





It is a priority to find surgical techniques that guarantee acceptable healing rates without sequelae in the treatment of complex anal fistula. The concept of the deep intersphincteric space as the origin of perianal sepsis has provided a new perspective, allowing the emergence of techniques such as TROPIS (Transanal Opening of Intersphincteric Space), with few published series to date. The aim of this study is to evaluate the healing rate and complications one year after the TROPIS technique as a treatment for complex anal fistula without hospitalization.
MethodProspective, observational study from January 2021 to January 2023. Patients with complex anal fistulas who met the inclusion criteria were treated using the TROPIS technique. A one-year follow up review was conducted, assessing healing rates, recurrence, continence, and complications.
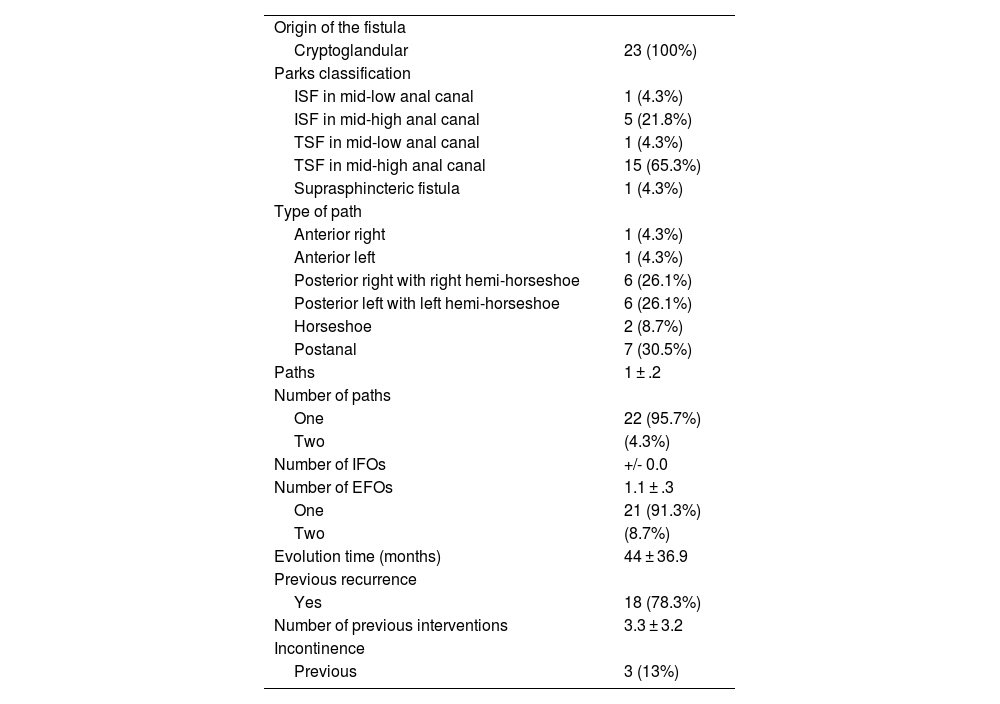
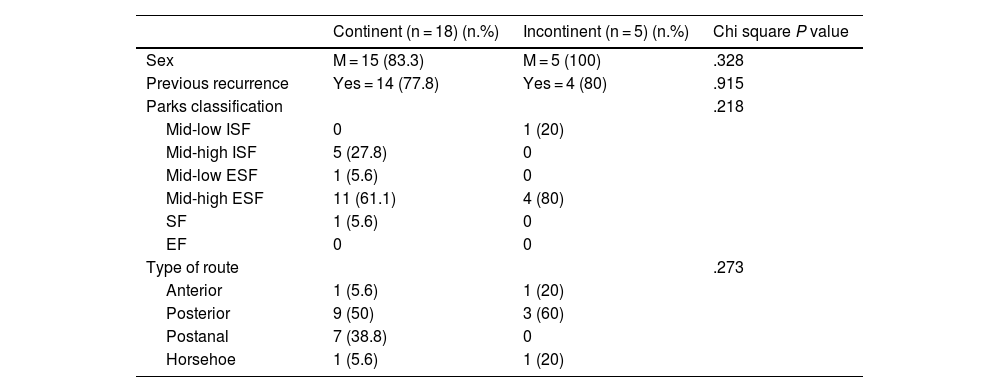
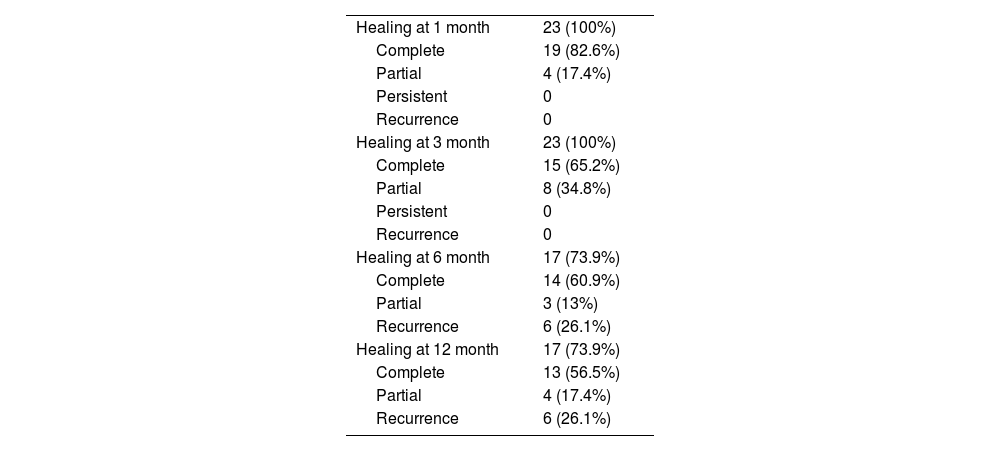
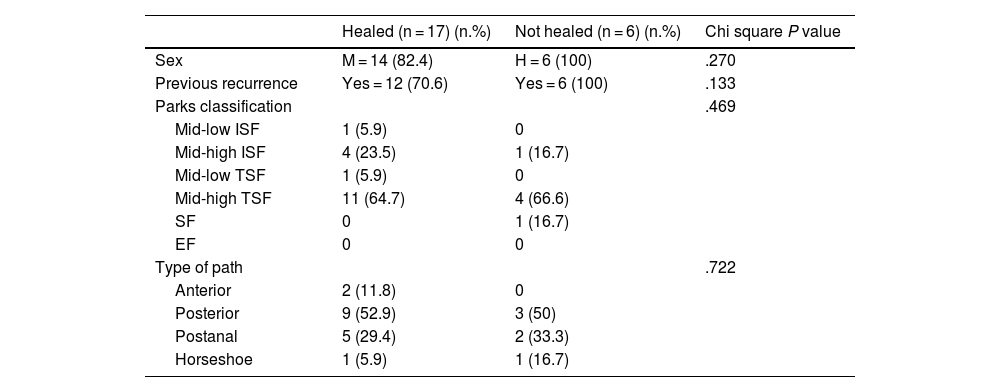
ResultsA total of 23 patients with cryptoglandular complex perianal fistula were included (87% male, mean age 54.7 ± 9.6 years). 78.3% were treated for recurrent fistulas with an average of 3.3 ± 3.2 previous interventions. At one month, 82.6% of the patients had complete healing. At three, six, and twelve months, complete healing occurred in 63.6%, 61.9%, and 55.6%, respectively. One patient developed an abscess at one month. Continence was altered in 8.7%.
ConclusionsThe treatment of cryptoglandular complex anal fistula with this procedure was safe and showed acceptable healing rates.
Es prioritario encontrar técnicas quirúrgicas que garanticen tasas de curación aceptables sin secuelas en el tratamiento de la fístula anal compleja. El concepto de espacio interesfintérico profundo como origen de la sepsis perianal ha dado una nueva perspectiva, permitiendo la aparición de técnicas como, TROPIS (Transanal Opening of Intersphincteric Space), con escasas series publicada hasta el momento. El objetivo de este estudio es valorar la tasa de curación y las complicaciones al año de la técnica TROPIS, como tratamiento de la fistula anal compleja sin ingreso.
MétodoEstudio ambispectivo, observacional, desde enero del 2021 a enero del 2023. Se trató mediante técnica TROPIS a pacientes con fístula anal compleja que cumplían criterios de inclusión. Se realizó una evaluación al año, valorando tasas de curación, recurrencia, de continencia y complicaciones.
ResultadosSe han incluido un total de 23 pacientes con fistula anal compleja criptoglandular (87% varones, edad media 54,7 ± 9,6 años). El 78,3% fueron fistulas recidivadas con una media de 3,3 ± 3,2 intervenciones previas. Al mes, un 82,6% de las pacientes tuvieron una curación completa. A los tres, seis y doce meses la curación completa se dio en un 63,6%, 61,9% y 55,6% respectivamente. Un paciente tuvo un absceso al mes. La continencia se modificó en un 8.7%.
ConclusionesEl tratamiento de la fístula anal compleja criptoglandular con este procedimiento fue seguro y mostró aceptables tasas de curación.

