



Dystonias are defined as a joint sustained and involuntary contraction of agonist and antagonist muscles, which can cause torsion, repetitive abnormal involuntary movements, and/or abnormal postures. One special group of dystonias are those known as occupational, which include dystonia disorders triggered by a repetitive motor activity associated with a specific professional activity or task. Musicians are a population particularly vulnerable to these types of dystonia, which are presented as a loss of coordination and voluntary motor control movements highly trained in musical interpretation. Our aim is to describe a clinical series of focal dystonias in musicians evaluated and treated in our centre.
Patients and methodsData are presented on a clinical series of 12 musicians with occupational dystonia. Their history and phenomenology are described, as well as well as their outcome after therapy.
ResultsDemographic details: Mean age 34.8±11.8 years, 10 males (83.3%) and 2 females (16.7%). Clinical history: History of trauma in dystonic segment, 6 patients (50%); family history of neurological diseases in first-degree relatives, 6 patients (50%). Occupational history according to music category: 8 patients (66.6%) were classical musicians and 4 patients (33.3%) were popular musicians.
PhenomenologyDystonia syndrome was characterised by having a mean age of onset of 28.2±11.3 years (range 18–57 years). The segment affected was the hand (91.7%) in 11 patients. Of all the musicians seen in the clinic, 9 of them (75%) received therapy. The majority of patients appeared to have triggering factors specific to musical execution and linked to the requirement of fine motor control. It should be mentioned that 50% of the musicians treated maintained their professional activity or position in the orchestra to which they belonged.
ConclusionsThe majority of our phenomenological findings are consistent with those reported in the current literature. However, it is worth mentioning the presence of triggering factors attributed to the specific requirements of performing music, linked to the participation of fine motor control.
Las distonías se definen como una contracción conjunta, sostenida e involuntaria de músculos agonistas y antagonistas, que puede causar torsión, movimientos involuntarios anormales repetitivos y/o posturas anormales. Un grupo especial de distonías son las conocidas como ocupacionales, que incluyen trastornos distónicos desencadenados por una actividad motora repetitiva, relacionada con la actividad profesional o tarea específica. Los músicos son una población especialmente vulnerable a este tipo de distonías que se presentan como una pérdida de coordinación y control motor voluntario de movimientos altamente entrenados en la interpretación musical. Nuestro objetivo es describir una serie clínica de distonías focales en músicos evaluados y tratados en nuestro centro.
Pacientes y métodosSe presentan los datos de una serie clínica de 12 músicos con distonía ocupacional; se describen sus antecedentes y fenomenología, así como su evolución después de de la terapia.
ResultadosAntecedentes demográficos: edad promedio 34,8±11,8 años, 10 hombres (83,3%) y 2 mujeres (16,7%). Antecedentes médicos: antecedentes traumáticos en segmento distónico, 6 pacientes (50%); antecedentes familiares de enfermedades neurológicas en parientes de primer grado, 6 pacientes (50%); antecedentes laborales según categoría musical, 8 pacientes (66,6%) eran músicos clásicos y 4 pacientes (33,3%) eran músicos populares.
FenomenologíaEl cuadro distónico se caracterizó por presentarse a una edad promedio de inicio de 28,2±11,3 años (rango 18–57 años). En 11 pacientes el segmento afectado fue la mano (91,7%). De todos los músicos consultados, un total de 9 (75%) recibió terapia. En la mayoría de los pacientes se describen desencadenantes específicos de la ejecución musical, asociados a requerimientos de control motor fino. Cabe mencionar que el 50% de los músicos tratados mantuvo su actividad laboral o puesto en la orquesta a la que pertenecía.
ConclusionesLa mayoría de nuestros hallazgos fenomenológicos son coherentes con la literatura actualmente disponible. Sin embargo, nos parece destacable la presencia de desencadenantes atribuibles a requerimientos específicos de la ejecución musical, ligados a la participación del control motor fino.
Dystonias are defined as joint sustained and involuntary contractions of agonist and antagonist muscles which often cause torsion, involuntary and repetitive abnormal movements, and abnormal posture.1–3 Occupational dystonias are a special subgroup that includes dystonia disorders triggered by a repetitive motor activity associated with a specific professional activity or task. Musicians are especially vulnerable to this type of dystonia, which manifests as a loss of coordination and voluntary motor control over the frequently repeated movements employed in playing instruments.4–6
Musician's dystonia is a form of focal dystonia and its prevalence ranges from 0.5% to 1% in musicians.7,8 However, prevalence rates vary substantially depending on the instrument and the level required for performance (dystonia is more prevalent among soloists). The purpose of the present study is to describe a series of musicians with occupational dystonia, characterising the phenomenon itself (including impact on musical performance) and examining demographics, previous occupations, and therapeutic approaches.
Materials and methodsWe conducted a prospective, descriptive study of 12 musicians with occupational dystonia who attended the Movement Disorders Centre (CETRAM) at Universidad de Santiago de Chile between January 2008 and January 2012. Participants completed a semi-structured interview inquiring about their demographic data and medical and employment histories. We collected the following data in all cases:
- (1)
Academic and employment history: professionals (soloist or accompanist) or students, musical genre (classical or popular), main and secondary instruments, and musical education (starting age, years of training, mean daily hours of practice).
- (2)
Complete medical history, including trauma and personal or family history of neurological disorders.
- (3)
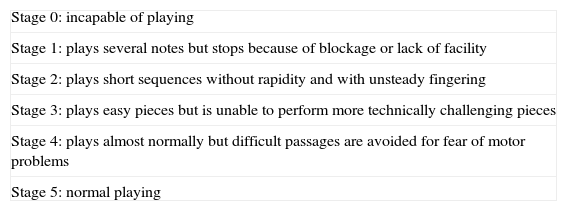
Characterisation: description of the affected segment, lateralisation, severity according to the Tubiana scale for functional impairment in musicians with occupational dystonia9 (Table 1), initial symptoms (loss of motor control in hands while playing, slow movement of fingers or the affected segment, weakness of the affected segment, finger tremor in the affected segment, pain, etc.), and type of abnormal movement (dystonia and/or tremor at flexion or extension).
Table 1.The Tubiana scale for functional impairment in musician's dystonia.
Stage 0: incapable of playing Stage 1: plays several notes but stops because of blockage or lack of facility Stage 2: plays short sequences without rapidity and with unsteady fingering Stage 3: plays easy pieces but is unable to perform more technically challenging pieces Stage 4: plays almost normally but difficult passages are avoided for fear of motor problems Stage 5: normal playing Source: Tubiana.9
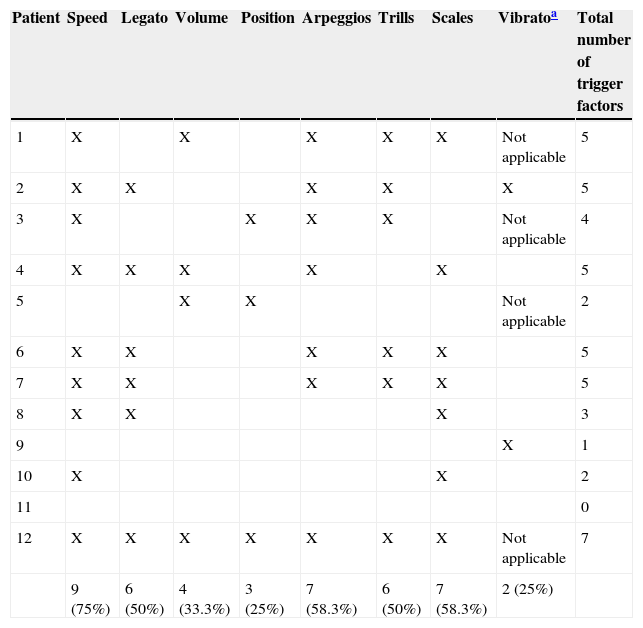
We also described the presence of other factors related to interpretation: playing speed, legato (a style in which no rests are perceived between musical notes), pianissimo (very low volume), pitch (wind instruments only), public performance, alternating repetitive movements involving 3 or more fingers, trills (alternating between 2 fingers), scales (set of notes ordered by pitch), and vibrato (string instruments only).
The patients were treated with non-pharmacological therapy (sensory training, pedagogical retraining, physical rehabilitation) and pharmacological therapy (botulinum toxin or anticholinergics). We recorded type of treatment, treatment duration, and results (assessed on the Tubiana scale).
Statistical dataQuantitative variables are shown as means±SD; ranges are given in brackets. Qualitative variables are expressed as frequencies (percentage of the total is shown in brackets). We used Wilcoxon signed-rank test to compare therapy results. P values <.05 were considered statistically significant.
ResultsDemographic data: mean age was 34.8±11.8 years (range, 20–62); 10 participants were men (83.3%), and 2 were women (16.7%).
Medical history: 4 (33.3%) patients had a history of unrelated disorders (alcoholism, 1; depression, 1; tobacco dependence, 1; surgically treated spontaneous pneumothorax, 1). Six patients (50%) had a history of trauma in the affected segment: repeated shoulder contusions from practising martial arts, 1; lateral epicondylitis, 1; fractured incisor, 1; wrist sprain and fracture, 1; and clavicle fracture, 2.
Six patients had a family history of neurological disorders in first-degree relatives: Alzheimer disease, 2; Parkinson's disease, 1; essential tremor, 2; and writer's cramp, 1.
Employment history: 8 patients (66.6%) were classical musicians, while 4 (33.3%) played popular music. At symptom onset, 4 patients (33.3%) were soloists, 4 patients were accompanists, and 4 were students (2 were university students, 1 studied at a conservatory, and another practised independently).
Classification by instrument type, using the Hornbostel–Sachs system, was as follows: aerophones, 5 patients (clarinet, 2 [16.7%], flute, 1 [8.3%], bandoneon concertina, 2); and chordophones, 7 patients (cello, 2; acoustic guitar, 2; electric guitar, 1; piano, 1; and violin, 1). All participants played a second instrument.
Mean age of beginning music education was 12±3.8 years (range 5–18); mean number of years of education was 18.1±1.4 (range 16–20); and mean number of years playing music was 10.4±5.0 (range 4–21). Participants’ mean daily practice time was 4.3±2hours (range 2–8).
Characterisation of dystonic symptoms: mean age at symptom onset was 28.2±11.3 years (range 18–57). Patients had presented initial symptoms a mean of 6.5±5.8 years (range 0.1–15) before the evaluation was performed.
In 11 patients (91.7%), the affected segment was the hand (the dominant hand in 6 cases), whereas one participant, a clarinet student, presented dystonic symptoms in the mandible and mouth area (embouchure dystonia).
Regarding forms of presentation, the primary symptoms given as the reason for consultation were as follows:
- •
tension or rigidity in the hand or affected segment, 11 patients (91.7%);
- •
loss of hand motor control while playing, 10 patients (83.3%);
- •
slow movement of fingers or the affected segment, 3 patients (25%);
- •
finger tremor in the affected segment, 3 patients (25%);
- •
weakness of the hand or affected segment, 1 patient (8.3%), and
- •
pain in the affected segment, 1 patient.
Five patients (41.7%) experienced tremor at some point during progression of dystonic symptoms.
We classified severity of functional impairment before starting therapy on the Tubiana scale: plays almost normally but difficult passages are avoided for fear of motor problems, 1 patient (8.3%); plays easy pieces but is unable to perform more technically challenging pieces, 5 patients (41.7%); plays short sequences without rapidity and with unsteady fingering, 2 patients; plays several notes but stops because of blockage or lack of facility, 2 patients; and incapable of playing, 2 patients (16.7%).
The triggering factors for dystonic movement specific to playing an instrument are listed in Table 2.
Trigger factors associated with specific requirements of fine motor control among musicians in our series.
| Patient | Speed | Legato | Volume | Position | Arpeggios | Trills | Scales | Vibratoa | Total number of trigger factors |
|---|---|---|---|---|---|---|---|---|---|
| 1 | X | X | X | X | X | Not applicable | 5 | ||
| 2 | X | X | X | X | X | 5 | |||
| 3 | X | X | X | X | Not applicable | 4 | |||
| 4 | X | X | X | X | X | 5 | |||
| 5 | X | X | Not applicable | 2 | |||||
| 6 | X | X | X | X | X | 5 | |||
| 7 | X | X | X | X | X | 5 | |||
| 8 | X | X | X | 3 | |||||
| 9 | X | 1 | |||||||
| 10 | X | X | 2 | ||||||
| 11 | 0 | ||||||||
| 12 | X | X | X | X | X | X | X | Not applicable | 7 |
| 9 (75%) | 6 (50%) | 4 (33.3%) | 3 (25%) | 7 (58.3%) | 6 (50%) | 7 (58.3%) | 2 (25%) |
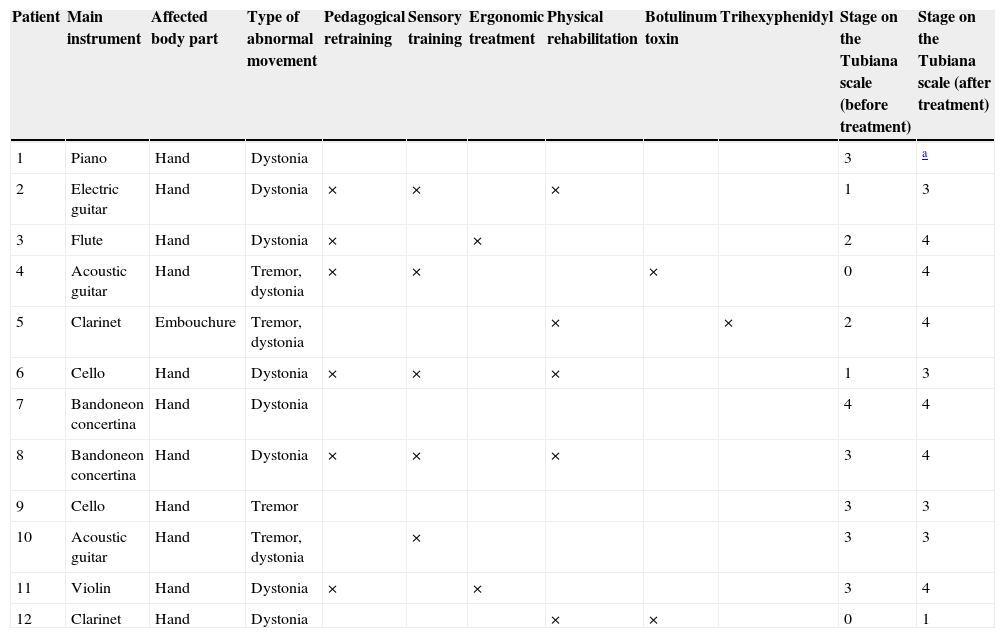
Table 3 summarises the treatment used for each patient. We compared patients’ performance before and after therapy and found considerable improvements as reflected by changes of one or more stages on the Tubiana scale (P<.05). Most of the participants received more than one type of treatment. This multidisciplinary approach involved different non-pharmacological therapies including pedagogical retraining, sensory training, ergonomic treatment, and physical rehabilitation, as previously described in another study.5 Treatment with botulinum toxin was necessary in only 22% of the patients. Fifty percent of the participants were able to continue their professional activity or maintain their position in the orchestra.
Characterisation of dystonic symptoms, treatments used, and scores on the Tubiana scale before and after multidisciplinary therapy in a series of musicians.
| Patient | Main instrument | Affected body part | Type of abnormal movement | Pedagogical retraining | Sensory training | Ergonomic treatment | Physical rehabilitation | Botulinum toxin | Trihexyphenidyl | Stage on the Tubiana scale (before treatment) | Stage on the Tubiana scale (after treatment) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Piano | Hand | Dystonia | 3 | a | ||||||
| 2 | Electric guitar | Hand | Dystonia | × | × | × | 1 | 3 | |||
| 3 | Flute | Hand | Dystonia | × | × | 2 | 4 | ||||
| 4 | Acoustic guitar | Hand | Tremor, dystonia | × | × | × | 0 | 4 | |||
| 5 | Clarinet | Embouchure | Tremor, dystonia | × | × | 2 | 4 | ||||
| 6 | Cello | Hand | Dystonia | × | × | × | 1 | 3 | |||
| 7 | Bandoneon concertina | Hand | Dystonia | 4 | 4 | ||||||
| 8 | Bandoneon concertina | Hand | Dystonia | × | × | × | 3 | 4 | |||
| 9 | Cello | Hand | Tremor | 3 | 3 | ||||||
| 10 | Acoustic guitar | Hand | Tremor, dystonia | × | 3 | 3 | |||||
| 11 | Violin | Hand | Dystonia | × | × | 3 | 4 | ||||
| 12 | Clarinet | Hand | Dystonia | × | × | 0 | 1 |
Focal dystonia has a great impact on musicians’ quality of life and in many cases marks the end of their musical careers. We feel that this issue is insufficiently addressed in most articles about dystonia.
A third of the subjects were not classical musicians but this group accounts for more than 90% of the study population in most articles. This may be due to the fact that those articles are based on samples drawn directly from institutions that train musicians,4,10–13 whereas our centre is open to the general population and has no specific links to any such institutions.
Regarding impact on employment, 50% of participants maintained their professional or student activities, which is coherent with reports in the literature.10,14
We should also highlight the high frequency of histories of trauma to the affected body part; this finding has also been reported in several other studies.15–17 In addition to the above, half of the subjects had a first-degree relative with a neurological disorder (extrapyramidal disorders in two-thirds of these cases). In fact, several genetic studies have suggested that musician's dystonia has a genetic component.18,19
Our data characterising the condition coincide with those from previous series in terms of symptom distribution by affected finger (hand dystonia) and percentage of patients with embouchure dystonia.4,12 We must point out that musicians in our series play a second instrument, which some authors have highlighted as a risk factor for focal dystonia.20 We should also mention that all musicians in our series reported at least one triggering factor pertaining to playing music, and most of these factors were movements requiring an extreme degree of motor control. However, most descriptive studies do not address this issue in depth.5,7,12,21
Regarding treatment response, all treated subjects experienced improvements in musical performance (according to the Tubiana scale); however, these gains did not necessarily deliver improvements in the workplace, and only 50% of musicians under treatment maintained the positions they had held at symptom onset. Since the present study is an open study, our findings should be compared to those from studies featuring blinded evaluators.7,11,22–28
In conclusion, most of our findings regarding dystonia description, medical comorbidities, and employment history are consistent with reports in the literature. However, we wish to highlight the involvement of trigger factors linked to the specific requirements of playing music and fine motor control (playing speed, trills, vibrato, etc.). This is consistent with sensorimotor integration and inhibitory control alterations described in this disorder,29,30 and it may be especially relevant for selecting repertoire to be played during the musician's rehabilitation. When patients are students, this may require cooperation from their teachers. While selection of repertoire is unlikely to be immediately addressed in the rehabilitation process, we find that this issue arises frequently among student musicians, and will invariably require therapeutic decision-making.
Conflict of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Aránguiz R, Chana-Cuevas P, Alburquerque D, Curinao X. Distonía del músico: fenomenología y desencadenantes vinculados a la ejecución musical. Neurología. 2015;30:270–275.
