





To analyze the survival of patients hospitalized with COVID-19 and who presented some vascular thrombotic complication.
Material and MethodsAll consecutive patients with COVID-19 who were treated during the months of March and April 2020 at our institution were included. All patients were symptomatic and the thrombotic event objectively confirmed. Patients with deep vein thrombosis (DVT), pulmonary embolism (PE), ischemic stroke, and peripheral arterial thrombosis (PAT) were included. Survival curves for all groups were analyzed using Kaplan-Meier with Log Rank test, and Cox regression.
ResultsDuring the pandemic period from March-1 to April-30, 2943 patients were treated with confirmed COVID-19 in our center. 106 patients showed some symptomatic vascular thrombosis: 13 patients had PAT, 15 ischemic stroke, 20 DVT and 58 PE. 11 patients presented multiple vascular thrombosis. Although the mean age was 65 years, there were differences between groups being older those patients with arterial thrombosis. A 67.92% were men. In total, 25 patients died during their hospital admission (23.58%), with differences between groups, being more common in patients with PAT (9 patients out of 13) and ischemic stroke (8 patients out of 15), than in those with DVT (1 patient out of 20) or PE (7 patients out of 58).
ConclusionsThe venous thromboembolic risk in these patients is greater than the arterial, but arterial thrombosis when it occurs was associated with high mortality rates. Survival was better in patients with DVT and PE than in patients with ischemic stroke or PAT.
Presentar nuestra experiencia y analizar la supervivencia de los pacientes hospitalizados con COVID-19 y que presentaron algún proceso trombótico vascular.
Material y MétodosSe incluyeron todos los pacientes consecutivos COVID-19 que fueron atendidos durante los meses de marzo-abril 2020 en nuestra institución. Se incluyeron pacientes sintomáticos con trombosis venosa profunda (TVP), tromboembolia pulmonar (TEP), ictus isquémico y trombosis arterial periférica (TAP) confirmados objetivamente. Se analizaron las curvas de supervivencia de todos los grupos mediante Kaplan-Meier, test de Log Rank, y regresión de Cox.
ResultadosDurante el periodo pandémico del 1-marzo al 30-abril, se atendieron 2943 pacientes COVID-19 en nuestro centro. 106 pacientes presentaron algún proceso trombótico vascular sintomático: 13 pacientes tuvieron TAP, 15 ictus, 20 TVP y 58 TEP. 11 pacientes mostraron trombosis vasculares múltiples. Aunque la edad media fue de 65 años, fueron de edad más avanzada los que mostraron trombosis arteriales que procesos tromboembólicos venosos. El 67.92% fueron hombres. En total, 25 pacientes murieron durante su ingreso hospitalario (23.58%), existiendo diferencias entre grupos siendo más común en pacientes con TAP (9 pacientes de 13), e ictus isquémico (8 pacientes de 15), que en los de TVP (1 paciente de 20) o TEP (7 pacientes de 58).
ConclusionesEl riesgo tromboembólico venoso en estos pacientes es mayor que el arterial, pero la trombosis arterial cuando acontece estuvo asociada a altas tasas de mortalidad. La supervivencia fue mejor en los pacientes con TVP y TEP que en los pacientes con ictus isquémico o trombosis arterial periférica.
Patients with SARS-CoV-2 coronavirus infection (or COVID-19) are at increased risk of arterial or venous thromboembolic disease.1–5 However, the information regarding mortality associated with these conditions is poorly understood. In this article we report on our experience and analyse the survival of patients who were hospitalised with COVID-19 and who developed a vascular thrombotic event during the months of March and April 2020 in a large university hospital in Madrid.
Material and methodsStudy populationData from consecutive patients with a diagnosis of pneumonia and SARS-CoV-2 infection confirmed in all cases by a reverse transcriptase-polymerase chain reaction (RT-PCR) test were included in this cohort study. All the patients included with COVID-19 were treated during the months of March and April 2020 (the highest peak of infection in Madrid) in our department at the 12 de Octubre University Hospital. All patients were symptomatic, were hospitalized for their respiratory disease and required our assessment for some arterial or venous thrombotic event. All diagnoses were objectively confirmed with imaging scans. Doppler ultrasound was used in patients with suspected deep vein thrombosis (DVT) and CT angiography in cases of acute arterial ischemia, large vessel occlusion ischemic stroke or pulmonary embolism (PE). Young patients (<16 years) with unconfirmed clinical diagnosis were excluded from the analysis. The hemodynamic tests were cancelled due to the risk of infection and the limitations in the examination.
This study was approved by the clinical research ethics committee and the need for informed consent was waived due to the observational nature of the study.
Data collectionThe patients were identified from the registry data obtained from the computerized hospital management system and from the patient information system of our department (electronic medical record). Electronic medical records served as a data source for the collection of demographic and clinical characteristics, laboratory parameters, treatment, and results, which were recorded prospectively. The date of admission to the hospital and the date of the first thrombotic event were considered. We recorded patients rather than thrombotic disorders, as there were cases with multiple episodes. In this series, the main vascular event has always been considered the primary event that prompted their hospitalization or initiated their clinical symptoms.
DeterminationsThe mortality of patients with COVID-19 with peripheral arterial thrombosis, DVT, PE, and large vessel occlusion ischemic stroke was compared. All patients were symptomatic of their primary thrombotic event. The patient's demographic characteristics and laboratory parameters were analysed upon admission and on the date of the episode. All patients underwent follow-up until discharge from hospital or until death.
StatisticsContinuous variables were expressed as mean±standard deviation and were compared using the ANOVA test, with subsequent paired analysis. The mean hospital stay was expressed as median±interquartile range. The categorical variables were expressed as relative and absolute frequencies and were compared using the χ2 test. Survival was analysed using Kaplan-Meier curves and log rank test. In addition, Cox regression was used to study the association between thrombotic events and survival, taking as reference the variable of thrombotic episode with the largest size and performing a univariate and multivariate analysis adjusted for the different clinical covariates that could have a possible influence. All analyses were done with the SAS statistical software, version 9.4, of the SAS System for Windows (copyright © 2002–2012 SAS Institute Inc.).
ResultsDuring the pandemic period from 1st March to 30th April, 2,943 confirmed patients were treated at our center, with 261 admissions to the intensive care unit. Of these, 106 patients showed symptomatic vascular thrombosis (arterial or venous); 11 patients showed multiple vascular thrombosis in different sites and of a different nature.
7 patients showed DVT, with an incidental finding of asymptomatic PE. During the stroke study, there were several incidental findings in different patients: in one patient an asymptomatic aortic thrombus was detected, a PE in another patient and both PE and DVT in another. Finally, PE was also detected in a patient who showed acute arterial ischemia. Therefore, PE was the most common thrombotic finding in all patients with associated thrombosis.
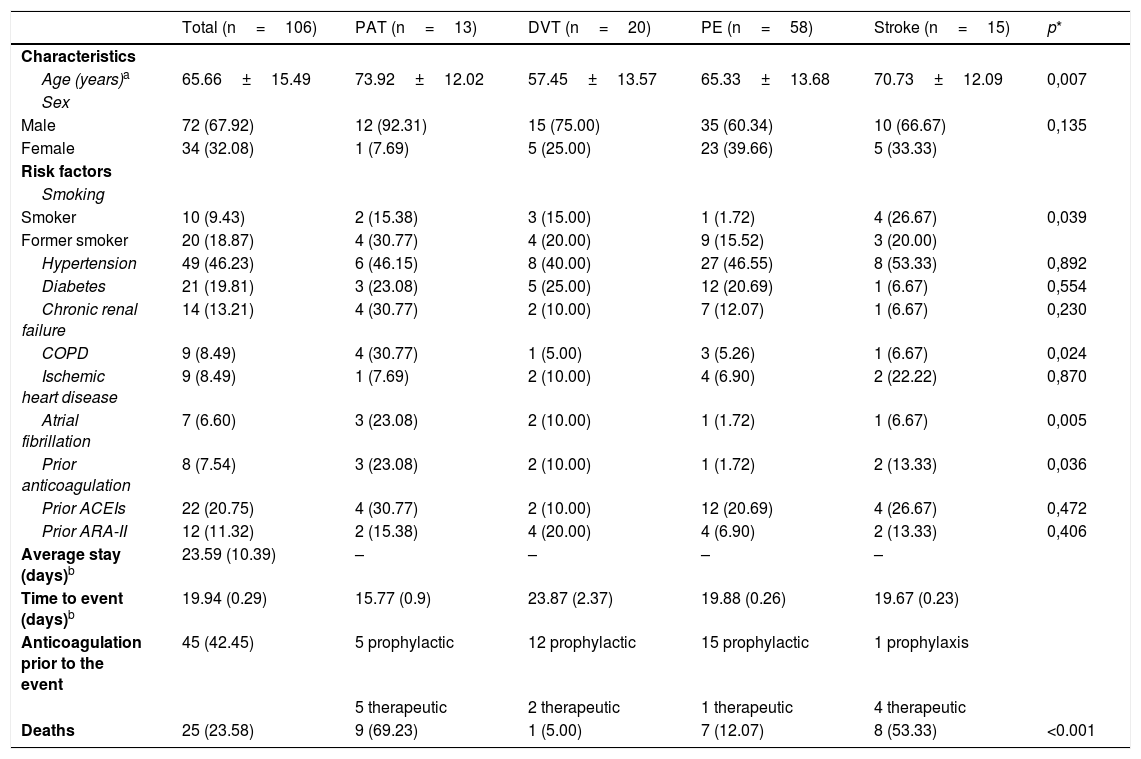
All the data on the clinical characteristics, risk factors and medical history are collected in Table 1. Of the total, 13 patients (12.26%; 95% CI: 6.69–20.05) had peripheral arterial thrombosis, 15 patients (14.15%; 95% CI: 8.14–22.26) had an ischemic stroke, 20 patients (18.86%; 95% CI: 11.92–27.62) had DVT and 58 patients (54.71%; 95% CI: 44.75–64.40) had PE. The most common vascular event among COVID-19 patients was symptomatic PE.
Patient characteristics.
| Total (n=106) | PAT (n=13) | DVT (n=20) | PE (n=58) | Stroke (n=15) | p* | |
|---|---|---|---|---|---|---|
| Characteristics | ||||||
| Age (years)a | 65.66±15.49 | 73.92±12.02 | 57.45±13.57 | 65.33±13.68 | 70.73±12.09 | 0,007 |
| Sex | ||||||
| Male | 72 (67.92) | 12 (92.31) | 15 (75.00) | 35 (60.34) | 10 (66.67) | 0,135 |
| Female | 34 (32.08) | 1 (7.69) | 5 (25.00) | 23 (39.66) | 5 (33.33) | |
| Risk factors | ||||||
| Smoking | ||||||
| Smoker | 10 (9.43) | 2 (15.38) | 3 (15.00) | 1 (1.72) | 4 (26.67) | 0,039 |
| Former smoker | 20 (18.87) | 4 (30.77) | 4 (20.00) | 9 (15.52) | 3 (20.00) | |
| Hypertension | 49 (46.23) | 6 (46.15) | 8 (40.00) | 27 (46.55) | 8 (53.33) | 0,892 |
| Diabetes | 21 (19.81) | 3 (23.08) | 5 (25.00) | 12 (20.69) | 1 (6.67) | 0,554 |
| Chronic renal failure | 14 (13.21) | 4 (30.77) | 2 (10.00) | 7 (12.07) | 1 (6.67) | 0,230 |
| COPD | 9 (8.49) | 4 (30.77) | 1 (5.00) | 3 (5.26) | 1 (6.67) | 0,024 |
| Ischemic heart disease | 9 (8.49) | 1 (7.69) | 2 (10.00) | 4 (6.90) | 2 (22.22) | 0,870 |
| Atrial fibrillation | 7 (6.60) | 3 (23.08) | 2 (10.00) | 1 (1.72) | 1 (6.67) | 0,005 |
| Prior anticoagulation | 8 (7.54) | 3 (23.08) | 2 (10.00) | 1 (1.72) | 2 (13.33) | 0,036 |
| Prior ACEIs | 22 (20.75) | 4 (30.77) | 2 (10.00) | 12 (20.69) | 4 (26.67) | 0,472 |
| Prior ARA-II | 12 (11.32) | 2 (15.38) | 4 (20.00) | 4 (6.90) | 2 (13.33) | 0,406 |
| Average stay (days)b | 23.59 (10.39) | – | – | – | – | |
| Time to event (days)b | 19.94 (0.29) | 15.77 (0.9) | 23.87 (2.37) | 19.88 (0.26) | 19.67 (0.23) | |
| Anticoagulation prior to the event | 45 (42.45) | 5 prophylactic | 12 prophylactic | 15 prophylactic | 1 prophylaxis | |
| 5 therapeutic | 2 therapeutic | 1 therapeutic | 4 therapeutic | |||
| Deaths | 25 (23.58) | 9 (69.23) | 1 (5.00) | 7 (12.07) | 8 (53.33) | <0.001 |
ARA-II: angiotensin II receptor antagonists; COPD: chronic obstructive pulmonary disease; ACEI: angiotensin converting enzyme inhibitors.
The mean age of the patients with COVID-19 was 65±15.49 years. Those who showed arterial thrombosis were older (73,92±12.02) than those who showed DVT (57.45±13.57). Seventy-two patients (67.92%) were men. Eight patients with ischemic stroke were admitted from the emergency department, who were treated with neurointerventional procedures in the stroke unit. The other patients were identified during hospital admission.
The median overall hospitalization time was 23.59 days. The median time to the episode was 15.77 days in patients with arterial thrombosis, 23.87 days in patients with DVT, 19.88 days in patients with PE, and 19.67 days in patients with stroke.
No differences were observed regarding risk factors, with the exception of smoking and atrial fibrillation. 28.30% had a history of smoking, which was more common among those who had arterial ischemic episodes (6 patients out of 13) or stroke (7 patients out of 15). Likewise, atrial fibrillation was more common in patients with arterial thrombotic events (3 patients with peripheral ischemia and 2 patients with stroke).
In our series, 8 patients received anticoagulation before admission but, despite this, they developed arterial or venous thrombosis. During hospitalization, most patients (61 patients out of 106; 57.55%) did not receive any type of anticoagulation, 33 patients (31.13%) were treated with prophylactic doses of low molecular weight heparin (LMWH) and only 12 patients (11.32%) were anticoagulated before the thrombotic event. Despite prophylactic or therapeutic anticoagulation, 20 patients had rethrombosis (8 patients with arterial ischemia, 5 with stroke, one with various thrombotic events, and 6 with PE). This rethrombosis event (arterial or venous) was always associated with the death of the patient.
Of the 13 patients with arterial thrombosis, only 7 were operated on for acute arterial ischemia. All patients were previously healthy and only one patient had previous vascular disease (a popliteal aneurysm that was thrombosed). Of these, only 3 survived after surgery: Two patients with thrombectomy and 1 woman with direct amputation. The rest of the patients who underwent surgery experienced rethrombosis despite anticoagulation and died. Two patients with free-floating aortic thrombi resolved satisfactorily with LMWH. The other patients with peripheral arterial thrombosis who were not operated on were older (> 80 years), with severe respiratory distress and a poor clinical condition that limited mobilization and surgery. These patients received palliative measures until they died.
Eight patients with large vessel occlusion ischemic stroke were treated using neurointerventional techniques; 3 patients rethrombosed and in one patient the procedure was unsuccessful due to immediate re-occlusion.
The laboratory parameters in patients with COVID-19 showed lymphopenia, thrombocytosis, increased LDH, D-dimer and elevated CRP, as has already been reported in the literature, with no differences between groups. No variable was predictive of the thrombotic event.
In total, 25 patients died during their hospitalization (23.58%), with differences between groups: death was more common in patients with peripheral arterial ischemia (9 patients out of 13) and ischemic stroke (8 patients out of 15) compared to those who showed DVT (1 patient out of 20) or PE (7 patients out of 58) (Fig. 1).
, with log rank analysis, which graphically show the difference in favour of venous thromboembolic events (DVT, PE) versus arterial thrombotic events (stroke, peripheral arterial thrombosis) (p<0.0001).")
Kaplan-Meier survival curves for DVT, PE, stroke, and peripheral arterial thrombosis (PAT), with log rank analysis, which graphically show the difference in favour of venous thromboembolic events (DVT, PE) versus arterial thrombotic events (stroke, peripheral arterial thrombosis) (p<0.0001).
No haemorrhages were recorded in this series, or readmissions of patients with recurrent thrombosis.
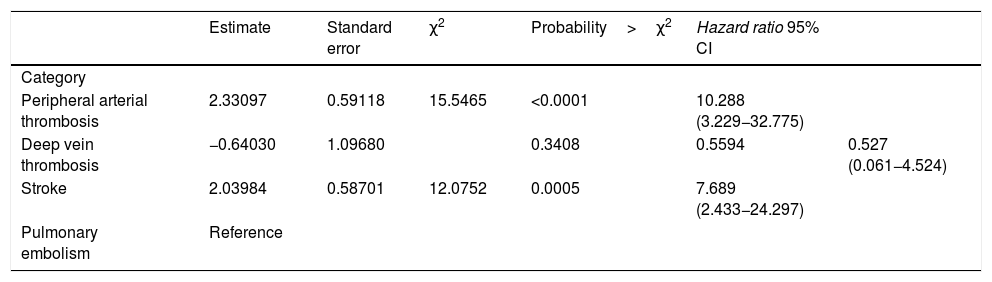
An effect of thrombotic events on mortality was observed in the univariate analysis, which was for peripheral arterial thrombosis (HR 10.288; 95% CI: 3.229–32.77); for DVT (HR 0.527; 95% CI: 0.061−4.524) and for stroke (HR 7.689; 95% CI: 2.433 24.297) versus PE, as this was the reference variable (Table 2).
Univariate analysis.
| Estimate | Standard error | χ2 | Probability>χ2 | Hazard ratio 95% CI | ||
|---|---|---|---|---|---|---|
| Category | ||||||
| Peripheral arterial thrombosis | 2.33097 | 0.59118 | 15.5465 | <0.0001 | 10.288 (3.229−32.775) | |
| Deep vein thrombosis | −0.64030 | 1.09680 | 0.3408 | 0.5594 | 0.527 (0.061−4.524) | |
| Stroke | 2.03984 | 0.58701 | 12.0752 | 0.0005 | 7.689 (2.433−24.297) | |
| Pulmonary embolism | Reference |
Univariate analysis calculated using Cox regression, taking the variable pulmonary embolism as a reference, as it was the variable with the largest number of patients.
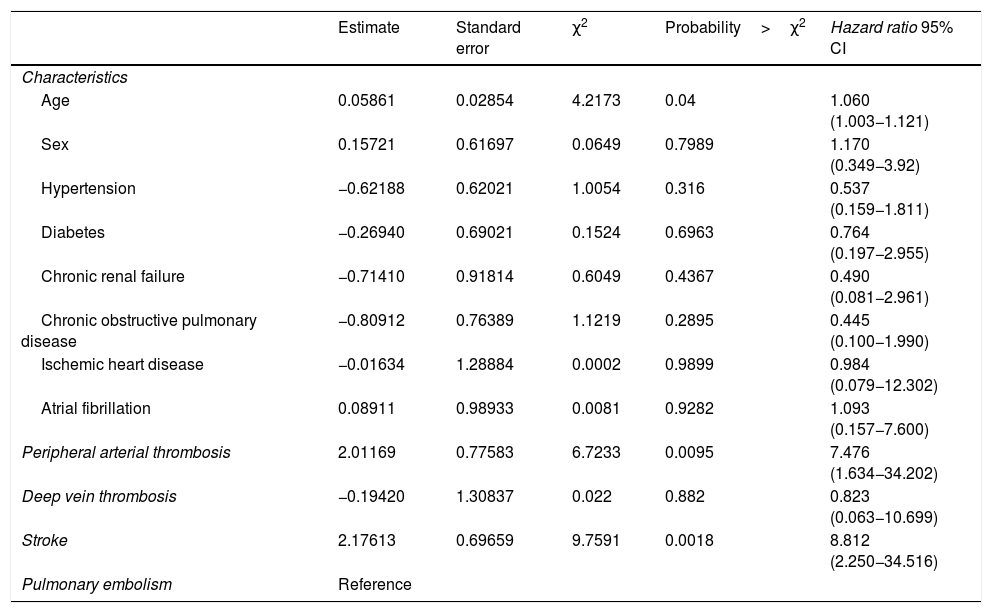
After a multivariate adjustment for the clinical variables that could have an influence (age, sex, hypertension, diabetes, renal failure, chronic obstructive pulmonary disease, ischemic heart disease and atrial fibrillation) this effect was maintained for arterial thrombotic events and stroke on mortality when compared with PE (Table 3).
Multivariate analysis.
| Estimate | Standard error | χ2 | Probability>χ2 | Hazard ratio 95% CI | |
|---|---|---|---|---|---|
| Characteristics | |||||
| Age | 0.05861 | 0.02854 | 4.2173 | 0.04 | 1.060 (1.003−1.121) |
| Sex | 0.15721 | 0.61697 | 0.0649 | 0.7989 | 1.170 (0.349−3.92) |
| Hypertension | −0.62188 | 0.62021 | 1.0054 | 0.316 | 0.537 (0.159−1.811) |
| Diabetes | −0.26940 | 0.69021 | 0.1524 | 0.6963 | 0.764 (0.197−2.955) |
| Chronic renal failure | −0.71410 | 0.91814 | 0.6049 | 0.4367 | 0.490 (0.081−2.961) |
| Chronic obstructive pulmonary disease | −0.80912 | 0.76389 | 1.1219 | 0.2895 | 0.445 (0.100−1.990) |
| Ischemic heart disease | −0.01634 | 1.28884 | 0.0002 | 0.9899 | 0.984 (0.079−12.302) |
| Atrial fibrillation | 0.08911 | 0.98933 | 0.0081 | 0.9282 | 1.093 (0.157−7.600) |
| Peripheral arterial thrombosis | 2.01169 | 0.77583 | 6.7233 | 0.0095 | 7.476 (1.634−34.202) |
| Deep vein thrombosis | −0.19420 | 1.30837 | 0.022 | 0.882 | 0.823 (0.063−10.699) |
| Stroke | 2.17613 | 0.69659 | 9.7591 | 0.0018 | 8.812 (2.250−34.516) |
| Pulmonary embolism | Reference |
Multivariate analysis calculated using Cox regression, adjusted for variables of clinical interest, taking as reference the variable PE because it is the one with the largest number of patients.
Patients with COVID-19 have a high thrombotic risk (arterial or venous), due to the large inflammatory component associated with SARS-CoV-2 infection, platelet activation, circulatory stasis due to their immobility and the possible endothelial dysfunction caused by the coronavirus.6–11 Our experience corroborates that the venous thromboembolic risk in these patients is higher than the arterial risk,12–14 but arterial thrombosis, when it occurs, further complicates the prognosis of these patients.
Thrombotic events were more common in men while arterial thrombosis (peripheral or stroke) was more common in smokers and elderly patients compared with those with DVT or PE. PE was the most common vascular event and the one most associated with other thrombotic events. Venous thromboembolic disease accounted for 73.6% of cases, while arterial thrombosis (peripheral and stroke) accounted for 26.4%. However, survival was significantly better in patients with DVT and PE than in patients with ischemic stroke or peripheral arterial thrombosis (Fig. 1). An arterial thrombotic episode during COVID-19 was associated with high mortality rates, which were catastrophic if they recurred.
In addition to the infection and high thrombogenicity of these patients, the high incidence of venous thromboembolic events in this population may be partly justified by the long mean stay and immobilization. In fact, many of these episodes occurred in patients who did not even receive prophylactic doses of LMWH, as was the case for most patients hospitalized in the first weeks of the pandemic. These observations justify the recommendations of scientific societies15,16 that all patients with COVID-19 should receive at least one prophylactic dose of LMWH because they are at high risk of thrombosis.
The high hypercoagulability of these patients may also explain why thrombotic events, especially arterial ones and stroke, occur not only in patients with cardiovascular risk factors or elderly people, but also in healthy or anticoagulated patients. These findings appear to support the hypothesis that SARS-CoV-2 induces endothelial dysfunction and diffuse inflammation that could explain the circulatory impairment and the high risk of rethrombosis despite anticoagulation.17,18 In fact, except in one case, arterial occlusions occurred in previously healthy arteries.
Furthermore, we observe that if these patients are operated on, mortality is even higher. Surgical trauma increases the vulnerability of these COVID-19 patients. In fact, it is important to emphasize that, despite anticoagulation, many of these patients had thrombosis recurrence and died. The high thrombogenicity of these patients discourages any complex procedure. The surgical technique, if necessary, should therefore be straightforward and simple with the goal of solving the problem and saving life.
Based on our clinical experience, we recommend that all patients with a thrombotic event maintain LMWH anticoagulation for at least one month after discharge due to its anti-inflammatory effect. They should then continue with the new oral anticoagulants to avoid monitoring and outpatient visits. Long-term treatment should be individualized and should consider the use of antiplatelet therapy only in patients with arterial thrombosis or stroke.
Laboratory parameters were comparable between all groups and consistent with what has been described in patients with coronavirus.1–7 Biomarkers are elevated in these COVID-19 patients, reflecting an inflammatory state and coagulation activation with a high level of D-dimer.
Our study has limitations. The patients included in this analysis were objectively diagnosed in one of the most affected areas of the European COVID-19 outbreak. The situation collapsed the health system and prompted the use of treatments that were extremely heterogeneous at the time. It is likely that it does not reflect the total incidence of venous thrombotic events, given the numerous hospitalized patients, the extreme severity of many of them and the limitation to perform complementary examinations, but it does include all patients known to have had arterial thrombotic events, regardless of the department to which they were assigned. Hospital circuits were not well established at that time, which made it difficult to manage many of them optimally. No global experience with the disease was available at the time, which may have influenced mortality rates. Furthermore, a comparative analysis of survival between historical hospital records or the critical population versus this cohort of patients with COVID-19 was not intended in this study. This article is only descriptive of the observed clinical situation and shows the real experience in a tertiary hospital in Madrid. Further research is needed to support these data and help identify future improvements in the management of these patients with vascular thrombotic complications and COVID-19.
FundingNone.
Conflict of interestsNone.
Please cite the article as: Comanges A, Gómez-Arbeláez D, Ibarra G, et al. Mortalidad de los pacientes COVID-19 con complicaciones trombóticas. Med Clin (Barc). 2021;156:112–117.
