








Physicians find it difficult to take on the role of the patient and they show unusual behaviors when ill. One of these behaviors is presenteeism, which is working while sick. The objective of this research is to analyze the factors that contribute to the phenomenon of presenteeism in Spanish physicians.
Material and methodsMixed methodology study: one national survey through the General Council of Medical Associations website (quantitative part), 22 semistructured interviews with sick residents and practicing physicians, and three focus groups involving professionals from the occupational health services (qualitative). A bivariate analysis using parametric and non-parametric tests. The significance level was p<0.05 (95% confidence interval). Qualitative analysis using the comparative-constant method until saturation of information.
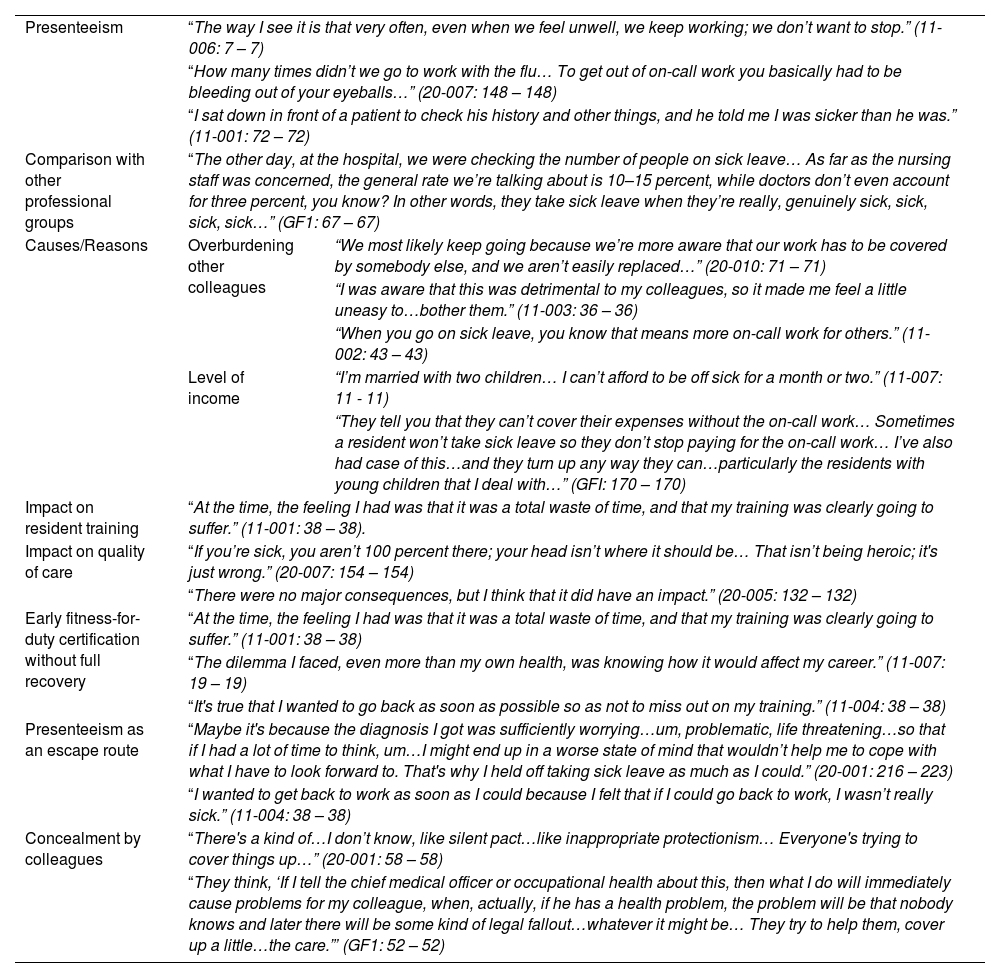
ResultsPresenteeism is reported by 89.4% of doctors who responded to the survey, and it is more common among women. Contributing factors include fear of overburdening colleagues (the main reason and more common among women 58.14% vs 48.35%), self-perception of doing one's duty (the second reason and more common among men, 44.63% vs 33.14%) and economic impact and difficulty in accepting the role of a sick person. This behavior has an impact on patient safety, and is part of the hidden curriculum that also affects the training of medical professionals.
ConclusionsPresenteeism is a widespread and accepted practice among medical professionals. Although normalized, and even appreciated as a way to avoid overburdening colleagues, presenteeism has important implications for clinical ethics and patient safety.
A los médicos les cuesta asumir el papel de pacientes y muestran comportamientos anómalos cuando están enfermos. Uno de estos comportamientos es el presentismo, que consiste en trabajar mientras estás enfermo. El objetivo de esta investigación es analizar los factores que contribuyen al fenómeno del presentismo en los médicos españoles.
Material y métodosEstudio de metodología mixta: una encuesta nacional a través de la página web del Consejo General de Colegios de Médicos (parte cuantitativa), 22 entrevistas semiestructuradas a residentes enfermos y médicos en ejercicio, y tres grupos focales en los que participaron profesionales de los servicios de salud laboral (cualitativa). Se realizó un análisis bivariante mediante pruebas paramétricas y no paramétricas. El nivel de significación fue p<0,05 (intervalo de confianza del 95%). Análisis cualitativo mediante el método comparativo/constante hasta la saturación de la información.
ResultadosEl presentismo es referido por el 89,4% de los médicos que respondieron a la encuesta. Y es más frecuente en las mujeres. Entre los factores que contribuyen a ello se encuentran el miedo a sobrecargar a los colegas (principal motivo y más frecuente en las mujeres, el 58,1 frente al 48,4%), la autopercepción de cumplir con el deber (segundo motivo y más frecuente en los varones, el 44,6 frente al 33,1%), el impacto económico y la dificultad para aceptar el papel de enfermo. Este comportamiento repercute en la seguridad del paciente, y forma parte del currículo oculto que también afecta a la formación de los profesionales médicos.
ConclusionesEl presentismo es una práctica extendida y aceptada entre los profesionales de la medicina. Aunque normalizado, e incluso apreciado como una forma de evitar sobrecargar a los colegas, el presentismo tiene importantes implicaciones para la ética clínica y la seguridad del paciente.

