



Although cognitive and learning disorders have been described in patients with epilepsy, very few studies focus on specific disorders such as absence epilepsy. The aim of this study was to evaluate learning skills and academic performance in children and adolescents with absence epilepsy.
MethodsObservational case-control study. Cases were chosen from the Central League against Epilepsy's clinic in Bogotá, Colombia. Controls were selected from a private school and matched with cases by age, school year, and sex. Medical history, seizure frequency, antiepileptic treatment, and academic performance were assessed. Academic abilities were tested with Batería de Aptitudes Diferenciales y Generales (BADyG) (a Spanish-language test of differential and general aptitudes). Data were analysed using Student t-test.
ResultsThe sample consisted of 19 cases and 19 controls aged between 7 and 16. In 15 patients, seizures were controlled; all patients had received antiepileptic medication at some point and 78.9% were actively being treated. Although cases had higher rates of academic failure, a greater incidence of grade retention, and more therapeutic interventions than controls, these differences were not significant. Similarly, there were no significant differences on the BADyG test, except for the immediate memory subcategory on which cases scored higher than controls (P=.0006).
ConclusionChildren treated pharmacologically for absence epilepsy, whose seizures are controlled, have normal academic abilities and skills for their age.
Aunque se describen desórdenes cognitivos y trastornos del aprendizaje en pacientes que presentan epilepsia, son pocos los trabajos que estudian trastornos específicos como la epilepsia ausencia. El objetivo del presente trabajo fue evaluar las características escolares y las aptitudes del aprendizaje en niños y jóvenes que presentan epilepsia ausencia.
MétodosInvestigación observacional analítica de casos y controles. Los casos fueron escogidos en la consulta de la Liga Central contra la Epilepsia de Bogotá. Los controles se seleccionaron de un colegio privado y fueron pareados con los casos por edad, grado escolar y sexo. Se evaluaron la historia clínica, la frecuencia de las crisis, el tratamiento farmacológico, el desempeño académico. Las aptitudes escolares se estudiaron por medio de la Batería de Aptitudes Diferenciales y Generales (BADyG). Los datos fueron analizados por medio del test T de Student.
ResultadosLa muestra estuvo conformada por 19 casos y 19 controles entre los 7 y 16 años. Quince pacientes se encontraban controlados, todos habían recibido medicación antiepiléptica y el 78,9% se encontraba con tratamiento activo. Aunque los casos presentaron mayores fallas académicas, más incidencia en pérdidas de grado y mayores intervenciones terapéuticas que los controles, no hubo diferencias significativas. Igualmente no hubo diferencias en la prueba de BADyG, salvo en la subprueba de memoria inmediata en la que los casos tuvieron resultados superiores (p=0,0006).
ConclusiónLos niños con epilepsia ausencia tratados farmacológicamente y controlados en lo que se refiere a crisis tienen las aptitudes y competencias académicas que corresponden normalmente a su edad.
Impairment of cognitive functions, which in turn negatively impacts learning, is one of the most frequent problems in epileptic patients.1–6 As a general rule, epileptic patients show poorer academic performance, present a higher incidence of grade retention and repeated courses, need more psycho-pedagogical support, and are more frequently diagnosed with learning disorders. According to Jackson et al.7 academic difficulties are observed in up to 50% of cases. Such difficulties result from factors inherent to the patient's disease, including aetiology, location of the epileptogenic focus, age at disease onset, seizure frequency, EEG abnormalities, pharmacological treatment, various psychological disorders, psychiatric comorbidities, and the patient's lifestyle.3,8–11 They can also lead to school absenteeism and emotional disorders.12,13
At present, schools do not offer an ideal environment in which children with epilepsy can develop academically. This situation arises because teachers are still unaware of the real aptitudes of children with epileptic syndromes, and they do not know what level of academic performance to expect from them.14
The present study aims to evaluate academic performance and learning skills in children with absence epilepsy younger than 17. Our ultimate purpose is to contribute to implementing pedagogical methods that may help these children improve their academic performance.
Patients and methodsWe conducted an observational study to analyse patient and control groups. These groups consisted of children and adolescents aged 7 to 16 of both sexes, enrolled in elementary and secondary education. Cases were patients diagnosed with absence epilepsy who attended the Central League against Epilepsy clinic in Bogotá, Colombia, during 2011. The control group consisted of children and adolescents with similar characteristics to those listed above but lacking a diagnosis of epilepsy.
All patients and their parents or guardians were contacted by telephone. They were informed about the study and asked to participate. They later signed an informed consent form in order to be included in the study. Parents completed a questionnaire inquiring about various factors related to their children's absence epilepsy, academic performance, and social relationships.
Academic skills were assessed with the Batería de Aptitudes Diferenciales y Generales (BADyG), a Spanish-language test of differential and general aptitudes validated in Colombia. Different types of battery were used according to the grade level: E1 (1st and 2nd grade), E2 (3rd and 4th grade), E3 (5th, 6th, and 7th grade), and M (8th, 9th, 10th, and 11th grade). The Colombian education system includes 5 primary education grades for ages 6 to 11 (grades 1-5) and 6 secondary education grades for ages 12 to 18 (grades 6-11). To assess learning skills, we chose the sub-tests addressing linguistic, memory, and attention capacity, and the development of levels of reasoning. Sub-tests included analogies, completing sentences, letter-number series; maths problems, logical matrices, matching shapes; immediate memory tests, visual-orthographic memory, and identifying differences.15
We also recorded data from student records and each patient's clinical history, including pharmacological treatment, seizure frequency, age at diagnosis, previous treatments, and academic performance. The latter included the most recent marks earned in the basic subjects (Spanish, maths, science, social sciences, English, physical education, and technology and information systems). Marks were classified as poor (0-2.9/5), average (3-3.9/5), high (4-4.5/5), and excellent (4.6-5/5). We decided to compare 2 groups in the final analysis, categorised as poor performance and average-to-excellent performance, since the study variable was poor performance. For this purpose, we considered the number of grade levels repeated by each patient and any need for psycho-pedagogical support.
Data were analysed using SPSS version 20.0. A descriptive analysis was performed for all variables as a first step. We calculated the percentages of occurrence for nominal categorical variables and the mean and standard deviation for quantitative variables. We later tested for normal distribution using the Shapiro-Wilk test and conducted a bivariate analysis of the dependent variable and the results on the BADyG sub-tests using the t-test. The significance level was established at P<.05.
Since the present study did not pose any risks to its participants, it was classified as ‘research with no risk’ according to Resolution 008730/1993 issued by the Colombian Ministry of Health, which establishes the scientific, technical, and administrative requirements for health research. The protocol was approved by the Clinical Research Ethics Committee at the Faculty of Health Sciences at Universidad del Rosario, Bogotá, Colombia. All patients and controls were volunteers and had previously signed an informed consent form. Confidentiality was guaranteed.
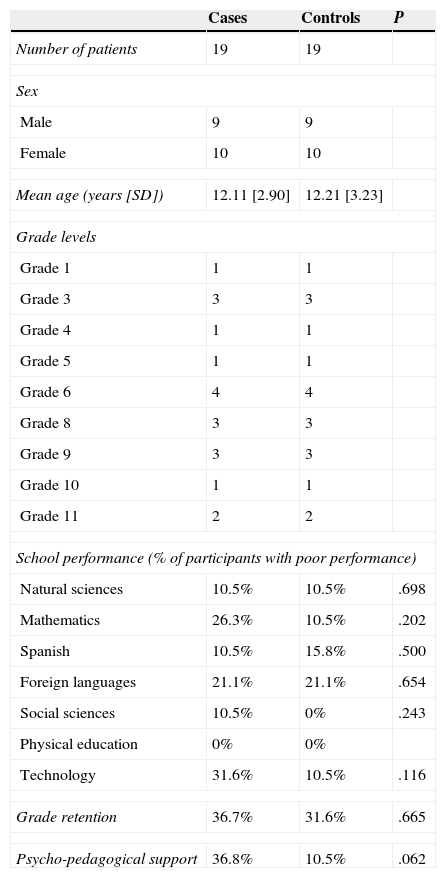
ResultsThe final sample included 38 children aged 7 to 16; 19 of them had been diagnosed with absence epilepsy and the remaining 19 were age-, sex-, and grade-matched controls (Table 1). Grade levels ranged from 1 to 11. Grade distribution was similar for cases and controls, and the median grade was 6th grade.
Demographic characteristics and academic performance
| Cases | Controls | P | |
|---|---|---|---|
| Number of patients | 19 | 19 | |
| Sex | |||
| Male | 9 | 9 | |
| Female | 10 | 10 | |
| Mean age (years [SD]) | 12.11 [2.90] | 12.21 [3.23] | |
| Grade levels | |||
| Grade 1 | 1 | 1 | |
| Grade 3 | 3 | 3 | |
| Grade 4 | 1 | 1 | |
| Grade 5 | 1 | 1 | |
| Grade 6 | 4 | 4 | |
| Grade 8 | 3 | 3 | |
| Grade 9 | 3 | 3 | |
| Grade 10 | 1 | 1 | |
| Grade 11 | 2 | 2 | |
| School performance (% of participants with poor performance) | |||
| Natural sciences | 10.5% | 10.5% | .698 |
| Mathematics | 26.3% | 10.5% | .202 |
| Spanish | 10.5% | 15.8% | .500 |
| Foreign languages | 21.1% | 21.1% | .654 |
| Social sciences | 10.5% | 0% | .243 |
| Physical education | 0% | 0% | |
| Technology | 31.6% | 10.5% | .116 |
| Grade retention | 36.7% | 31.6% | .665 |
| Psycho-pedagogical support | 36.8% | 10.5% | .062 |
The patient group included 13 patients with childhood absence epilepsy, 4 patients with juvenile absence epilepsy, and 2 patients with absence seizures as well as other seizure types. Mean age at diagnosis was 6.68 years (SD 3.019) and mean duration of epilepsy was 5.42 years (SD 2.17).
In 15 patients (78.9%), seizures were controlled at the time of the evaluation: these patients had not experienced seizures for 2 years. Three patients experienced one or more crises per day, and 1 patient experienced a crisis every 2 months.
All patients had been treated with antiepileptic drugs. The 78.9% of the patient total on active treatment were taking valproic acid (47.4%), lamotrigine (15.8%), valproic acid plus lamotrigine (10.5%), and levetiracetam (5.3%). Patients who were not taking drugs had interrupted treatment following doctor's advice. They had previously been taking valproic acid (2 patients) and magnesium valproate (1 patient), and lamotrigine (1 patient). We were not able to analyse the impact of treatment on performance at school and on the BADyG sub-tests due to the small sample size.
Academic performance of participants in both groups differed greatly depending on the subject, and there were high percentages of poor performance among both cases and controls (Table 1). Participants in the patient group performed more poorly in maths, social sciences, and technology than controls, but these differences were not statistically significant.
Patients usually needed more psycho-pedagogical support than controls (36.8% vs 10.5%), although this difference was also non-significant (P=.06). The prevalence of grade retention reached 36.7% in the patient group and 31.6% in the control group. Although there was no clear association between epilepsy and grade retention, it is an interesting fact that 2 epileptic children repeated 2 and 3 grades respectively, whereas no controls repeated more than one grade.
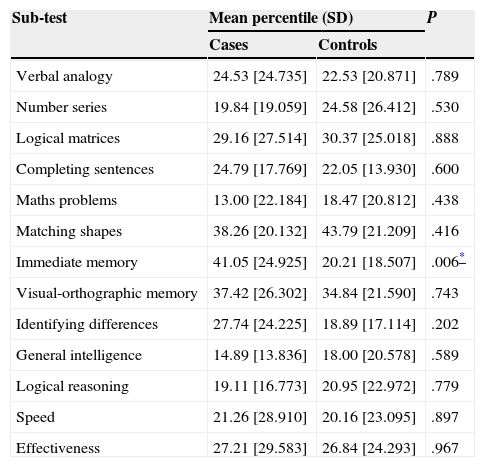
The selected BADyG sub-tests were administered to all participants. Mean values varied between patients and controls, but overall, no clear associations can be drawn (Table 2). The immediate memory test was the only one on which patients achieved higher scores than controls (P=.006).
Scores on BADyG sub-tests
| Sub-test | Mean percentile (SD) | P | |
|---|---|---|---|
| Cases | Controls | ||
| Verbal analogy | 24.53 [24.735] | 22.53 [20.871] | .789 |
| Number series | 19.84 [19.059] | 24.58 [26.412] | .530 |
| Logical matrices | 29.16 [27.514] | 30.37 [25.018] | .888 |
| Completing sentences | 24.79 [17.769] | 22.05 [13.930] | .600 |
| Maths problems | 13.00 [22.184] | 18.47 [20.812] | .438 |
| Matching shapes | 38.26 [20.132] | 43.79 [21.209] | .416 |
| Immediate memory | 41.05 [24.925] | 20.21 [18.507] | .006* |
| Visual-orthographic memory | 37.42 [26.302] | 34.84 [21.590] | .743 |
| Identifying differences | 27.74 [24.225] | 18.89 [17.114] | .202 |
| General intelligence | 14.89 [13.836] | 18.00 [20.578] | .589 |
| Logical reasoning | 19.11 [16.773] | 20.95 [22.972] | .779 |
| Speed | 21.26 [28.910] | 20.16 [23.095] | .897 |
| Effectiveness | 27.21 [29.583] | 26.84 [24.293] | .967 |
| Additional assessments | Mean direct score (SD) | P | |
|---|---|---|---|
| Verbal factor | 21.79 [8.741] | 20.58 [8.662] | .671 |
| Number factor | 14.63 [8.591] | 16.74 [9.457] | .477 |
| Spatial factor | 23.42 [9.430] | 24.32 [8.374] | .759 |
Verbal factor: ability to establish significant connections using verbal constructions (verbal analogies+completing sentences). Number factor: ability to establish significant connections between numbers and to operate with numbers (number series+maths problems). Spatial factor: ability to establish significant connections between geometric shapes (logical matrices+matching shapes).
These findings are insufficient to support the hypothesis that children and adolescents of both sexes with absence epilepsy have poorer learning skills.
DiscussionNumerous studies have addressed different types of learning disabilities in children with epilepsy. These problems are not only because of cognitive impairment but also due to lack of attention and memory and language impairments, among other factors.10,13,16,17 Battistini et al.18 found higher incidence rates of specific learning disabilities (14 out of 16 children with epilepsy) than the expected rate (2-10%) in the Italian Metropolitan City of Milan. The study population described by De Oliveira et al.17 differs from our own but also displays childhood epilepsy (rolandic epilepsy). These researchers observed that epileptic children scored significantly lower than controls on tests assessing academic performance.
A population-based study conducted by Sillanpää in Finland in 1992 found a prevalence rate of 23% for learning disorders and 14.7% for mathematics disorders in epileptic subjects.19 In their study, Dunn et al.20 observed that children with seizures achieved poorer results in reading, mathematics, and writing tests at 36 months after onset than at baseline. Fastenau et al.21 propose the following as potential risk factors for early cognitive deficits: multiple seizures (second unprovoked seizure), use of antiepileptic drugs, symptomatic/cryptogenic aetiology, and epileptiform activity on the initial EEG.
However, most published studies present heterogeneous groups of patients experiencing different types of crises, epileptic syndromes, and aetiologies, with no comparison to a control group.7,22 Regarding generalised epilepsy, Tavera Saldaña et al.23 reported a frequency of learning disabilities of 34.38% in a group of patients with primary generalised epilepsy identified by the Central League against Epilepsy in Bogotá. We aimed to study a similar population diagnosed with absence epilepsy. Although the sample size was small and did not allow us to analyse subgroups, we did assess and compare patients’ results with those of age-, sex-, and grade-matched children. According to our findings, children and adolescents with absence epilepsy did not present poorly developed learning skills or lower results on the BADyG sub-tests. Assessment and analysis of academic performance of epileptic patients yielded similar results to those of controls except in maths, social sciences, and technology: controls scored higher on these subjects, although differences were not statistically significant. However, we did observe a slightly higher prevalence of grade retention and a greater need for psycho-pedagogical support in the patient group. This may suggest that children and adolescents with absence epilepsy are more prone to developing academic problems, which does not mean that they have learning disabilities.
Our findings coincide with those by Fastenau et al.21 who reported no significant differences in neuropsychological functioning between controls and patients with different types of idiopathic epilepsy (including absence epilepsy). On the other hand, a study conducted by Bhise et al.22 found that patients with recent-onset primary generalised epilepsy (and especially absence epilepsy) achieved significantly lower results in vocabulary and short-term auditory memory tests than patients with focal epilepsy. Henkin24 found that patients with absence epilepsy displayed deficits in attention, verbal learning, memory, verbal fluency, and fine motor response. With regard to attention, our study did not find any differences in BADyG sub-test scores between patients and controls.
Oostrom et al. found that patients with idiopathic or cryptogenic epilepsy needed more pedagogical support than controls with similar intelligence and educational levels. However, the two groups displayed similar prevalences of grade retention.13 These findings are consistent with our own.
Pharmaceutical treatments have been reported to have both positive and negative impacts on cognitive skills and academic performance in epileptic patients.25,26 Concerning absence epilepsy, the study by Mandelbaum et al. showed that patients achieved lower scores in the matrices sub-test of the Kaufman Brief Intelligence Test when evaluated at baseline. Nevertheless, these authors observed no cognitive impairment in patients who had been taking antiepileptic drugs for 12 months except in some patients who experienced persistent seizures.27 This team therefore hypothesised that cognitive impairment was attributable to seizure persistence and not to antiepileptic drugs. Although our study did not analyse the direct impact of medication on performance, all patients had taken antiepileptic drugs for an average of 4 consecutive years, and some of them were still under treatment. As concluded by Mandelbaum et al. reduced seizure frequency is very likely to have a positive impact on cognitive skills and academic performance in epileptic patients.2,27
In conclusion, we can state that patients undergoing antiepileptic drug therapy were able to compete on an equal footing with their peers both academically and in other age-appropriate activities. However, our findings cannot be generalised due to small sample size. We recommend conducting collaborative studies evaluating larger groups of children in order to draw firm conclusions. In any case, we believe that patients should be closely monitored by parents and teachers from the onset of the disease until the seizures are under control. This will help them detect potential academic problems and provide appropriate psycho-pedagogical support in order to avoid grade retention and drop-outs.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank the Central League against Epilepsy's clinic in Bogotá, Colombia, for their support and permission to study their patients.
Please cite this article as: Talero-Gutiérrez C, Sánchez-Torres JM, Velez-van-Meerbeke A. Aptitudes de aprendizaje y desempeño escolar en niños y jóvenes con epilepsia ausencia. Neurología. 2015;30:71–6.
