









Today, primary care professionals’ (PCPs) perspectives on hospital quality are unknown when evaluating hospital quality priorities. The aims of the present study were to identify key healthcare quality attributes from PCPs’ perspective, to validate an instrument that measures PCPs’ experiences of healthcare quality multidimensionally and to define hospital quality priorities based on PCPs’ experiences.
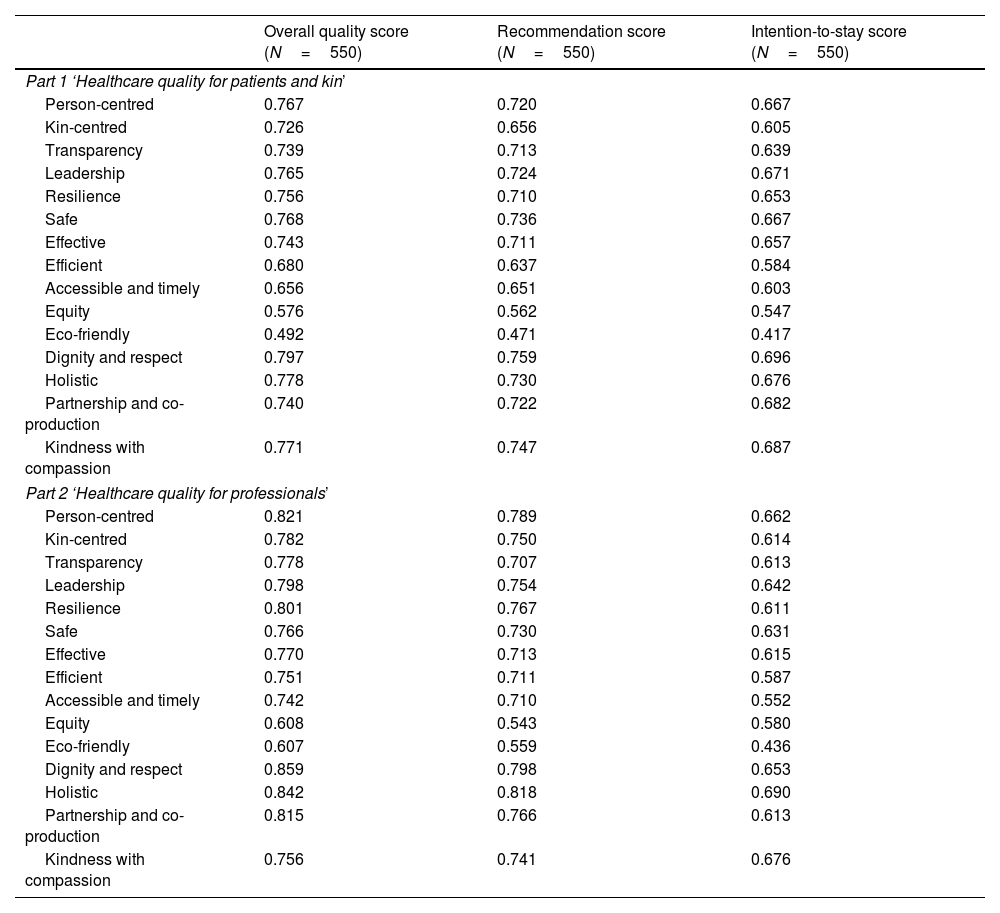
Material and methodsFocus groups with PCPs were conducted to identify quality attributes through a qualitative in-depth analysis. A multicentre study of 18 hospitals was used to quantitatively assess construct, discriminant and criterion validity of the FlaQuM-Quickscan, an instrument that measures ‘Healthcare quality for patients and kin’ (part 1) and ‘Healthcare quality for professionals’ (part 2). To set quality priorities, scores on quality domains were analyzed descriptively and between-hospital variation was examined by evaluating differences in hospitals’ mean scores on the quality domains using one-way Analysis of Variance (ANOVA).
ResultsIdentified key attributes largely corresponded with Lachman's multidimensional quality model. Including ‘Communication’ as a new quality domain was recommended. The FlaQuM-Quickscan was completed by 550 PCPs. Confirmatory factor analyses showed reasonable to good fit, except for the Root Mean Square Error of Approximation (RMSEA) in part 2. The ‘Equity’ domain scored the highest in parts 1 and 2. Domains ‘Kin-centred care’ and ‘Accessibility and timeliness’ scored the lowest in part 1 and ‘Resilience’ and ‘Partnership and co-production’ in part 2. Significant variation in hospitals’ mean scores was observed for eleven domains in part 1 and sixteen domains in part 2.
ConclusionsThe results gained a better understanding of PCPs’ perspective on quality. The FlaQuM-Quickscan is a valid instrument to measure PCPs’ experiences of hospital quality. Identified priorities indicate that hospital management should focus on multifaceted quality strategies, including technical domains, person-and kin-centredness, core values and catalysts.
En la actualidad, se desconocen las perspectivas de los profesionales de atención primaria (APP) sobre la calidad hospitalaria a la hora de evaluar las prioridades de la calidad hospitalaria. El objetivo del estudio fue identificar los atributos de calidad de la atención sanitaria desde la perspectiva de los médicos de atención primaria, validar un instrumento que mide las experiencias multidimensionales de los APP sobre la calidad de la atención sanitaria y definir las prioridades de calidad hospitalaria basándonos en las experiencias de los APP.
Material y métodosSe llevaron a cabo grupos focales con APP para identificar atributos de calidad mediante un análisis cualitativo en profundidad. Se utilizó un estudio multicéntrico de 18 hospitales para evaluar cuantitativamente la validez de construcción, discriminante y de criterio del FlaQuM-Quickscan, un instrumento que mide «Calidad de atención médica para pacientes y familiares» (parte 1) y «Calidad de atención médica para profesionales» (parte 2). Para establecer las prioridades de calidad, se analizaron descriptivamente las puntuaciones en los dominios de calidad, y se examinó la variación entre hospitales evaluando las diferencias en las puntuaciones medias de los hospitales en los dominios de calidad mediante Analysis of Variance (ANOVA) unidireccional.
ResultadosLos atributos clave identificados coincidieron en gran medida con el modelo de calidad multidimensional de Lachman. Se recomendó incluir «Comunicación» como un nuevo dominio de calidad. El FlaQuM-Quickscan fue completado por 550 APP. Los análisis factoriales confirmatorios mostraron un ajuste razonable a bueno, excepto para el Root Mean Square Error of Approximation (RMSEA) en parte 2. El dominio «Equidad» obtuvo la puntuación más alta en parte 1 y 2. Los dominios «Atención centrada en la familia» y «Accesibilidad y oportunidad» obtuvieron las puntuaciones más bajas en la parte 1 y «Resiliencia» y «Colaboración y coproducción» en la parte 2. Se observó una variación significativa en las puntuaciones medias de los hospitales en once dominios en la parte 1 y dieciséis dominios en la parte 2.
ConclusionesLos resultados proporcionaron una mejor comprensión de la perspectiva de los APP sobre la calidad. El FlaQuM-Quickscan es un instrumento válido para medir las experiencias de los APP en cuanto a la calidad hospitalaria. Las prioridades identificadas indican que la gestión hospitalaria debería centrarse en estrategias de calidad multifacéticas, que incluyan dominios técnicos, centrados en la persona y en la familia, valores fundamentales y catalizadores.

