









Attention-deficit/hyperactivity disorder (ADHD) is one of the most common behavioural disorders of childhood; its prevalence in Spain is estimated at 5%-9%. Available treatments for this condition include methylphenidate, atomoxetine, and lisdexamfetamine, whose consumption increases each year.
Material and methodsThe prevalence of ADHD was estimated by calculating the defined daily dose per 1000 population per day of each drug and the total doses (therapeutic group N06BA) between 1992 and 2015 in each of the provinces of Castile-La Mancha (Spain). Trends, joinpoints, and annual percentages of change were analysed using joinpoint regression models.
ResultsThe minimum prevalence of ADHD in the population of Castile-La Mancha aged 5-19 was estimated at 13.22 cases per 1000 population per day; prevalence varied across provinces (P<.05). Overall consumption has increased from 1992 to 2015, with an annual percentage of change of 10.3% and several joinpoints (2000, 2009, and 2012). Methylphenidate represents 89.6% of total drug consumption, followed by lisdexamfetamine at 8%.
ConclusionsAnalysing drug consumption enables us to estimate the distribution of ADHD patients in Castile-La Mancha. Our data show an increase in the consumption of these drugs as well as differences in drug consumption between provinces, which reflect differences in ADHD management in clinical practice.
El trastorno por déficit de atención e hiperactividad (TDAH) es uno de los trastornos conductuales más frecuentes de la infancia, se estima su prevalencia en España en un 5-9%. Existen varios fármacos para esta patología como el metilfenidato, la atomoxetina y la lisdexanfetamina cuyos consumos están creciendo anualmente.
Material y métodosSe estima la prevalencia de TDAH a través del cálculo de las dosis diarias definidas por 1.000 habitantes y día de cada fármaco y el total (grupo terapéutico N06BA), durante los años 1992-2015, para cada una de las provincias de Castilla-La Mancha (España). Se observa la tendencia, sus puntos de cambio y los porcentajes anuales de cambio mediante modelos de regresión de joinpoint.
ResultadosSe estima una prevalencia mínima de TDAH de 13,22 casos por 1.000 habitantes y día para Castilla-La Mancha en la población de 5 a 19 años, existiendo una variabilidad provincial (p < 0,05). En su conjunto, el consumo se ha incrementado un porcentaje anual de cambio de 10,3% desde 1992 a 2015 con varios años o puntos de inflexión (2000, 2009 y 2012). El metilfenidato supone el 89,6% de los fármacos consumidos, seguido por la lisdexanfetamina con un 8%.
ConclusionesEl consumo de fármacos permite estimar la distribución de TDAH en Castilla-La Mancha. Se observa un crecimiento en el consumo de estos fármacos, y se observa una variabilidad provincial en su consumo, lo que supone diferencias en la práctica médica frente a esta enfermedad.
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder with potential to become chronic and affects approximately 5% of children.1 It is characterised by attention deficit, hyperactivity, and impulsivity; it does not manifest constantly; rather, the level of functional interference varies.2 Failure to assess the level of dysfunction may lead to an over-estimation of ADHD, as occurs in half of epidemiological studies conducted on the disorder's prevalence in Spain.3 There is growing interest in this disorder due to the increasing number of cases, the administration of psychostimulants to children and adolescents,4 and its status as one of the most frequent neuropsychiatric disorders during childhood.1,2 ADHD was described in a group of children a century ago by Still; the concept, classification, and diagnosis have varied.2,5 The variations in the clinical classification have led to heterogeneity in prevalence figures from different countries, which range from 0.78% in Hong Kong to 17.8% in Germany.5,6 This partly explains the contrast between European prevalence figures of 1% to 2%, and figures of 20% or higher in American studies; more recent meta-analyses estimate a global prevalence of between 3% and 7%, whereas in Spain it is estimated at 6.8%, with a 95% confidence interval (95% CI) of 4.9% to 8.8%.1,3,7–12 Epidemiological studies conducted in Spain have obtained disparate figures due to the differences in the ages included, with prevalence figures of 1% to 2% in Navarre, 3% to 14% in Valencia, 4.6% in Majorca, 4.9% in the Canary Islands, and 4% to 6% in Seville.5,13–15 One meta-analysis of Spanish studies obtained a prevalence figure of 6.8%, with a 95% CI of 4.9% to 8.8%.3
ADHD is a behavioural disorder which may require pharmacological treatment. Such psychostimulants as methylphenidate (MPH) and lisdexamfetamine (LDX), and such non-stimulant drugs as atomoxetine (ATX) are the approved drugs in Spain, and their efficacy and safety have been widely studied.1,2,9,16 Indiscriminate use of MPH in the USA (where more than 80% of the MPH manufactured in the world is consumed)17–21 and Australia has led psychostimulant consumption to triple and quadruple, respectively, from 1991 to 2011. In 2011, 20 cases were treated for every 1000 children aged 4.22–24 However, consumption of the drug in Europe is lower due to legal and pharmacological limitations on prescriptions.12,19,25–29 In Spain, the introduction of drug therapy was delayed by almost a decade, coinciding with the marketing of sustained-release MPH in 2004.16,25,26
MPH has an efficacy of 75% to 80%, improving motor, behavioural, and cognitive manifestations; self-esteem; and social and family adaptation; and improves comorbid ADHD. It is indicated for patients older than 6 (since studies only include patients aged 6-12) and to a lesser extent for adolescents and adults.8,11,12,16 Despite the drug's efficacy, symptoms may persist in 10% to 60% of adults who displayed them during childhood, and 50% may develop psychiatric comorbidities; however, prevalence is 50% lower in adults.1,9,30
This article aims to study consumption trends for ADHD drugs in Castile-La Mancha (CLM), Spain, in the period 1992-2015, and to estimate prevalence of the condition between the ages of 5 and 19 using drug consumption data.
Material and methodsWe used data from the drug database of the Subdirectorate General for Drug Assistance and Supply of the Spanish Ministry of Health and Consumer Affairs for the period 1992-2001, which were published in a previous study25; and data from the database of the Castile-La Mancha Health Service's (SESCAM) Pharmaceutical Monitoring Service for the period 2002-2015. These systems record outpatient use of drugs officially prescribed within the Spanish National Health System and SESCAM. Consumption through these channels is normally considered a close image of actual consumption.25,26 We selected MPH, ATX, and LDX, respectively belonging to the N06BA04, N06BA09, and N06BA12 groups of the Anatomical Therapeutic Chemical Classification System, since they were the drugs available in Spain. We used the defined daily dose (DDD) to measure consumption. DDD is the mean daily dose of an active ingredient used in its main indication, and is the technical measurement unit proposed by the Drug Utilization Research Group of the WHO Regional Office for Europe. The DDD used was proposed by the Nordic Council on Medicines: 30mg for MPH, 80mg for ATX, and 30mg for LDX.31 For geographical comparisons, we calculated the number of DDD per 1000 inhabitants/day (daily dose per inhabitant [DDI]), which represents the proportion (cases per 1000 inhabitants) of population receiving treatment with a given active ingredient, expressed as a daily mean. These are calculated by dividing the number of DDD by 365, which estimates the average number of patients receiving daily treatment with each active ingredient.32 Although these drugs are the first choice in most treatment patterns for ADHD, other patterns not including them are also used.10,11,16,19 Therefore, prevalence estimations based on drug consumption must be considered estimations of the minimum prevalence or the prescription method. Rates (DDI) were calculated based on population data obtained from the Spanish National Statistics Institute (www.ine.es: TEMPUS database) for each year (as of 1 July). We included patients aged between 5 and 19 years (5-year groups of 5-9, 10-14, and 15-19 years), as they are the target population for this treatment and the population included in most international studies.11,24–28
We used joinpoint or segmented Poisson regression models due to their effectiveness in identifying changes in trends. The aim is to analyse the effect of time, which acts as an independent variable, on the calculated rates. In this analysis, joinpoints show the presence of significant changes in the trend (ascending or descending). Every joinpoint indicates a statistically significant change in the trend, and an annual percentage change (APC) is calculated for every trend using general linear models and assuming a Poisson distribution. The 95% CI was calculated for every APC.33,34 The study of differences between provinces for each year was performed using the Friedman test and Kendall W. The level of statistical significance was set at P<.05.
ResultsConsumption of ADHD drugs increased by 98.8% throughout CLM, from an initial 0.15 DDI in 1992 to 13.22 DDI in 2015 (or 13.22 cases per 1000 inhabitants). This parameter can be used to estimate the prevalence of the disorder in CLM in patients aged between 5 and 19 (this increase was homogeneous in all provinces). If the calculation is performed with the total population, we observe that DDI increases from 0.03 in 1992 to 2.07 DDI in 2015.
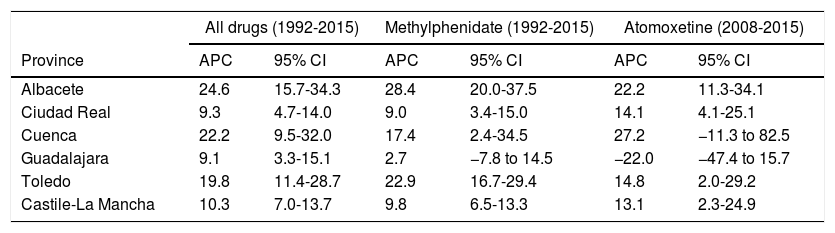
Variability was observed between provinces, with a range between 9.07 DDI in Albacete and 17 DDI in Ciudad Real and Guadalajara, with statistically significant differences (P<.05) (Fig. 1). MPH was the most frequently used drug in 2015, representing 89.6% of the total consumption, ranging from 82.9% in Cuenca to 92.6% in Guadalajara, with statistically significant differences (P<.05). DDI of this drug has increased from 0.15 in 1992 (at which time it was the only drug available) to 11.84 in 2015, which represents a 98.72% increase. LDX was the second most frequently used drug in 2015 (8%), with differences between provinces: the lowest figures were observed in Albacete (5.2%) and the highest in Cuenca (13.6%); thus, DDI in Albacete is 0.47 vs 2.13 DDI in Cuenca (Figs. 2 and 3). ATX is the least used drug in CLM (0.33 DDI) in 2015, and presents the highest level of variability between provinces in terms of DDI and increase in consumption from 2008 (when it was first commercially available) to 2015, with statistically significant differences (P<.05). Overall, consumption of ATX in CLM increased by 61.9% from 0.12 DDI in 2008 to 0.32 DDI in 2015 (Fig. 4). The APC of ADHD drugs in CLM from 1992 to 2015 is 10.3% (95% CI, 7.0-13.7) (Table 1). This growth has not been homogeneous; several significant joinpoints (years 2000, 2009, and 2012) were observed over the period studied (Fig. 5). The APC for MPH from 1992 to 2015 is 9.8% (95% CI, 6.5-13.3) (Fig. 6); an APC of 13.1% was observed for ATX (2008-2015 period) (95% CI, 2.3-24.9).
.")
.")
.")
.")
Annual percentage change in ADHD drugs.
| All drugs (1992-2015) | Methylphenidate (1992-2015) | Atomoxetine (2008-2015) | ||||
|---|---|---|---|---|---|---|
| Province | APC | 95% CI | APC | 95% CI | APC | 95% CI |
| Albacete | 24.6 | 15.7-34.3 | 28.4 | 20.0-37.5 | 22.2 | 11.3-34.1 |
| Ciudad Real | 9.3 | 4.7-14.0 | 9.0 | 3.4-15.0 | 14.1 | 4.1-25.1 |
| Cuenca | 22.2 | 9.5-32.0 | 17.4 | 2.4-34.5 | 27.2 | −11.3 to 82.5 |
| Guadalajara | 9.1 | 3.3-15.1 | 2.7 | −7.8 to 14.5 | −22.0 | −47.4 to 15.7 |
| Toledo | 19.8 | 11.4-28.7 | 22.9 | 16.7-29.4 | 14.8 | 2.0-29.2 |
| Castile-La Mancha | 10.3 | 7.0-13.7 | 9.8 | 6.5-13.3 | 13.1 | 2.3-24.9 |
95% CI: 95% confidence interval; ADHD: attention deficit/hyperactivity disorder; APC: annual percentage change.
. APC: annual percentage change.")
. APC: annual percentage change.")
We observe an increase in the consumption of ADHD drugs in CLM, as has also been reported by other national and international studies.7,19,20,26 Growth was progressive between 1992 and 2000, followed by an inflection that year with the introduction of new forms of presentation of MPH in 1998, and with the introduction of ATX in 2008.7,19,35 By determining the DDD and DDI for the prescription of ADHD drugs, prevalence in CLM in 2015 is estimated at 13.22 cases per 1000 inhabitants in the 5-19 age group. These figures are similar to those obtained by another study conducted in Castile and Leon, estimating 12 cases per 1000 inhabitants for MPH,26 or another conducted in Navarre, which obtained a figure of 14.12 cases per 1000 inhabitants36; the increase was similar, changing from 0.1 cases per 1000 inhabitants in 1992 to 1.5 in 2009 (we obtained 1.42 cases per 1000). Despite the increase in the consumption of LDX since it entered the Spanish market in 2014, becoming the second most frequently prescribed drug in CLM, MPH is still the first-choice drug and represents 90% of consumption.26,36–41 LDX is a prodrug of dextroamphetamine, indicated for children older than 6 years who show no positive response to MPH.16 It is more widely used than ATX in the USA and Australia; the same may also be the case in Europe with the introduction of the drug, since publications highlight the needs yet to be satisfied in ADHD treatment.42There are still few national and international studies on trends in LDX consumption due to its recent introduction.24,39,43,44 Some studies on ADHD drug consumption include modafinil.26,38,44,45 This was not included in our consumption calculations since its use is minimal and largely restricted to adults. Furthermore, the drug has not been included as a routine treatment in the main therapeutic guidelines,1,2,36,46 and its use is not exclusive to this disorder: it can also be used for narcolepsy or fatigue in multiple sclerosis.26,38,39,45 Prevalence of ADHD in adults is estimated at 0.04% of the population (0.02 DDI in 2009 for ATX in Castile and Leon and Ireland)26,38, although some studies report rates as high as 2.5% to 4%.39 Less than one-third of adults diagnosed receive treatment.36,47
Prevalence of ADHD in Spain is estimated at 6.8% of the population,3 which is similar to that reported in Europe (5.5%).7 In our case, we have a figure of 2.02 cases per 1000 inhabitants for the total population, which is lower than that obtained in international studies. However, the growing consumption pattern is approaching that of the Nordic countries, where figures of 2.18 cases per 1000 inhabitants for all ages were reported in 2007 (although there are differences, with 1.88 cases in Iceland and 3.59 in Finland); Australia, with 5.5 cases per 1000 inhabitants in 2011; and Ireland, Israel, and the United Kingdom in 2012, with 8.63, 9.92, and 9.2 cases per 1000, respectively.24,38,40,41,45 Studies in the Netherlands and the United Kingdom, report growth from 1.5 cases per 1000 in 1995 to 21 cases per 1000,28,39,48 similar to the 29 cases per 1000 reported in the USA.17,18 On the contrary, in Italy, Turkey, and France, figures for patients younger than 18 indicate 0.19, 0.59, and 1.8 cases per 1000 inhabitants, which represent the lowest figures for any country.49–51 These figures may be due to the requirement for medical prescription in those countries; however, this is also required in Spain, and figures are higher.51–53 In CLM, we observed an average annual increase in ADHD drug consumption of 10.3% (95% CI, 7.0-13.7), which does not seem to be associated with an increased incidence of the disorder, but rather to an active search for cases, improvements in diagnosis and patient care, drug treatment of less severe cases who were not receiving drugs previously, or greater availability of resources for child and adolescent healthcare.26,27,29,54 Despite this increase, prevalence figures for consumption are lower than those reported in the USA and the Netherlands.18,28,44,45 We should also consider the variability in medical prescription, with differences in the diagnosis and treatment of these children and adolescents, frequently due to the failure to apply the available clinical guidelines and protocols,46 the higher percentage of physicians supporting the use of these drugs, or an increased use in girls. The topic therefore merits further attention.48,55,56
In our case, we cannot explain variability between provinces in terms of social and cultural differences or access to healthcare services, since they are universally available and free of charge (in Israel, the Jewish population present higher rates than the Muslim population), or socioeconomic differences which prevent access,27–29,50,55,56 since the region of CLM is homogeneous and resources are equitably distributed. The drafting of new clinical practice guidelines in Spain and the creation and staffing of child and youth mental health units or child neurology units may improve diagnosis and treatment of this disorder, leading to increased consumption of ADHD drugs.11,19,27–29,46,57 Greater awareness among the general and medical population on psychiatric disorders in children, the introduction of new drugs (with fewer adverse effects and more easily administered), and marketing campaigns by the pharmaceutical industry may lead to increased use of ADHD drugs due to overdiagnosis and overtreatment. Therefore, more children start treatment and for more prolonged periods.22–25,45,56 We must insist on complementing pharmacological therapy with behavioural interventions and the support of the family and school environment,16,36,46,57 in addition to performing follow-up of children, since 19% of them do not have the disorder, which may be leading to unnecessary consumption.24,28,44,45
The SESCAM is able to determine DDI consumption due to its wide coverage and control of drug prescription and dispensing.25,26 In the case of ADHD, the specificity of the prescription of these drugs (MPH, ATX, and LDX) enables us to estimate the prevalence of the disorder. The validity of our data is supported by the follow-up of these patients by specialists, the required medical inspection authorisation for some of the drugs (ATX up to 2013), consensus on the treatment with standard DDD, and their almost exclusive use for this disorder.43,50,51,56,57 Drug consumption is increasing in Spain due to changes in the population pyramid, with the age group studied decreasing in size (the number has decreased from 357455 in 1992 to 323022 in 2015 in CLM); therefore, with the same total consumption, rates increase. Using an age group between 5 and 19 years rather than the total population is demonstrated to have no effect on the rates observed, meaning that regional differences cannot be explained by the effect of age.25,40,58 Also, the population covered by the SESCAM has increased, as have life expectancy, access to specialised case, quality in the prescription of these drugs, and maintenance doses in the case of MPH.16,29 Data on drug consumption in the public health system during the 1992-2015 period are comprehensive, and their use in estimating the prevalence of ADHD depends on all patients receiving the correct treatment (which occurs in 80% of cases due to the therapeutic efficacy of MPH, which is replaced by ATX and LDX in case of MPH failure1,2,11), on the fact that patients are taking the correct doses (since not all the prescribed drugs are consumed due to poor adherence or adverse effects), and on patients consulting with the public health service.25,32 Due to the subsidised price of the drugs and the required medical inspection authorisation, consumption through private prescription is virtually non-existent, further increasing the reliability of this database.25,56,59,60 However, universal coverage and the mental health reform underway in CLM have enabled us to have access to actual user consumption data, which may explain this growing consumption trend.25,26,54 This model only becomes stable when sales data have stabilised with time25,32; and the values obtained are always underestimates.29,59,60 MPH first became commercially available in Spain in May 1981; therefore, the drug and its use are widely known. This is not the case for ATX and LDX, which have been available in the Spanish market for a shorter period, and the hypothetical optimal figure of consumption has not been reached. Therefore, small changes in consumption levels may have caused significant inflection points in the years 2000, 2009, and 2012.60 The 2009 inflection point may be associated with the economic crisis,61,62 but further studies are needed to confirm this hypothesis.
In 2014, a resolution was passed by the Parliamentary Assembly of the Council of Europe to ensure comprehensive treatment of children with ADHD. The resolution proposes that pharmacological treatment should not be the first recourse in mild cases, and should always be accompanied by the combination of such other interventions as psychoeducational therapy.4,57 Pharmacological treatment has been shown to be effective and cost-efficient in the short term, but should not be indicated in mild cases or as the only therapeutic intervention; a multimodal intervention is proposed.1,2,48,57 Despite the clear upward trend in the cost of the drugs, which will cost 4.2 billion dollars in 2015, corresponding to an annual cost of 70 million euros in Spain, the main concern should not be financial, but rather the educational and social impact.23,36,48 Cultural and educational changes in Western society do not favour sustained attention in children, reflexive strategy, or the development of the emotional intelligence and maturity that is later demanded of children.9,24,26,40,49 In this context, families and schools are overwhelmed by cases with complex features (lack of time and specific abilities, difficulty of individualising curricula, collapse of moral authority, competitive pressure, etc.).4,36 Persistence of the disorder, rather than its onset, is associated with difficult family situations.5 The financial crisis, added to an educational crisis, results in a situation that has led to a decrease in the resources and investment in education (support teachers, care for children with special needs),61,62 and to the referral of children with special educational needs to the healthcare sector, converting it into a medical issue.22 In some cases, the drug is a convenient option, with visible results in the short term, and is even more economical than alternatives to pharmacotherapy.36,57
Further studies are needed to identify the reason for the variability in the use of these drugs in the region. Efforts should be made to inform parents, teachers, physicians, psychologists, and public authorities on ADHD, and to improve professionals’ information and training in addition to offering them therapies and diagnosis and treatment guidelines.
FundingNone.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Criado-Álvarez JJ, González González J, Romo Barrientos C, Mohedano Moriano A, Montero Rubio JC, Pérez Veiga JP. Variabilidad y tendencias en el consumo de fármacos para los trastornos por déficit de atención e hiperactividad en Castilla-La Mancha, España (1992-2015). Neurología. 2018;33:360–368.
