



The marked heterogeneity among children diagnosed with specific language impairment (SLI) highlights the importance of studying and describing cases based on the distinction between the expressive and receptive-expressive SLI subtypes. The main objective of this study was to examine neuropsychological, linguistic, and narrative behaviours in children with different SLI subtypes.
MethodA comprehensive battery of language and neuropsychological tests was administered to a total of 58 children (29 with SLI and 29 normal controls) between 5.60 and 11.20 years old.
ResultsBoth SLI subtypes performed more poorly than the control group in language skills, narrative, and executive function. Furthermore, the expressive SLI group demonstrated substantial ungrammaticality, as well as problems with verbal fluency and both verbal and spatial working memory, while the receptive-expressive SLI subtype displayed poorer neuropsychological performance in general.
ConclusionsOur findings showed that children with either SLI subtype displayed executive dysfunctions that were not limited to verbal tasks but rather extended to nonverbal measures. This could reflect a global cognitive difficulty which, along with declining linguistic and narrative skills, illustrates the complex profile of this impairment.
La heterogeneidad existente entre los niños diagnosticados con trastorno específico del lenguaje (TEL) enfatiza la necesidad de su estudio y caracterización a partir de la distinción entre los subtipos TEL-expresivo y TEL-expresivo-receptivo. El principal objetivo de esta investigación ha sido estudiar el rendimiento neuropsicológico, lingüístico y narrativo en distintos subtipos de niños con TEL.
MétodoUn protocolo de evaluación exhaustiva tanto de funciones lingüísticas como neuropsicológicas se administró a un total de 58 niños (29 TEL y 29 con desarrollo típico) entre los 5,60 y los 11,20 años de edad.
ResultadosAmbos subtipos de TEL obtuvieron peores resultados que el grupo control en las habilidades de lenguaje, en narración y en funcionamiento ejecutivo. Además, el subtipo TEL-expresivo evidenció una elevada presencia de agramaticalidad así como de problemas en la fluidez verbal y en memoria de trabajo verbal y espacial, mientras que el subtipo TEL-expresivo-receptivo obtuvo, en general, un peor rendimiento neuropsicológico.
ConclusionesNuestros hallazgos muestran como los niños de ambos subtipos de TEL tienen disfunciones ejecutivas que no se reducen a las tareas verbales sino que se extienden a las medidas no verbales. Todo ello podría reflejar una dificultad cognitiva general que, junto con un deterioro lingüístico y narrativo, confiere un perfil complejo a este trastorno.
Specific language impairment (SLI) is defined as a significant alteration in the acquisition and execution of language, in the context of appropriate sensory and brain development with no deficits in either intellectual ability or linguistic stimulation. However, mounting empirical evidence shows that symptoms in this patient population are highly heterogeneous. Therefore, a better methodological approach for characterising SLI might consist of analysing it by subtype. This methodology is supported by both psycholinguistics and neuropsychology, and it would probably reveal diverse anatomopathological substrates for each of the different subtypes.
Executive functions (EF) are defined as a group of mechanisms related to the optimisation of the cognitive processes aimed at resolving complex or new situations. They involve such functions as volition, working memory, planning, purposive action, and effective performance. Carrying out EF depends on the anatomo-functional integrity of the frontal cortex and its connections. Although the literature suggests that children with SLI may experience difficulties in several components of executive performance,11 results are not consistent between studies; most depict SLI as a simple entity, without considering its heterogeneity. Therefore, the related studies of SLI subgroups and how they are linked to neuropsychological performance of executive functions will probably provide more in-depth knowledge of the pathophysiology of this disorder.
Children with SLI typically manifest deficits in narrative abilities. In this context, one proposed explanation of the underlying aetiology is cognitive changes, referring more specifically to the executive function disorders identified in this population.2 Some studies have shown that working memory is an essential mechanism that keeps relevant aspects of narratives active and available in the mind3; others point to the main role of attention, cognitive flexibility, inhibitory control, and planning skills in lending coherence and cohesion to stories.4
The profile of SLI underlines the need for early identification of children with the disorder, and for interventions directed at the cognitive domains with deficits. These actions would place us at a vantage point for preventing future alterations in the acquisition of basic instrumental skills, such as reading, and therefore prove beneficial for the self-esteem of these children. A recent groundbreaking study in this area has used questionnaires to assess self-perception in children with SLI, as well as how their parents perceive them.5 Using the Paediatric Quality of Life Inventory (PedsQL), the authors concluded that children with SLI perceive themselves as having altered physical and social functioning, whereas parents describe them as having social difficulties but no physical problems. This article produces scientific evidence of the need to mitigate other disturbances that may affect the population with SLI concomitantly if they are not treated in time.
In light of the above, we designed our study to analyse the differences between 2 SLI subtypes and how they may affect narrative tasks and executive functions in patients. We proposed the following objectives: first, we aimed to analyse links between each group (receptive/expressive developmental language disorder [RE-SLI], expressive language disorder [E-SLI], and control) and the diverse linguistic tests that help us identify SLI. These tests examine phonological and lexical-semantic tasks, and linguistic expression and comprehension processes. Second, we examined the relationship between the different subgroups and narrative performance. Lastly, we studied executive functioning in each of the study groups.
MethodsSelection and characteristics of participantsWe included 29 schoolchildren diagnosed with SLI and 29 children with normal language development (control group). The group with SLI included 23 boys and 6 girls aged between 5.60 and 11.20 years (mean age [M]=7.90, standard deviation [SD]=1.52). The control group was made up of 20 boys and 9 girls aged between 5.90 and 11.20 years (M=8.54; SD=1.54). The experimental group was also divided into 2 subtypes (ER-SLI and E-SLI), in line with a previous study.6 The first subgroup (ER-SLI) included 16 of the children with SLI (12 boys and 4 girls), aged 5.90 to 11.20 years (mean age [M]=7.98, standard deviation [SD]=1.30); the second subgroup (E-SLI) contained the remaining 13 children (11 boys and 2 girls) aged 5.90 to 11.10 years (M=7.79; SD=1.81). We used the Kolgomorov–Smirnov test to check for normal distribution of age (z=0.85; P=.472), and performed a contrast to analyse between-group differences in age (F2,55=1.57; P=.218). As a previous step, homogeneity of variance had been determined using the Levene test (F2,55=0.90; P=.414).
Tools for identifying children with specific language impairmentWe used 3 tests to diagnose SLI. Firstly, we administered the most internationally used test for the analysis of this disorder, known as CELF-3.7 This screening test evaluates overall linguistic comprehension and expression processes using tasks assessing sentence structure, sentence formulation, concepts and directions, word structure and class, and recall of sentences. Children with SLI obtain mean scores below −1.25 standard deviations. We also used the Peabody test8 to measure vocabulary and the auditory and visual association subtests of the Illinois Test of Psycholinguistic Abilities (ITPA)9 to evaluate semantic psycholinguistic processes. Lastly, we verified that children with SLI had a non-verbal IQ > 85 as measured by the Kaufman brief intelligence test (K-BIT).10 The first group (ER-SLI) presented an IQ range from 86 to 121 (M=104; SD=10) and the second group (E-SLI), from 86 to 115 (M=100; SD=8). The control group showed a range from 90 to 127 (M=109; SD=11). We used the Kolgomorov–Smirnov test to check for normal distribution of IQ (z=0.97; P=.266). To determine whether IQs were similar among groups, we tested for homogeneity of variances (F2,55=1.71; P=.190) and performed a contrast (F2,55=4.05; P=.024); results showed intergroup heterogeneity. For this reason, we included non-verbal IQ as a covariable in the model. Since it did not affect any of the contrasts performed, we therefore excluded it from the final contrasts.
Procedure for assessing narrative abilitiesOnce children were diagnosed with SLI, we assessed their narrative abilities. In the assessment, children were asked to tell the story from the picture book Frog, where are you?.11 After literal transcription, we analysed problems in sentence formulation and speech fluency (mazes), as well as grammatical errors.
Procedure for assessing executive functionsThe neuropsychological protocol for the assessment of executive functions included the following tests:
Evaluation of verbal working memory. Digit subtest.12 This listening test presents increasingly difficult sequences of digits which the participant has to repeat both forward and backward.
Evaluation of spatial working memory. Spatial span test (WMS-III). This test is a visuospatial version of the span test created by Wechsler in the third edition of his memory scale.13 It has a direct and inverse version.
Evaluation of verbal fluency. We assessed verbal fluency using the Controlled Oral Word Association Test (COWAT) by Benton and Hamsher.14 The participant is asked to list as many words as possible starting with a given letter (F, A, S), or belonging to the semantic category ‘animal’. The time limit for each task is one minute.
Evaluation of design fluency. Design fluency test included in the NEPSY test battery (A Developmental Neuropsychological Assessment).15 Using a template featuring squares containing 5 dots each, the participant is given one minute in which to create different designs by connecting at least 2 dots. It has a structured version and a randomised version.
Planning assessment. Rey-Osterrieth Complex Figure.16 This test assesses visuoperceptual and visuoconstructive skills. Furthermore, the copy produced by the test subject provides a reasonable measure of that subject's level of planning. The test presents a complex geometrical drawing which is not related to any other familiar figure. The participant is asked to copy the drawing, and then to reproduce it from memory after 3 minutes, and then after 30 minutes.
Evaluation of inhibition and cognitive flexibility. Five digit test.17 The test presents 4 different situations in increasing order of difficulty. In each of these situations, the participant is shown a card with 50 stimuli grouped in 5 columns containing 10 rows. Stimuli are groups of asterisks or digits enclosed in small rectangles. The 4 assessment situations are reading, counting, choosing, and switching. The method of administration enables the generation of an inhibition index and a flexibility index.
Design and procedureThe study's experimental design assigned participants to 3 groups (ER-SLI, E-SLI, and control). Dependent variables were determined by participants’ results on all administered tests.
ResultsWe first checked each variable in our experimental model for normal distribution, and made the appropriate changes when variables showed an abnormal distribution. Lastly, to simplify the interpretation of the magnitude of differences, all variables were transformed into T-scores (M=50, SD=10). We conducted analysis of variance for each variable in order to identify potential differences between groups. We used the Scheffé test as post hoc contrast test in order to identify any significant differences between means.
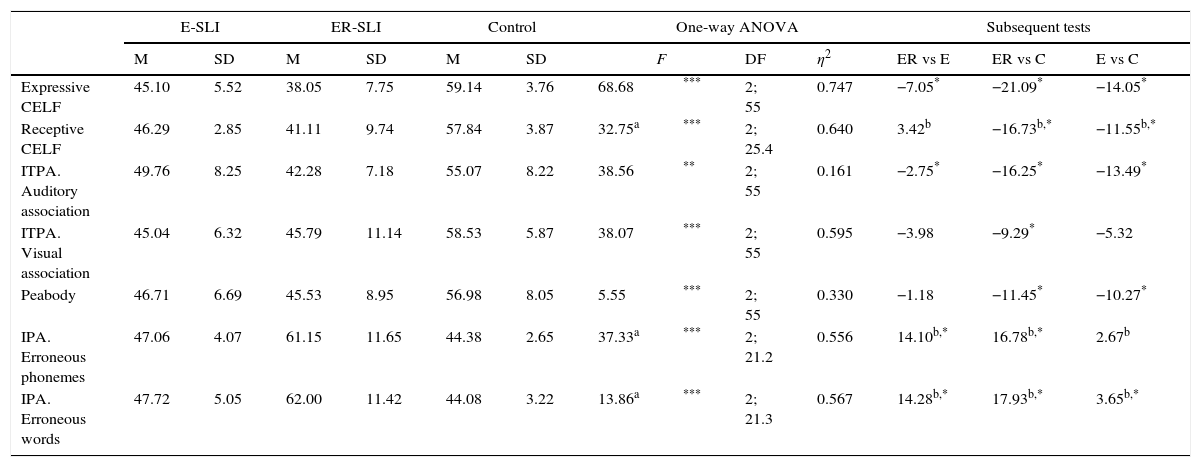
Diagnostic evaluation testsResults obtained with the different instruments are listed in Table 1.
Results on diagnostic assessment tests by group.
| E-SLI | ER-SLI | Control | One-way ANOVA | Subsequent tests | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | F | DF | η2 | ER vs E | ER vs C | E vs C | ||
| Expressive CELF | 45.10 | 5.52 | 38.05 | 7.75 | 59.14 | 3.76 | 68.68 | *** | 2; 55 | 0.747 | −7.05* | −21.09* | −14.05* |
| Receptive CELF | 46.29 | 2.85 | 41.11 | 9.74 | 57.84 | 3.87 | 32.75a | *** | 2; 25.4 | 0.640 | 3.42b | −16.73b,* | −11.55b,* |
| ITPA. Auditory association | 49.76 | 8.25 | 42.28 | 7.18 | 55.07 | 8.22 | 38.56 | ** | 2; 55 | 0.161 | −2.75* | −16.25* | −13.49* |
| ITPA. Visual association | 45.04 | 6.32 | 45.79 | 11.14 | 58.53 | 5.87 | 38.07 | *** | 2; 55 | 0.595 | −3.98 | −9.29* | −5.32 |
| Peabody | 46.71 | 6.69 | 45.53 | 8.95 | 56.98 | 8.05 | 5.55 | *** | 2; 55 | 0.330 | −1.18 | −11.45* | −10.27* |
| IPA. Erroneous phonemes | 47.06 | 4.07 | 61.15 | 11.65 | 44.38 | 2.65 | 37.33a | *** | 2; 21.2 | 0.556 | 14.10b,* | 16.78b,* | 2.67b |
| IPA. Erroneous words | 47.72 | 5.05 | 62.00 | 11.42 | 44.08 | 3.22 | 13.86a | *** | 2; 21.3 | 0.567 | 14.28b,* | 17.93b,* | 3.65b,* |
SD: standard deviation; DF: degree of freedom; M: mean.
The Bonferroni correction was used to assess the significance of post hoc contrasts (P<.05).
In the diagnostic evaluation, we observed significant differences for all tests administered, and examined them using a post hoc contrast test. Results showed that the control group performed significantly better on all tests than the ER-SLI group did. Furthermore, the control group showed significantly better performances than the E-SLI group on all tests, except for the visual association test (ITPA) and erroneous phonemes (induced phonological assessment, IPA). Comparing the 2 groups with SLI only revealed significant differences in performance on the IPA, expressive CELF, and auditory association subtests of ITPA; the ER-SLI group registered poorer performance on all tests.
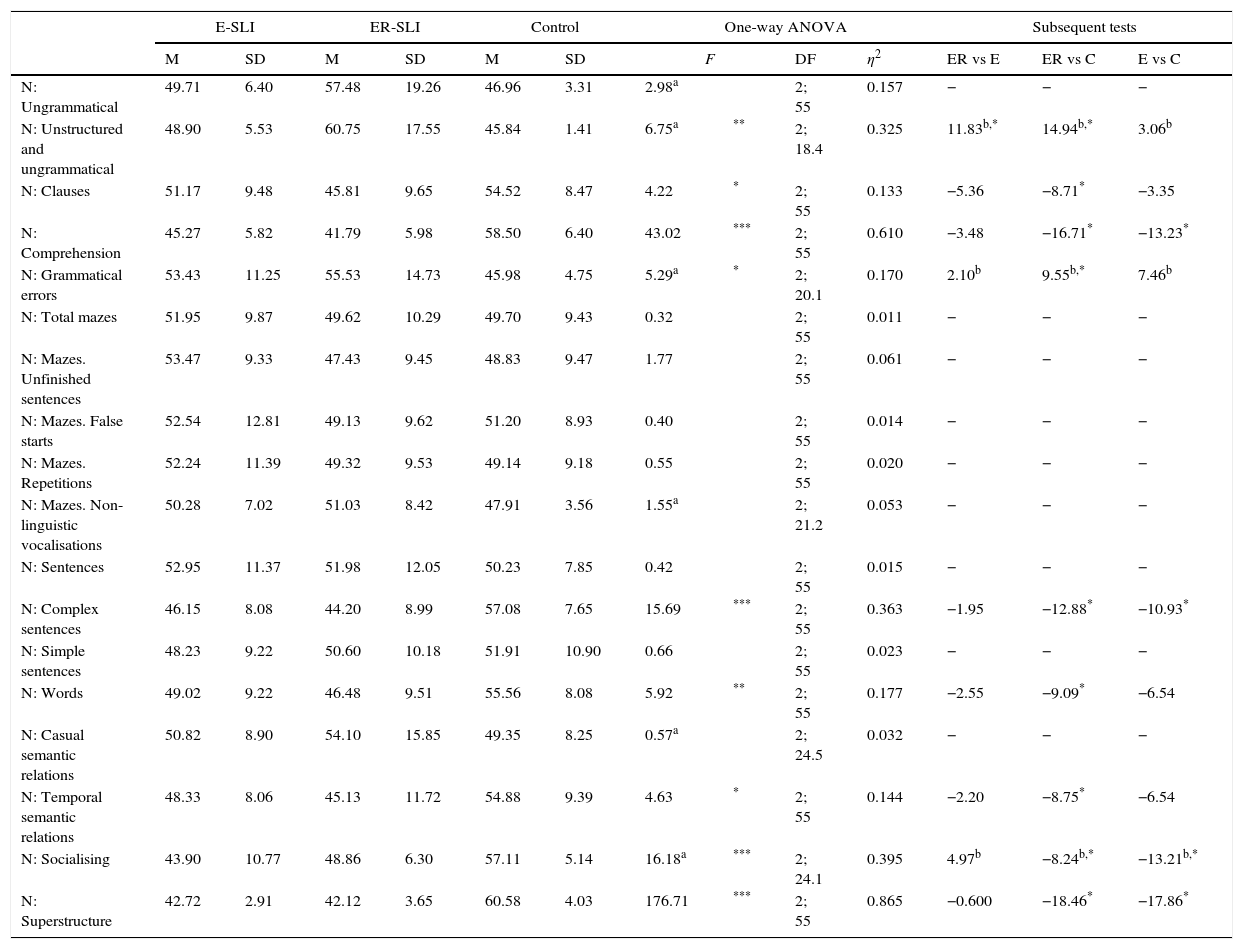
Narrative tasksThe results obtained for each of the different narrative tasks are listed in Table 2.
Results on narrative tasks (N) per group.
| E-SLI | ER-SLI | Control | One-way ANOVA | Subsequent tests | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | F | DF | η2 | ER vs E | ER vs C | E vs C | ||
| N: Ungrammatical | 49.71 | 6.40 | 57.48 | 19.26 | 46.96 | 3.31 | 2.98a | 2; 55 | 0.157 | − | − | − | |
| N: Unstructured and ungrammatical | 48.90 | 5.53 | 60.75 | 17.55 | 45.84 | 1.41 | 6.75a | ** | 2; 18.4 | 0.325 | 11.83b,* | 14.94b,* | 3.06b |
| N: Clauses | 51.17 | 9.48 | 45.81 | 9.65 | 54.52 | 8.47 | 4.22 | * | 2; 55 | 0.133 | −5.36 | −8.71* | −3.35 |
| N: Comprehension | 45.27 | 5.82 | 41.79 | 5.98 | 58.50 | 6.40 | 43.02 | *** | 2; 55 | 0.610 | −3.48 | −16.71* | −13.23* |
| N: Grammatical errors | 53.43 | 11.25 | 55.53 | 14.73 | 45.98 | 4.75 | 5.29a | * | 2; 20.1 | 0.170 | 2.10b | 9.55b,* | 7.46b |
| N: Total mazes | 51.95 | 9.87 | 49.62 | 10.29 | 49.70 | 9.43 | 0.32 | 2; 55 | 0.011 | − | − | − | |
| N: Mazes. Unfinished sentences | 53.47 | 9.33 | 47.43 | 9.45 | 48.83 | 9.47 | 1.77 | 2; 55 | 0.061 | − | − | − | |
| N: Mazes. False starts | 52.54 | 12.81 | 49.13 | 9.62 | 51.20 | 8.93 | 0.40 | 2; 55 | 0.014 | − | − | − | |
| N: Mazes. Repetitions | 52.24 | 11.39 | 49.32 | 9.53 | 49.14 | 9.18 | 0.55 | 2; 55 | 0.020 | − | − | − | |
| N: Mazes. Non-linguistic vocalisations | 50.28 | 7.02 | 51.03 | 8.42 | 47.91 | 3.56 | 1.55a | 2; 21.2 | 0.053 | − | − | − | |
| N: Sentences | 52.95 | 11.37 | 51.98 | 12.05 | 50.23 | 7.85 | 0.42 | 2; 55 | 0.015 | − | − | − | |
| N: Complex sentences | 46.15 | 8.08 | 44.20 | 8.99 | 57.08 | 7.65 | 15.69 | *** | 2; 55 | 0.363 | −1.95 | −12.88* | −10.93* |
| N: Simple sentences | 48.23 | 9.22 | 50.60 | 10.18 | 51.91 | 10.90 | 0.66 | 2; 55 | 0.023 | − | − | − | |
| N: Words | 49.02 | 9.22 | 46.48 | 9.51 | 55.56 | 8.08 | 5.92 | ** | 2; 55 | 0.177 | −2.55 | −9.09* | −6.54 |
| N: Casual semantic relations | 50.82 | 8.90 | 54.10 | 15.85 | 49.35 | 8.25 | 0.57a | 2; 24.5 | 0.032 | − | − | − | |
| N: Temporal semantic relations | 48.33 | 8.06 | 45.13 | 11.72 | 54.88 | 9.39 | 4.63 | * | 2; 55 | 0.144 | −2.20 | −8.75* | −6.54 |
| N: Socialising | 43.90 | 10.77 | 48.86 | 6.30 | 57.11 | 5.14 | 16.18a | *** | 2; 24.1 | 0.395 | 4.97b | −8.24b,* | −13.21b,* |
| N: Superstructure | 42.72 | 2.91 | 42.12 | 3.65 | 60.58 | 4.03 | 176.71 | *** | 2; 55 | 0.865 | −0.600 | −18.46* | −17.86* |
SD: standard deviation; DF: degree of freedom; M: mean.
The Bonferroni correction was used to assess the significance of post hoc contrasts (P<.05).
No significant differences were observed for any of the following skills: mazes, casual semantic relations, total number of sentences, number of simple sentences, and number of ungrammatical sentences. We assessed the differences in the remaining narrative tasks using a post hoc contrast test. Results showed that the control group performed significantly better on all tasks compared to the ER-SLI group. Furthermore, the control group only displayed a significantly better performance than that of E-SLI in superstructure, number of complex sentences, socialising, and comprehension tasks. In any case, and despite the lack of sentence length or syntactic complexity measurements, a detailed analysis of the data included in Table 2 shows that both groups of children with SLI obtain poorer results for complex syntax. In other words, these patients construct more ungrammatical sentences and make more grammatical errors, and a higher number of simple sentences than complex sentences. Comparison between the 2 SLI groups revealed significant differences only in the number of unstructured and ungrammatical errors, with poorer performance by the group with ER-SLI.
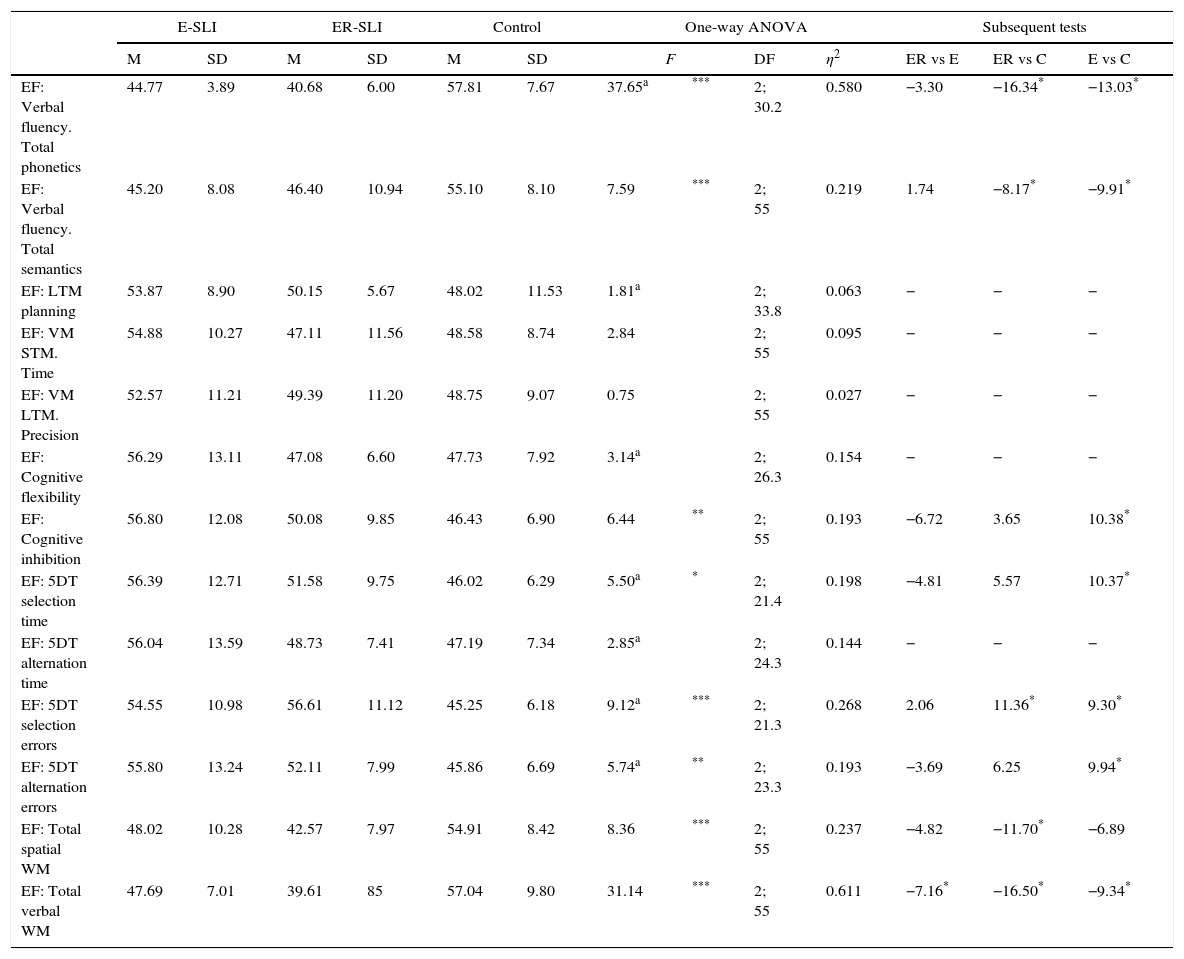
Executive function tasksThe results obtained on the different executive function tasks are given in Table 3.
Results for executive functions by group.
| E-SLI | ER-SLI | Control | One-way ANOVA | Subsequent tests | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | F | DF | η2 | ER vs E | ER vs C | E vs C | ||
| EF: Verbal fluency. Total phonetics | 44.77 | 3.89 | 40.68 | 6.00 | 57.81 | 7.67 | 37.65a | *** | 2; 30.2 | 0.580 | −3.30 | −16.34* | −13.03* |
| EF: Verbal fluency. Total semantics | 45.20 | 8.08 | 46.40 | 10.94 | 55.10 | 8.10 | 7.59 | *** | 2; 55 | 0.219 | 1.74 | −8.17* | −9.91* |
| EF: LTM planning | 53.87 | 8.90 | 50.15 | 5.67 | 48.02 | 11.53 | 1.81a | 2; 33.8 | 0.063 | − | − | − | |
| EF: VM STM. Time | 54.88 | 10.27 | 47.11 | 11.56 | 48.58 | 8.74 | 2.84 | 2; 55 | 0.095 | − | − | − | |
| EF: VM LTM. Precision | 52.57 | 11.21 | 49.39 | 11.20 | 48.75 | 9.07 | 0.75 | 2; 55 | 0.027 | − | − | − | |
| EF: Cognitive flexibility | 56.29 | 13.11 | 47.08 | 6.60 | 47.73 | 7.92 | 3.14a | 2; 26.3 | 0.154 | − | − | − | |
| EF: Cognitive inhibition | 56.80 | 12.08 | 50.08 | 9.85 | 46.43 | 6.90 | 6.44 | ** | 2; 55 | 0.193 | −6.72 | 3.65 | 10.38* |
| EF: 5DT selection time | 56.39 | 12.71 | 51.58 | 9.75 | 46.02 | 6.29 | 5.50a | * | 2; 21.4 | 0.198 | −4.81 | 5.57 | 10.37* |
| EF: 5DT alternation time | 56.04 | 13.59 | 48.73 | 7.41 | 47.19 | 7.34 | 2.85a | 2; 24.3 | 0.144 | − | − | − | |
| EF: 5DT selection errors | 54.55 | 10.98 | 56.61 | 11.12 | 45.25 | 6.18 | 9.12a | *** | 2; 21.3 | 0.268 | 2.06 | 11.36* | 9.30* |
| EF: 5DT alternation errors | 55.80 | 13.24 | 52.11 | 7.99 | 45.86 | 6.69 | 5.74a | ** | 2; 23.3 | 0.193 | −3.69 | 6.25 | 9.94* |
| EF: Total spatial WM | 48.02 | 10.28 | 42.57 | 7.97 | 54.91 | 8.42 | 8.36 | *** | 2; 55 | 0.237 | −4.82 | −11.70* | −6.89 |
| EF: Total verbal WM | 47.69 | 7.01 | 39.61 | 85 | 57.04 | 9.80 | 31.14 | *** | 2; 55 | 0.611 | −7.16* | −16.50* | −9.34* |
SD: standard deviation; EF: executive function; DF: degree of freedom; M: mean; WM: working memory; VM: verbal memory; STM: short term memory; LTM: long term memory.
The Bonferroni correction was used to assess the significance of post hoc contrasts (P<.05).
Regarding executive functions, we did not find significant differences in visuoperceptual memory, planning, long-term memory, short-term visual memory (time), long-term visual memory (precision), cognitive flexibility, or in shifting time. We completed a post hoc contrast test of the differences in the remaining executive function tasks. Results showed that the control group performed significantly better than the E-SLI group on all tasks, with the exception of spatial working memory. Furthermore, the control group only displayed a significantly better performance than the ER-SLI on the 2 verbal fluency subtests, selection error tasks, and for the 2 types of working memory. Comparing the 2 groups with SLI revealed significant differences in verbal working memory, with poorer performance by the group with ER-SLI.
DiscussionConsidering SLI an homogeneous nosological entity does not fully explain the classic and characteristic symptoms identified in this population. A better methodological approach would entail classifying this disease in at least 2 subtypes, ER-SLI and E-SLI. This was the main focus of our study. We believe that our results provide more detailed knowledge of the ER-SLI and E-SLI subtypes in the context of linguistic and narrative skills and executive functions. Regarding linguistic skills, we observed significant differences among the 3 study groups. We subsequently observed that the control group performed significantly better than the 2 groups with SLI subtypes for all language-related skills. However, comparing the 2 SLI subtype groups revealed differences in language expression (expressive CELF), speech (IPA), and auditory association (ITPA). In all cases, performance was much worse in the ER-SLI group. The language expression problems displayed by the ER-SLI subgroup may be explained by their difficulties associating terms with a given word. This causes severe difficulties with syntax and meaning retrieval with a negative impact on access to words used to express meanings.6
When we compare narrative skills between the ER-SLI and E-SLI groups, we observe a significant difference in grammatical correctness, and more specifically in sentence structuring ability. We therefore believe that ER-SLI is characterised by grammatical problems manifesting as severe irregularities in the use and understanding of grammatical structures. Impairment seems to transcend grammatical morphology since it also affects the sequential order of sentences. In other words, it manifests as a severe deficit in establishing dependency within the morphosyntactic system. This may lead to inconsistent creation and/or use of morphosyntactic structures, especially those involving dependent relationships between syntactic elements. Consequently, children with this subtype may make use of other types of non-syntactic signals (probably lexical and pragmatic) to interpret the meaning of sentences.18
The most interesting data regarding executive functions derive from the comparison of the 2 SLI subtypes. We are able to conclude that ER-SLI patients present poorer executive performance, mainly involving more severe working memory impairment, with negative consequences not only for language expression, but also for understanding more complex language.2 Considering the type of task used to evaluate verbal working memory (digits), the component for temporary storage of verbal information is what appears to be impaired, and not the central executive component of working memory.19
Our study's data set relating to narrative production and comprehension deficits, and to the series of dysfunction in these patients’ executive functioning, also raises some key questions.1 The role of verbal working memory in narrative tasks seems clear: this type of memory keeps the relevant information active and available for use when recounting a story. Therefore, impairment of this type of working memory creates difficulties for ER-SLI and E-SLI patients when they have to perform narrative tasks.3 In the same way, working memory is essential for narrative tasks since it lets listeners retain the information they hear, and link it to their knowledge of the real world which is a more important step. Since Baddeley's creation of the working memory model, which includes a device which regulates temporary storage of episodic memory by integrating, manipulating, and making it available, working memory has been considered an essential skill for understanding narratives.
Our findings suggest that children with SLI present executive dysfunctions affecting both verbal and non-verbal tasks. All this may point to overall cognitive impairment. These results are compatible with alterations in the prefrontal cortex and the cortico-cortical and cortical-subcortical connections that this structure maintains for executive functioning. In any case, future studies in this area should investigate the precise association between the different components which make up the working memory construct and the specific linguistic difficulties present in children with SLI. A recently published study by Vugs et al.19 shows that the elements best explaining the relationship between working memory and linguistic deficits in SLI are the central executive and verbal storage components.
We believe that our data underscore the need for therapeutic rehabilitation programmes including not only intensive training of psycholinguistic skills but also interventions aimed at developing neuropsychological functions, and especially executive performance.
FundingThe study has been funded by the Spanish Ministry of Economy and Competitiveness. Research project: “Funciones ejecutivas y lenguaje en alumnado con TEL. Un modelo de evaluación e intervención con bases psicolingüística y neuropsicológica”. Reference EDU2011-27789.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Acosta Rodríguez V, Ramírez Santana GM, Hernández Expósito S. Funciones ejecutivas y lenguaje en subtipos de niños con trastorno específico del lenguaje. Neurología. 2017;32:355–362.
