




Objective: to determine the association between smoking, depression and suicide risk in the Nursing Staff of a University Hospital.
Materials and method: this was a non-experimental, correlational cross-range study with observational analysis carried out between May 2012 and May 2013. We studied 232 nurses of the "Dr. José Eleuterio González" University Hospital.
Two self-administered scales were applied, one for depression and one for suicide risk. Another hetero-applied scale of nicotine dependency was also used, and the subjects' socio-demographic records were reviewed.
Results: A total of 527,232 nurses were studied. A smoking prevalence of 22.8% (53 subjects), an operational depression prevalence of 15.1% (35 subjects), and a suicide risk of 5.1% (12 subjects) were found.
Gender and age, specifically being male and young (mean age 29.2 years) were found to increase the risk of smoking. We also found that those nurses who had a partner and had a higher level of education smoked less compared to those who did not have a partner or had a lower degree of education. There were hospital departments where there was a higher prevalence of smoking, such as Internal Medicine and Shock trauma. No association between smoking and the presence of depression was found.
Regarding depression, we found that those nurses who worked in the Department of Pensioners were more likely to develop operational depression than those working in any other department. We also found that the risk of presenting operational depression decreases as age increases. About suicide risk, a statistically significant association between smoking and suicide risk was found. We also found an association between operational depression and suicide risk.
Conclusions: It is recommended to consider nicotine dependence as a fundamental part of psychopathology assessment because of its strong association with suicide risk. This study emphasizes the complexity of the issue of the comorbidity of smoking and psychopathology and the need to continue research lines.
Introduction
Smoking is a risk factor for over 20 disease groups, and it's the number one cause of avoidable death.1 tobacco addiction is one of the main causes of morbidity and impaired quality of life. There is a strong connection between smoking and neurological and psychiatric disorders such as depression, schizophrenia, Parkinson's and Alzheimer's diseases.2 In Mexico there is a higher prevalence of smoking among health professionals (31.6%) in comparison with professionals in other fields (23.5%). There are reports in which 29.3% of the Nursing Staff was found to smoke.3
Depression is a syndrome characterized by a drop in mood, self-esteem, ability to experience pleasure with emotional, ideative, conductual and cognitive demonstrations; with serious repercussions on quality of life, social and work performance.4 It is the main cause of disability worldwide; it is considered that by the year 2020 it will be the second cause in absence from work in developed countries.2
The nursing profession is potentially stressing, amid health professions it is considered to be amongst the top ones causing fatigue, trouble sleeping, substance abuse and psychiatric morbidities such as depression.5
Depression risk factors for health professionals are: Working with terminally-ill patients, interpersonal problems with coworkers, clinical competition, fear of failure and excessive and demanding work.6 Working in areas with high work demand, little autonomy and monotony have been associated with depression.7 the stress level in nursing is displayed with absences from work, depression, strong smoking habits, or Burnout Syndrome.8 Other risk factors are extended work shifts, work overload, difficulty of working under optimal time and equipment and personnel conditions, in addition to rotating schedules and night shifts.5,9,10
Suicide is a public health problem. Depression is considered a common cause; around 75% of the people who commit suicide suffer from depression. The majority of suicides are not impulsive, those who attempt it do it after failed attempts at seeking help; therefore, there is not enough time to help the victim.11
A strong link between smoking and depression has been observed. We understand that people with a history of depression are more prone to smoke; depressive symptoms that occur during abstinence are reversible with reinitiation of smoking.2 However, there is little evidence that talks about the mechanism influencing this link. There are 2 possible mechanisms:12 depression causes smoking because the individuals with symptoms smoke as a self-medication to reduce their depressive mood2,12 or depression develops from the neurochemical changes caused by smoking. The common factor: both pathologies share genetic and environmental factors which independently increase the risk of both conditions.12
Women who smoke are twice as likely to present depressive symptoms, compared to those who do not smoke, and five times more than men. Men who smoke more than a pack a day, have a 500% higher possibility of presenting depressive symptoms compared to those who do not smoke. Those who used to smoke or who currently smoke, have a higher possibility of presenting depression compared to those who have never smoked.13 the Nursing Staff of a hospital is a specific population that simultaneously consumes tobacco and has a risk of presenting depressive episodes and suffering the consequences from a depressive disease, interfering with their work, impairing their development and performance, and with irreparable repercussions such as suicide, therefore justifying the need for studies to have a better understanding of its characteristics in order to develop integral strategies and treatments specifically for this population. The purpose of this study is to determine the connection between smoking, depression and risk of suicide in the Nursing Staff of the "Dr. José Eleuterio González" University Hospital.
Materials and method
This was a non-experimental, correlational cross-range study with observational analysis. We requested authorization from the Hospital administration and Head of Nursing to obtain a list of the Nursing Staff, and with an error margin of 5% we calculated our sample in 232 nurses. We randomly selected the subjects from the Nursing Staff in all of the hospital's areas and services. We invited them to voluntarily participate and asked them to sign an informed consent form. We applied 3 scales and a socio-demographic profile.
The scales we used were:
1. Zung Self-Rating Depression Scale: this scale was used to determine the prevalence of depression in the Nursing Staff. It may be applied and scored in a few minutes, and is drafted in simple language, including 20 phrases using a 4-point Likert scale. One of the statements in the scale is: "I feel down and sad, I feel that people around me would be better if I died". In this study we denominated operative depression to the mood disorder detected in the Zung Scale if the subject scored 36 or higher. The scale has a sensitivity of 85% and specificity of 75% when applied for case detection in a clinical population or the general population.
2. Plutchik Suicide Risk Scale: Designed to evaluate the risk of suicide, it is a self-rating tool. It consists of 15 items to which the subject may answer "yes" or "no". It includes questions about previous autolytic attempts, current suicidal ideation intensity and feelings of depression and despair. Some of the questions are: "Have you ever thought about ending your life?" Scoring is obtained by adding all the points and may go from 0 to 15 points. Authors propose a cutoff point of 6. It has been used to determine risk of suicide in Nursing Staff.
3. Fagerström test: It is a hetero-administered scale which assesses nicotine dependency in people. It consists of 6 items with a series of answers associated with a numeric value; values obtained in each one of them are added. A subject is considered to have low dependence with a score of 0-4, medium dependence with a score of 5-6, and high dependence with a score of 7-10. It was used to determine the correlation between nicotine and depressive symptomatology.
4. Socio-demographic profile: We asked about gender, age, marital status, schooling, source of economic support, current pregnancy, number of children, area/department of work, and shift the Nursing Staff was on.
Ethical Considerations
We contacted the members of the Nursing Staff who we detected to have severe depressive symptoms or a high risk of suicide; in order to secure their confidentiality, we contacted them personally through the phone, and we informed them how to make a free appointment in the Psychiatry Department.
The descriptive as well as the inferential statistical analysis was performed using SPSS® Statistics version 13. The categorical variables were obtained through absolute, proportional and percentage frequencies, while continuous numerical variables measurements of central tendency, variability and positioning were calculated. There were 2 types of estimates in this study, the point and the interval estimates, with a 95% confidence interval In order to achieve the study objectives and prove the hypothesis, we obtained chi-square tests for contingency charts and adjusted the logistic regression models.
Within the logistic regression model's adjustment, we considered as a complete model the one that included independent variables: shift (morning, afternoon, pilot, night), gender (male and female), source of economic support (personal, partner and/or shared), smoker (yes and no), marital status (with a partner, without a partner), Department (pensioner and rest), down mood (short period of time and another), and age in years. We implemented backward selection and obtained the best model to describe the behavior of the probability that Nursing Staff indicates operative depression (table 1). In a similar way, we worked to model the probability of the presence of suicidal thoughts (table 2).
Results
1. Sample characteristics
Of the 232 subjects, 193 (83.2%) were women and 39 (16.8%) were men. Average age was 33.4 years (SD 12.4). Regarding marital status, 127 (54.7%) subjects were single, 91 (39.2%) were married, 8 subjects (3.4%) were separated, and 6 (2.6%) were living together with someone. Economic support was shared in 56.5% of the cases (131 subjects), it came exclusively from the subject of the study in 84 cases (36.2%) and mainly from the partner in 17 cases (7.3%).
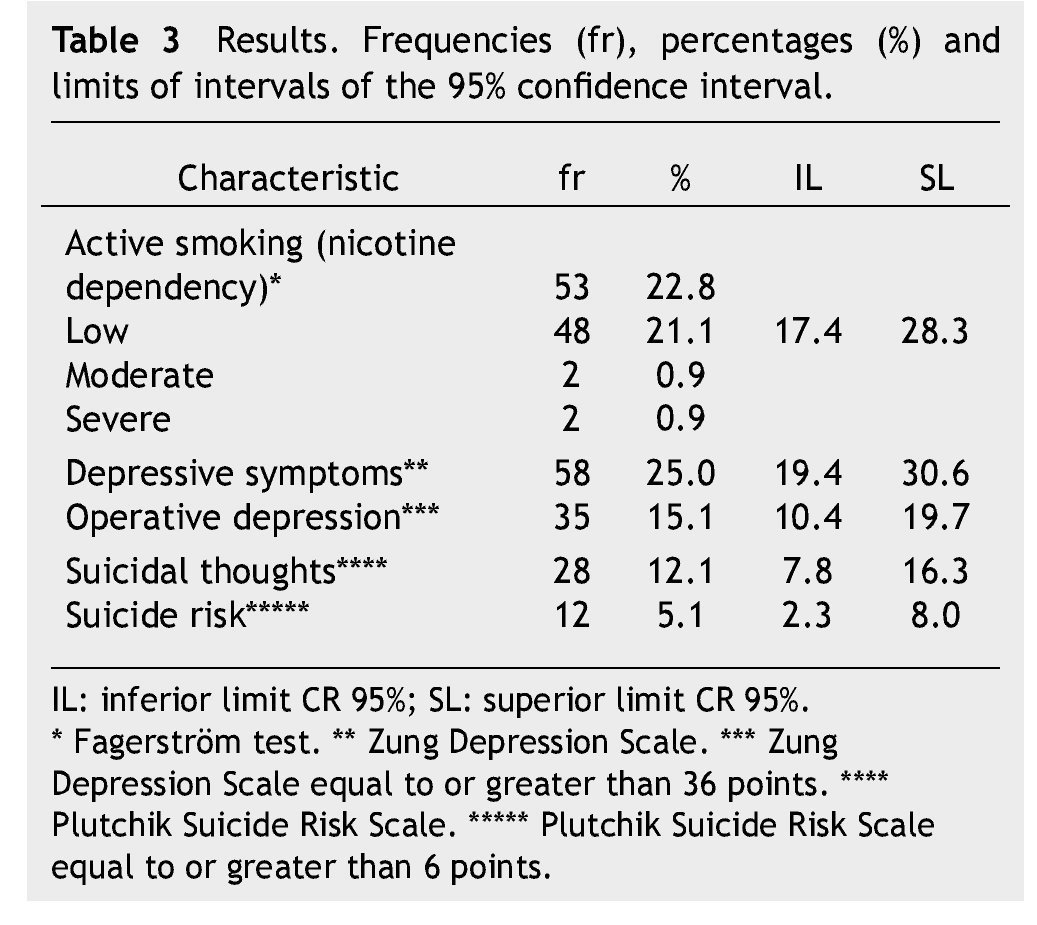
2. Prevalence
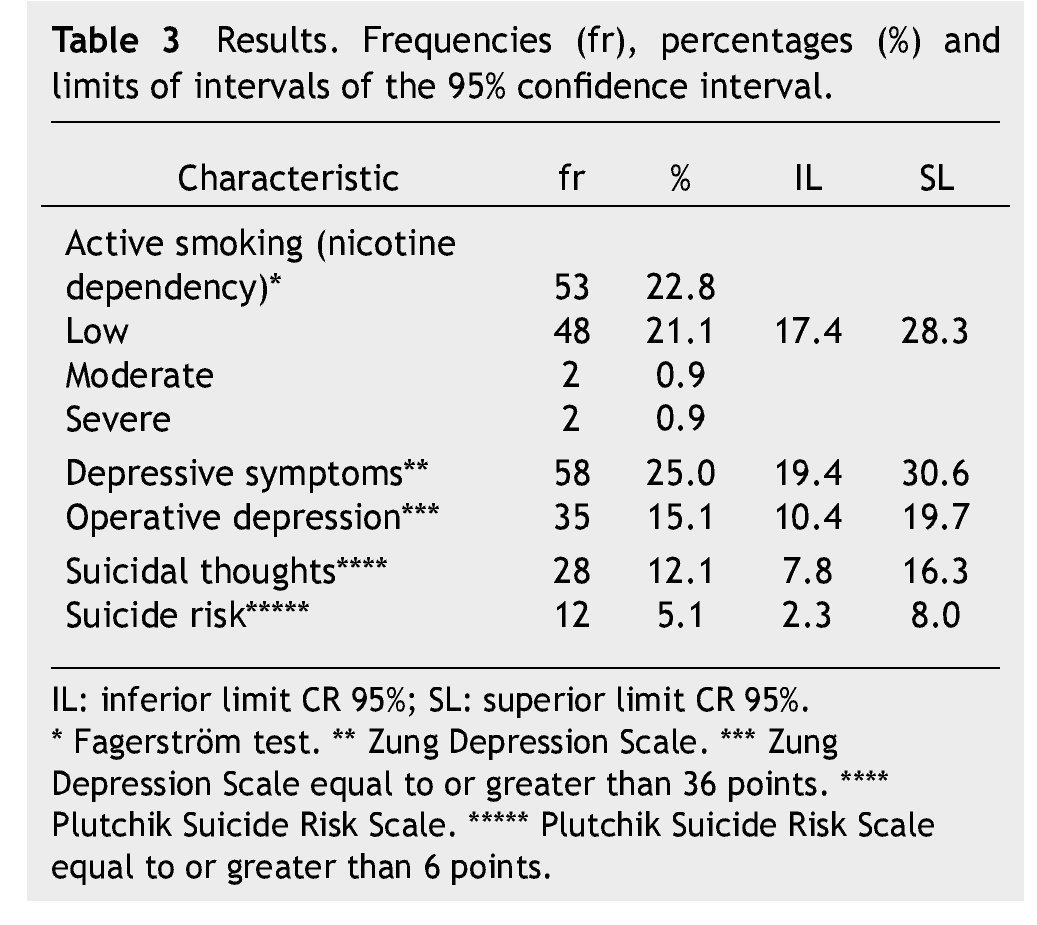
With a 95% confidence interval we found the following prevalences: for tobacco, 52 subjects (22.8%); operative depression, 35 subjects (15.1%), and under suicide watch, 12 subjects (5.1%) (table 3).
3. Characteristics of the group of nurses who smoke (53 in total)
There were 37 females and 16 males, with a statistically significant difference by gender. The males were more vulnerable to developing smoking habits (p=0.006). Average age of male nurses who smoke was 29.2 years. We also found that the younger the age the more likely they are to smoke (p=0.015).
Regarding marital status, 37 subjects (71%) did not have a partner and 16 (29%) did. About schooling, 27 had a technical degree (51.9%), 24 had a bachelor's degree (46.2) and 1 had a master's degree (1.9%). We found 2 protective factors against smoking: having a partner (p=0.038) and having a bachelor's degree (p=0.048).
The areas/departments where subjects smoked the most were Shock trauma (10 subjects) and Internal Medicine (10 subjects); the areas/departments where subjects smoked the least were Pediatrics (1 subject), Nursing Administration (1 subject), and External Consultation (1 subject); there were areas/departments where the subjects did not smoke (Oncology and Neurology). Of the 53 nurses, 10 subjects had suicidal thoughts and 6 subjects obtained a score of 6 or greater on the Plutchik Suicide Risk Scale, which places them as without risk of suicide.
4. Operative depression (36 to 80 points detected by Zung Self-Rating Scale)
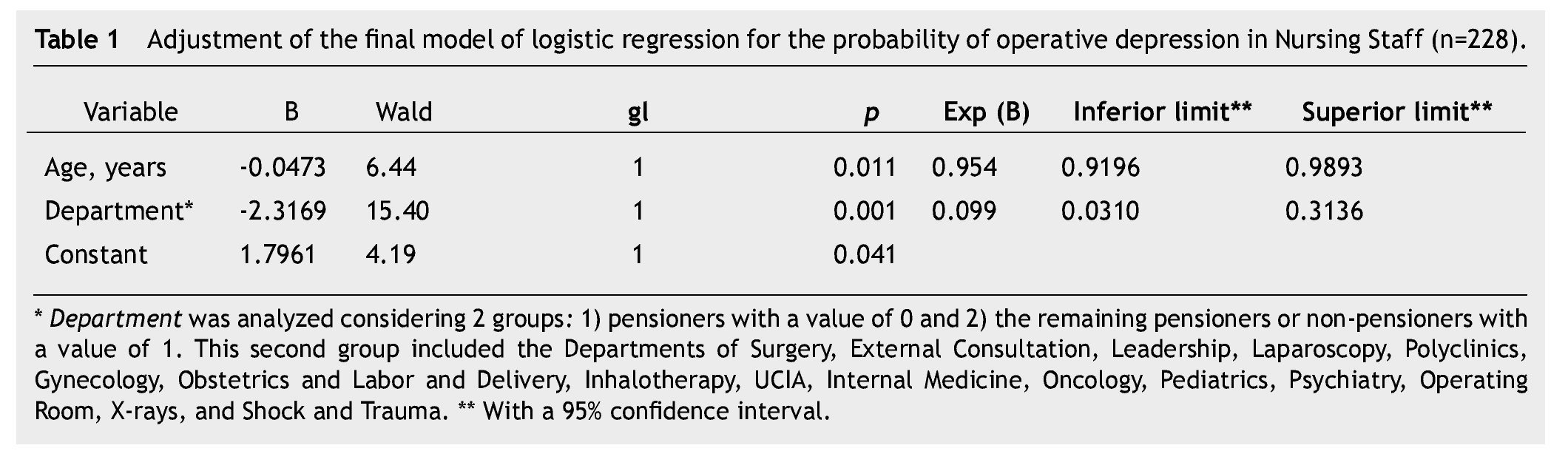
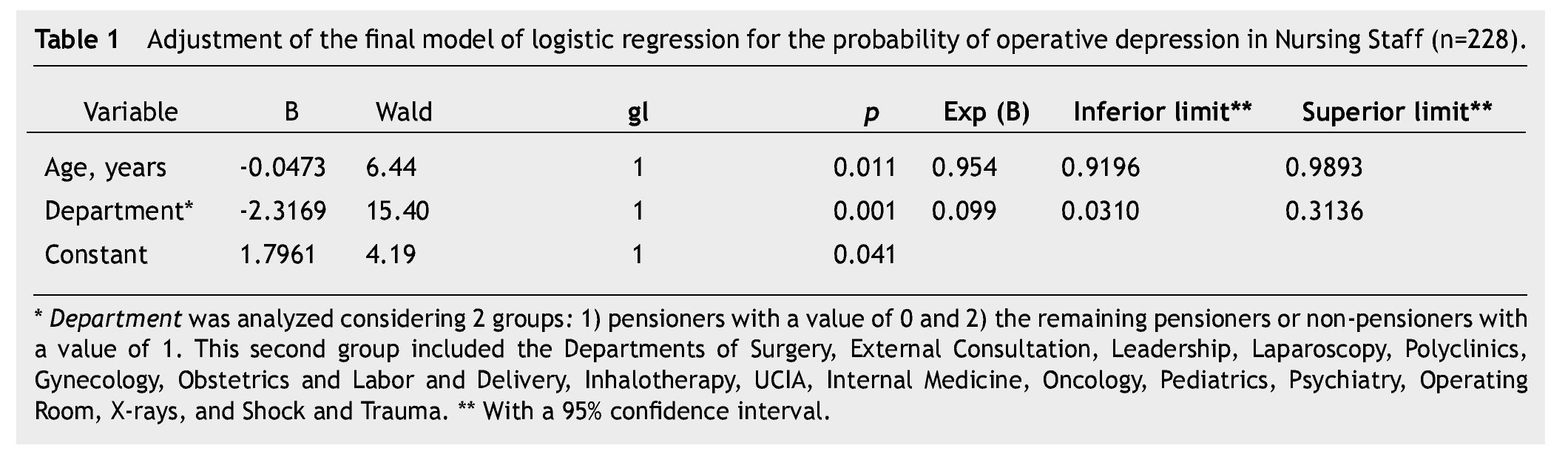
Of the 35 subjects with operative depression, 29 were females and 6 were males. Table 1 shows that the possibility of nurses developing operative depression is greater in the Department of Pensioners (Wald=15.40; p=0.001) compared to the rest of the departments at the hospital; this probability decreases with the increasing age of the nursing professional (Wald=6.44; p=0.011) (Fig. 1).
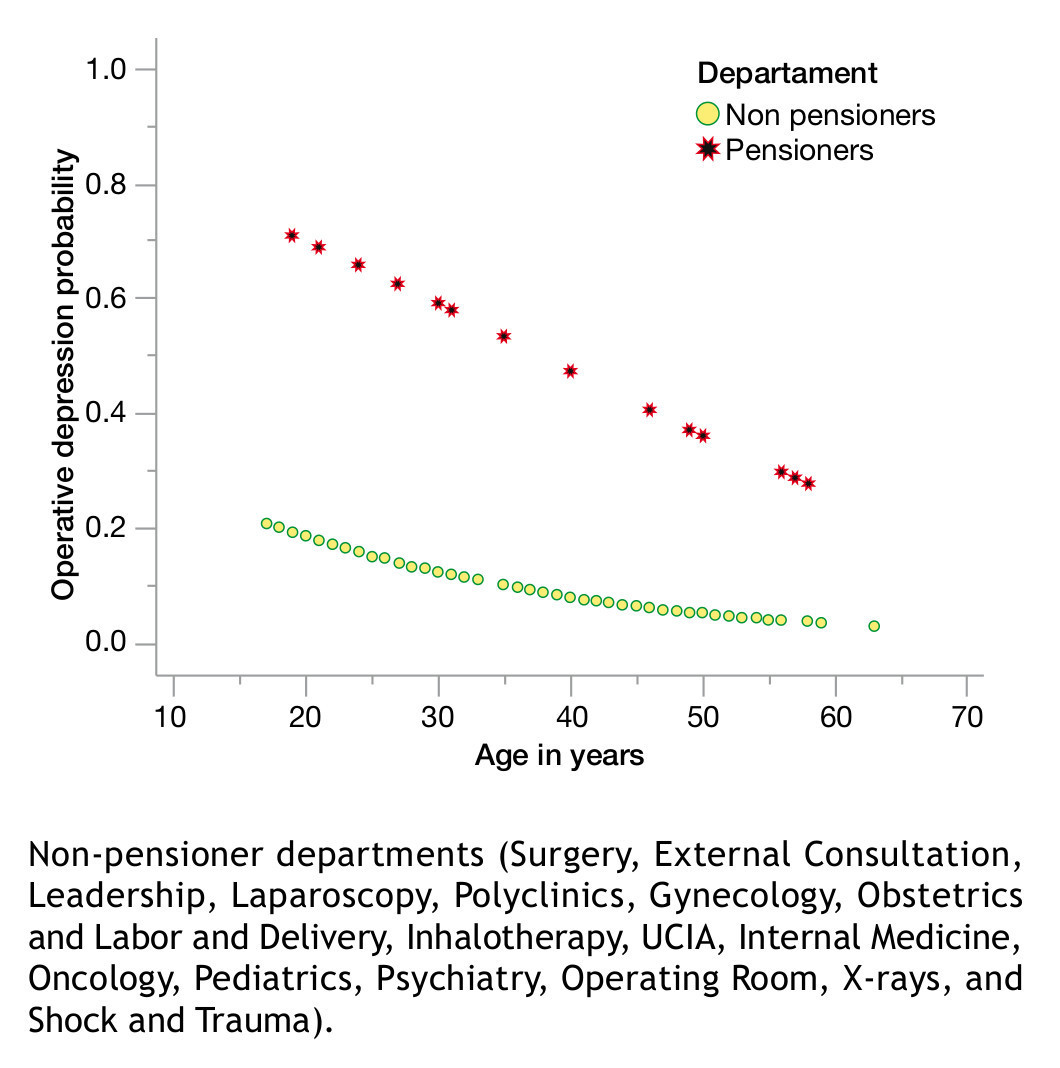
Figure 1 Probability of presenting operative depression according to the department of the University Hospital where the study was conducted.
Of the 35 subjects with operative depression, 8 smoked and 27 did not. We found no statistically significant connection between smoking and displaying depressive or operative depression symptoms.
5. Suicide risk (greater or equal to 6 points detected on the Plutchik Suicide Risk Scale, i.e., without risk of suicide)
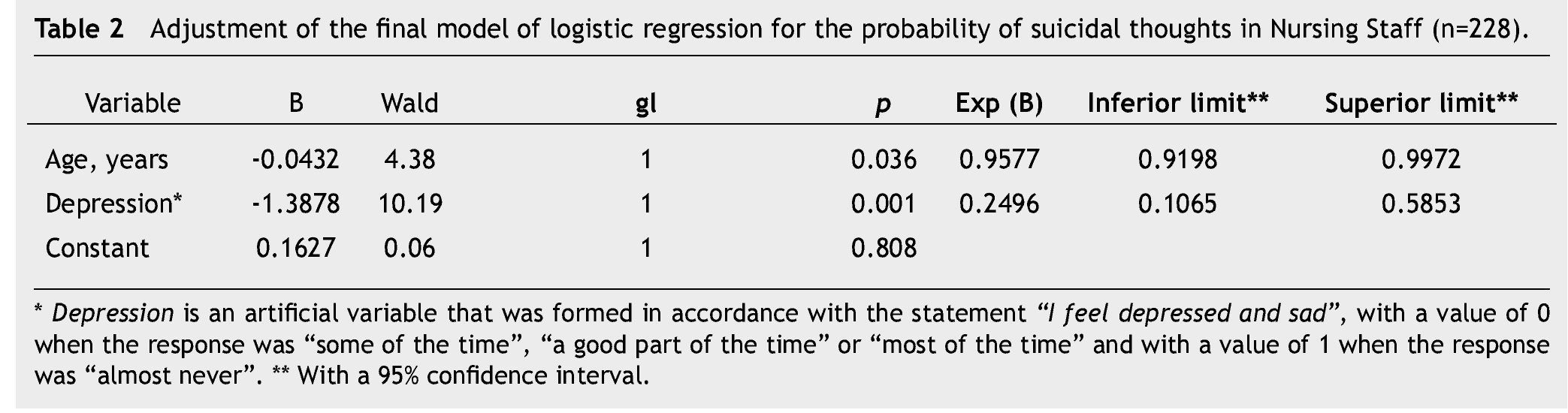
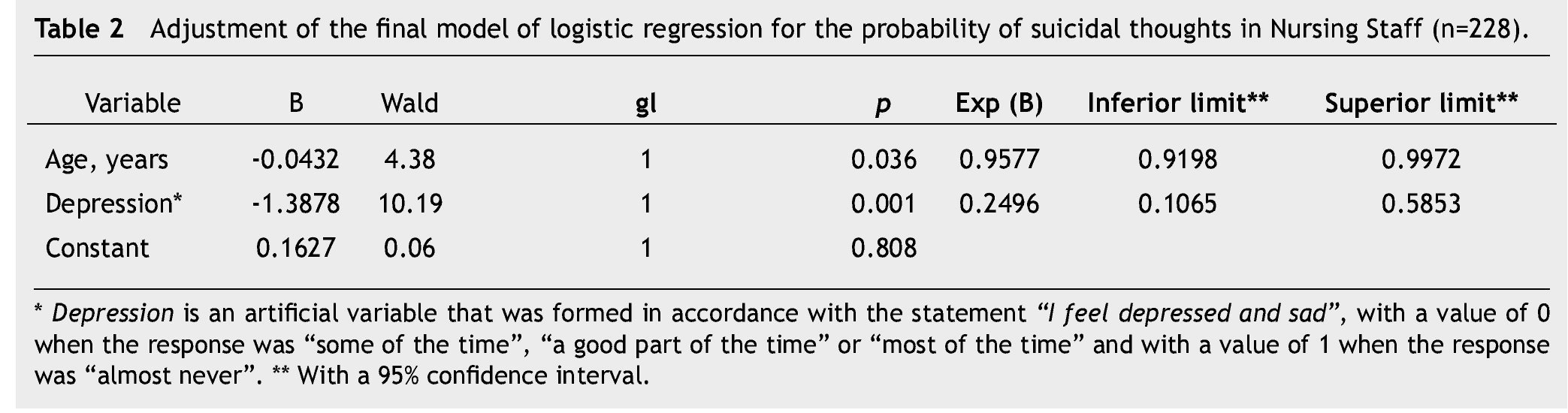
All of the 12 subjects found to have a suicide risk were females. Average age for suicide risk was 29.7 years. The variables which were significant to model the probability of suicidal thoughts were age and "feeling down and sad'. When the patient indicates he/she feels down and sad for a "short time," the probability of suicidal thoughts is lower than when said health professional expresses feeling down and sad "some of the time", "a good part of the time" or even "most of the time" (Wald=10.19; p=0.001). Additionally, table 2 shows the probability of having suicidal thoughts decreases when the nurse's age increases (Wald=4.38; p=0.036) (Fig. 2).
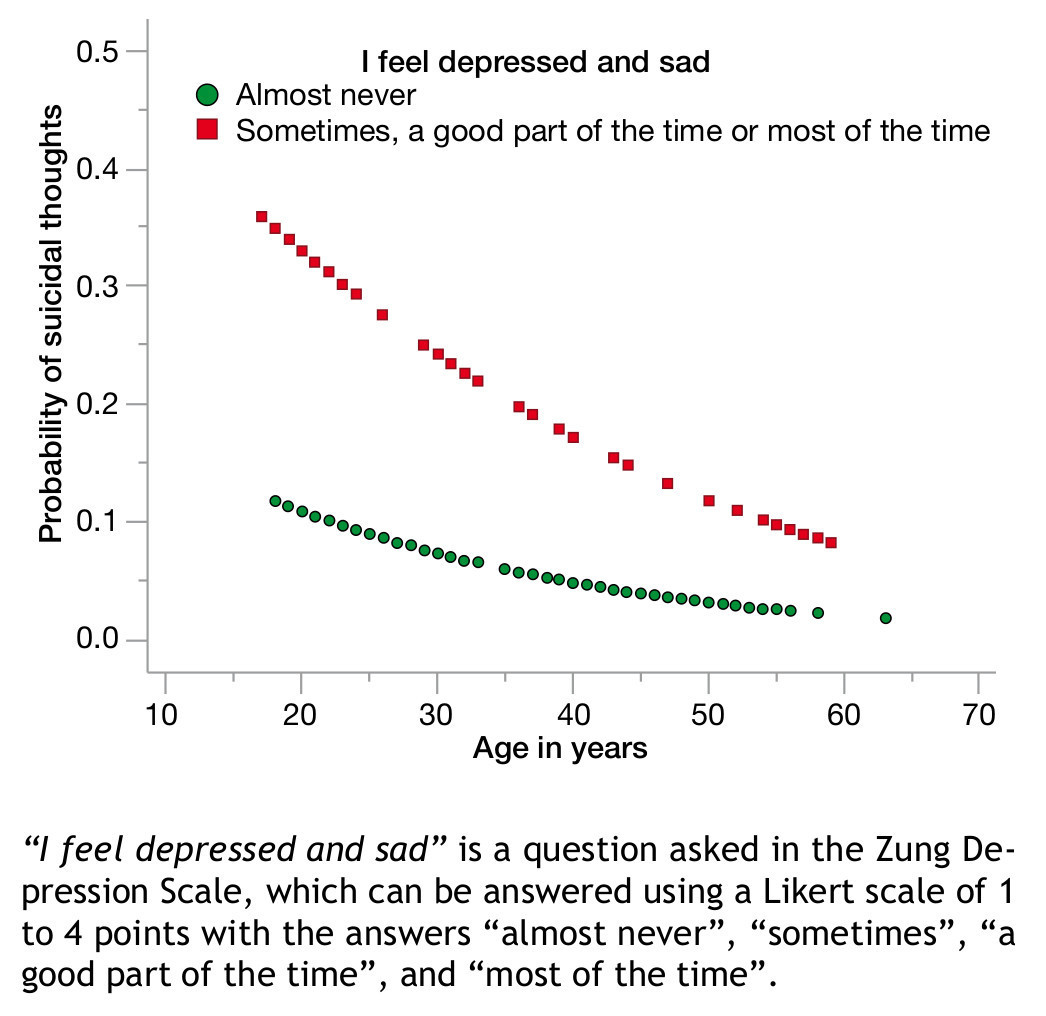
Figure 2 Probability of suicidal thoughts according to age.
The probability of displaying suicide risk depends mainly on 2 factors. One is having operative depression (p=0.001). Eight subjects out of the 12 with suicide risk, also displayed criteria for operative depression and active smoking (p=0.05). Of the 12 subjects with suicide risk, 6 smoke. The ones who do smoke have a probability of suicide risk of 0.113 and those who don't have a probability of 0.033. Therefore, there is a connection between smoking and suicide risk (p=0.05).
Discussion
When the causal factor has been studied, it has been demonstrated that depressive patients are more prone to smoke than the general population and show an important reduction in the severity of their symptoms with nicotine consumption.2,13 Moreover, tobacco abstinence may trigger depressive symptoms.12,13
Studies of patients undergoing anti-tobacco treatment have revealed that when depressive symptoms appear during the sixth week and sixth month of abstinence, there is a greater risk of relapsing. In the same way, it has been proposed that people with depression smoke as a way of self-medication against these depressive symptoms through negative reinforcement.14 these patients have greater odds of remaining in abstinence by receiving anti-depressive treatments like bupropion, fluoxetine, moclobemide or nortriptyline. It was recently reported that the depressive symptomatology level predicts the development of smoking in non-smokers.2,12,13
The connection can also be studied conversely, in other words, smoking as a cause of depression, since there is evidence that smokers and ex-smokers have an 80% higher probability of developing depression in comparison with those who have never smoked.2 Comorbidity studies show that depression is more frequently associated with intense smoking (more than 20 cigarettes a day) and nicotine dependence, more than with a "light" or "moderate" use of tobacco.12
When considering both possible comorbidity explanations (common risk factors or causal association), there is evidence of a shared etiology between dysthymia and intense smoking. One of the possible causes of this shared vulnerability is the fact that there is a genetic similitude shared amongt relatives that gives specific character traits such as neurotic traits and negative affectivity.12
Little is known about specific patient populations which register smoking and depression simultaneously, and there is a need for more information in order to implement integral treatments specific for this type of patient, taking into consideration gender, depression severity and level of nicotine dependence.13 this is the first assessment in Nuevo León applied to a specific population and describing the connection between depressive symptoms, socio-demographic characteristics and tobacco use. While some epidemiologic studies have demonstrated an independent association between smoking and major depression, other studies have shown that depression does not show a significant connection to smoking once comorbidity is adjusted.12
An indirect connection between smoking and depression has been suggested. Depression has been associated with tobacco consumption exclusively in the presence of comorbidity with behavioral problems. Other studies have found a connection between smoking and light depressive symptoms, rather than smoking and major depressive disorders.13
Compared to non-smokers, heavy smokers are at a higher risk of suicide. Suicide risk is related with the number of cigarettes smoked daily. Smokers of 15 or more cigarettes a day have a suicide risk 4 times higher than non-smokers.14
There are different characteristics among smokers and non-smokers: the presence of depression, schizophrenia, alcohol and drug abuse, ideation and intention of suicide, a greater risk of developing cancer, not being married and being socially isolated. All of these risk factors are more frequently displayed amongst smokers rather than non-smokers. In addition, smokers have a higher tendency of acting hostile and having more anxiety.14
There are 4 possible explanations for the relationship between tobacco consumption and suicide:14
1. Depression is a common background to suicide, and it is a condition that preconditions smoking as self-medication.
2. Smoking produces chemical changes in the brain which predispose to depression, which increases the risk of suicide.
3. Smoking increases the risk of chronic diseases like cancer, which predisposes to suicide.
4. Smoking is associated with other personal characteristics predisposing to suicide, such as low self-esteem, not because smoking lowers self-esteem, but because in our culture they tend to occur simultaneously.
This study does not pretend to define the causality between smoking and psychopathology, given the complexity of this matter and the multiple variables that should be studied; however, it does aspire to study some of the specific situations in the Nursing Staff and the connection between smoking and depression or suicide risk. We stress the need to continue investigating this subject, since contrary to what the literature shows, in this study we did not find a connection between smoking and the presence of depressive symptoms. We could presume that the population within the Nursing Staff is different from the rest of the population, and that as one of the hypotheses mentioned in the previous text, smoking may be used as a self-medication against depression, and that those nurses who smoke were not detected with depressive symptoms for this reason. There is evidence supporting that the Nursing Staff is under work stress and unfavorable working conditions, displaying psychopathology; this study detected the fact that there is at least one hospital area/department which must be studied more thoroughly in order to find specific stress factors, because of its connection with operative depression in its Nursing Staff. Just as reported in international literature, this study found an association between smoking and suicide risk. Some of the study's limitations are the fact that we only considered Zung's Self-Rating Scale to determine the presence or absence of depression (operative depression higher or equal to 36 points) and we did not perform a structured interview which could define it in terms reflected in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) as a persistent depressive disorder with mixed demonstrations. We did not consider work stress factors such as double shifts or working life in the study.
Conclusion
We recommend considering nicotine dependency a fundamental part in the evaluation of psychological aspects in nursing professionals, because its association with suicide risk was demonstrated. We highlight the importance of creating preventive measures for the Nursing Staff, like group therapy to provide psycho-occupational support against smoking, depression and suicide risk.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
No financial support was provided.
Received: November 2013;
Accepted: April 2014
* Corresponding author:
Francisco I. Madero and Dr. Eduardo Aguirre Pequeño, Mitras Centro, Z.P.
64460, Monterrey, N. L. Mexico.
Cell phone: 52 (81) 8287 5681.
E-mail address: raquelalejandra_kafka@hotmail.com (R. A. Sánchez-Núñez).