Bartlett test. Parallel analysis revealed the existence of only one factor. Likewise, the estimation method was unweighted least squares with Promin rotation.21 In the third stage, a confirmatory factor analysis (CFA) was executed and structural equation modelling (SEM) was considered. To evaluate the goodness-of-fit measures, we used the goodness-of-fit index (GFI), the adjusted goodness-of-fit index (AGFI), the parsimonious goodness-of-fit index (PGFI), the normalised fit index (NFI), the relative fit index (RFI), the incremental fit index (IFI), the Tucker-Lewis Index (TLI), and the comparative fit index (CFI). The parameters for the root mean square error of approximation (RMSEA) and the root mean square error rate (RMR) were also considered, following the criteria recommended by Hu et al.,22 who point out that GFI, CFI, TLI and NFI should be >0.9 and the RMSEA and SRMR should be <0.08.
For the descriptive analyses and the EFA, the FACTOR Analysis program version 10.1 was used. To execute the CFA, the AMOS statistical software version 21 was used, and to calculate the reliability of the scale, the statistical program SPSS version 25.0 and its respective confidence intervals were used.23
ResultsTable 1 shows that all the items received a favourable evaluation from the experts (V > 0.70). Regarding relevance, it was found that items four and five are the most important and representative (V = 1.00; 95% CI, 0.86−1.00). Regarding the most understandable (clear) items, items five and eight were the best evaluated (V = 1.00; 95% CI, 0.86−1.00). Likewise, we can see that the values of the lower limit (LL) of the 95% CI are adequate and all the values of the V coefficient were statistically significant.
Aiken's V for the evaluation of the relevance, representativeness and clarity of the EPPC-Cov19 items.
| [1,0]Items | [0,2-5]Relevance (n = 8) | [0,6-9]Representativeness (n = 8) | [0,10-13]Clarity (n = 8) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ma | SDb | Vc | 95% CId | M | SD | V | 95% CI | M | SD | V | 95% CI | |
| Item 1 | 2.88 | 0.35 | 0.96 | 0.80−0.99 | 2.88 | 0.35 | 0.96 | 0.80−0.99 | 2.88 | 0.35 | 0.96 | 0.80−0.99 |
| Item 2 | 2.75 | 0.46 | 0.92 | 0.74−0.98 | 2.63 | 0.52 | 0.88 | 0.69−0.96 | 2.38 | 0.52 | 0.79 | 0.60−0.91 |
| Item 3 | 2.88 | 0.35 | 0.96 | 0.80−0.99 | 2.75 | 0.46 | 0.92 | 0.74−0.98 | 2.63 | 0.52 | 0.88 | 0.69−0.96 |
| Item 4 | 3.00 | 0.00 | 1.00 | 0.86−1.00 | 3.00 | 0.00 | 1.00 | 0.86−1.00 | 2.88 | 0.35 | 0.96 | 0.80−0.99 |
| Item 5 | 3.00 | 0.00 | 1.00 | 0.86−1.00 | 3.00 | 0.00 | 1.00 | 0.86−1.00 | 3.00 | 0.00 | 1.00 | 0.86−1.00 |
| Item 6 | 2.38 | 0.74 | 0.79 | 0.60−0.91 | 2.25 | 0.89 | 0.75 | 0.55−0.88 | 2.25 | 0.89 | 0.75 | 0.55−0.88 |
| Item 7 | 2.88 | 0.35 | 0.96 | 0.80−0.99 | 2.88 | 0.35 | 0.96 | 0.80−0.99 | 2.63 | 0.52 | 0.88 | 0.69−0.96 |
| Item 8 | 3.00 | 0.00 | 1.00 | 0.86−1.00 | 3.00 | 0.00 | 1.00 | 0.86−1.00 | 3.00 | 0.00 | 1.00 | 0.86−1.00 |
Table 2 shows the mean ± standard deviation, skewness and kurtosis of the eight items of the EPPC-Cov19. We can see that item five has the highest average score and the greatest dispersion (3.68 ± 1.17). The skewness and kurtosis values of the eight items of the scale do not exceed the interval >±1.5.19 Likewise, the correlations between the items were significant (>0.40).
Descriptions of the EPPC-Cov19 scale.
| [1,0]Items | [1,0]Ma | [1,0]SDb | [1,0]Skc | [1,0]Kd | [0,6-13]Inter–item correlation | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | |||||
| Item 1 | 3.419 | 1.132 | –0.094 | –1.055 | 1 | |||||||
| Item 2 | 2.912 | 1.12 | 0.229 | –0.673 | 0.681 | 1 | ||||||
| Item 3 | 2.172 | 1.131 | 0.834 | 0.047 | 0.555 | 0.722 | 1 | |||||
| Item 4 | 2.146 | 1.146 | 0.777 | –0.315 | 0.503 | 0.589 | 0.692 | 1 | ||||
| Item 5 | 3.682 | 1.174 | –0.435 | –0.94 | 0.647 | 0.588 | 0.484 | 0.519 | 1 | |||
| Item 6 | 3.058 | 1.109 | 0.185 | –0.869 | 0.598 | 0.649 | 0.603 | 0.571 | 0.652 | 1 | ||
| Item 7 | 3.094 | 1.165 | 0.211 | –0.838 | 0.438 | 0.441 | 0.461 | 0.488 | 0.449 | 0.463 | 1 | |
| Item 8 | 2.825 | 1.14 | 0.229 | –0.848 | 0.615 | 0.689 | 0.67 | 0.658 | 0.642 | 0.709 | 0.565 | 1 |
In the first instance, the sample adequacy indices were analysed, the Kaiser-Meyer-Olkin value (KMO = 0.917) and the Bartlett test (1,555.4; gl = 28; P < .001) were very good, indicating that it is adequate to carry out the EFA in the studied sample. The unweighted least squares method was used, and the parallel analysis indicated that the eight items underlie a single factor. The factor obtained explains the 63.89% of the total variance of the test and its factor loadings range between 0.599 and 0.864 (Table 3).
Factorial analysis of the EPPC-Cov19.
| Items | F1 | h2* |
|---|---|---|
| 1. I am concerned about the possibility of catching COVID-19 during my working hours | 0.753 | 0.567 |
| 2. Thinking about the possibility of contracting COVID-19 while doing my job makes me nervous, anxious | 0.826 | 0.683 |
| 3. Thinking about the possibility of contracting COVID-19 in my work environment stops me from sleeping well | 0.787 | 0.619 |
| 4. Thinking about the possibility of contracting COVID-19 affects my ability to carry out my work and personal activities | 0.748 | 0.56 |
| 5. When I leave work, I worry about spreading COVID-19 to family members or people I live with | 0.74 | 0.548 |
| 6. COVID-19 creates uncertainty for me because it is an unpredictable disease | 0.799 | 0.638 |
| 7. At my workplace there are a lot of risks (high infection rates, shortage of PPE, problems with health insurance, etc.) that make me worry about contracting COVID-19 | 0.599 | 0.359 |
| 8. Despite putting biosecurity measures into practice to avoid contracting COVID-19, I can't help but worry | 0.864 | 0.746 |
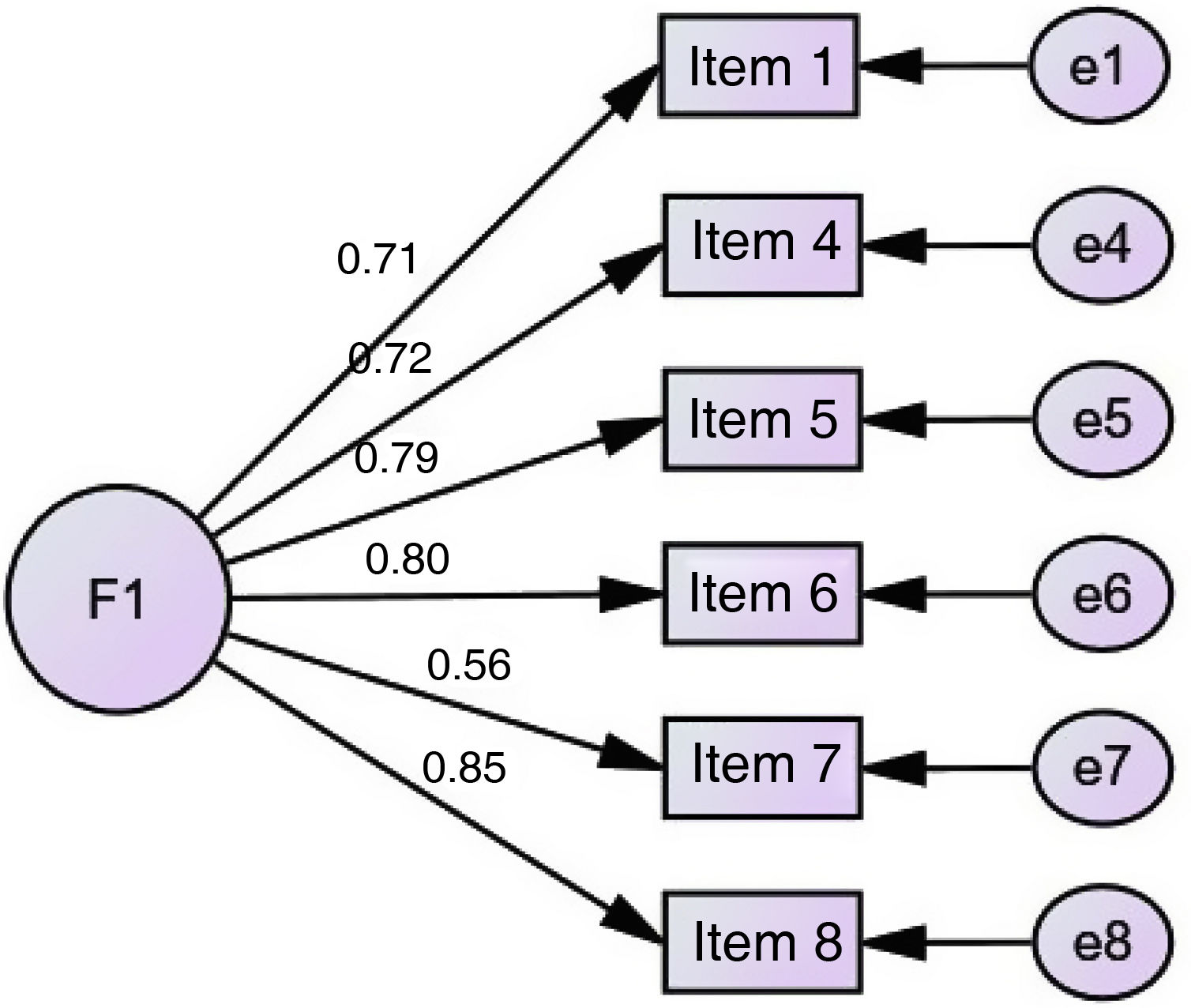
To analyse the internal structure of the scale, an EFA was carried out where the eight items of the EPPC-Cov19 were loaded into a single latent variable; the results of the original model showed that the goodness of fit was poor, therefore, through the index modification technique, items two and three were eliminated and an optimal model remained. The goodness of fit indices show that the proposed model is adequate (χ2 = 27.183; df = 9; P = .001; RMR = 0.036; GFI = 0.971; AGFI = 0.931; PGFI = 0.416; NFI = 0.971; RFI = 0.951; IFI = 0.980; TLI = 0.967; CFI = 0.980, and RMSEA = 0.079) (Table 4). The reliability of the test was calculated using Cronbach's alpha coefficient (α = 0.865; 95% CI, 0.83−0.89). In summary, the six-item model in one single factor is satisfactory (Fig. 1).
General goodness of fit indices.
| [1,0]Goodness of fit index | Original (8 items) | Model 1 (6 items) |
|---|---|---|
| CMIN | 111.408 | 27.183 |
| DF | 20 | 9 |
| p | <0.001 | 0.001 |
| CMIN/DF | 5.570 | 3.020 |
| RMR | 0.051 | 0.036 |
| GFI | 0.920 | 0.971 |
| AGFI | 0.856 | 0.931 |
| PGFI | 0.511 | 0.416 |
| NFI | 0.927 | 0.971 |
| RFI | 0.898 | 0.951 |
| IFI | 0.940 | 0.980 |
| TLI | 0.915 | 0.967 |
| CFI | 0.939 | 0.980 |
| RMSEA | 0.120 | 0.079 |
| β (95% CI) | 0.908 (0.887−0.925) | 0.865 (0.835−0.890) |
α (95% CI): Cronbach's alpha (95% confidence interval); AGFI: adjusted goodness-of-fit index; CFI: comparative fit index; CMIN: c2; CMIN/DF: c2 per degrees of freedom; DF: degrees of freedom; GFI: goodness of fit index; IFI: incremental fit index; NFI: normalised fit index; PGFI: parsimonious goodness-of-fit index; p: p-value; RFI: relative fit index; RMR: root mean square error rate; RMSEA: root mean square error of approximation; TLI: Tucker-Lewis index.

During the months of health emergency, it is not only the general population who have been victims of SARS-CoV-2. This disease has also taken the lives of police officers, public officials and, above all, healthcare personnel. Until the time of writing this study, Peru mourned the loss of 125 doctors throughout the national territory.24 In turn, the concern of healthcare personnel not only affects their private sphere, but also involves the risk of infection to which they expose their relatives, including parents (over 65 years of age), children (young children) and close relatives (patients with comorbidities), which in the worst case could mean the death of one of them. Therefore, the emotional burden and stress to which they are subjected due to the complexities of their professional work add to the risk they represent for their closest relatives.
Thus, the creation and validation of a scale that makes it possible to measure the concern that healthcare personnel experience as a result of the work they do acquires paramount importance, especially in times of pandemic. Mejia et al. had a similar objective, and designed some scales that were validated during the peaks of the Peruvian pandemic and had a highly varied sample that included populations from different parts of Peru, even taking cities as isolated as Iquitos. Thus the F-COVID-19 scale was proposed as an instrument to determine perceived fatality among the general population of Peru.14 Its application in a sample of 2466 people in 20 cities in Peru allowed us to observe that women and those who lived with a comorbidity were more prone to fatalistic ideas such as dying, getting infected or becoming depressed.25 Furthermore, that same work team developed the MED-COVID-19 scale, which measures the magnitude of the perception of fear generated by the information disclosed by the media and the closest circle of the participants.15 With this scale, in a sample of 4009 people it was possible to see that television and social networks were the sources that generated the most news and issued information that caused fear among their viewers.26
The current EPPC-Cov19 scale shows an internal structure and formal validity that are supported by Aiken's V values >0.70. Similarly, other studies that have measured variables related to the psychopathological aspects of the pandemic have obtained Aiken's V values similar to those of this validation.14,15,18 Regarding the exploratory factor analysis, the methods used allowed for grouping all the items into a single factor. Other validation studies, such as the one conducted by Ruiz Mamani et al.16 which aimed to measure concern during the times of COVID-19, reached the appropriate consistency by grouping their six items into one single factor. However, validations carried out in other contexts, such as the one developed by Chandu et al.27 in a sample from India, grouped their items with two factors. It would be appropriate to add that it had many more elements than those contained in this instrument. In addition, reliability measured by Cronbach's alpha coefficient was adequate (>0.80), as proposed by Gliem et al.28 Thus, the EPCov-19 scale obtained coefficients similar to those of this validation when evaluating its reliability.16 The MED-COVID-19 scale, however, obtained values of α > 0.90,15 but the F-COVID-19 scale obtained values of 0.70.14
The study has a series of limitations. The first is related to the sampling method used, which does not allow for its results to be extrapolated beyond the context in which it was carried out. In addition, it would be important to perform an analysis of factorial invariance. Further, focus groups were not carried out in the initial phases of the construction of the scale or evaluations in the target population, nor was there a test-retest reliability analysis, which must be considered when reproducing it in other contexts. However, the evidence of validity based on the content, the internal structure and the level of reliability achieved allow us to be confident that its application and its validation in other realities will be just as profitable as in this experience.
This scale is intended to be used as an instrument to generate public policies that allow us to improve the conditions and mental health status of healthcare personnel who are in charge of treating patients in the context of the pandemic in the different countries of the Latin American region.
Therefore, it is concluded that the EPPC-Cov19 scale has the validity of form and substance and the necessary reliability to assess the concern about infection suffered by Peruvian healthcare personnel during the COVID-19 pandemic. In addition, it is proposed that this instrument be used to measure the real implication of this problem in that specific population.
Conflicts of interestNone.
