








To evaluate whether a radioguided approach allows a higher intraoperative detection rate of adenoma and a minimally invasive parathyroidectomy (MIP), with the same or better cure rate of hyperparathyroidism secondary to parathyroid adenoma.
MethodsThis was an observational, prospective, single-center study involving 254 consecutive patients with primary hyperparathyroidism, between 2017 and 2022. A total of 258 procedures were performed: 129 non radioguided (NRS) and 129 radioguided (RS) (112 with intravenous 99mTc- MIBI and 17 with ultrasound-guided intralesional 99mTc-MAA injection) with an intraoperative gamma probe and gamma camera. Follow-up was performed for at least one year.
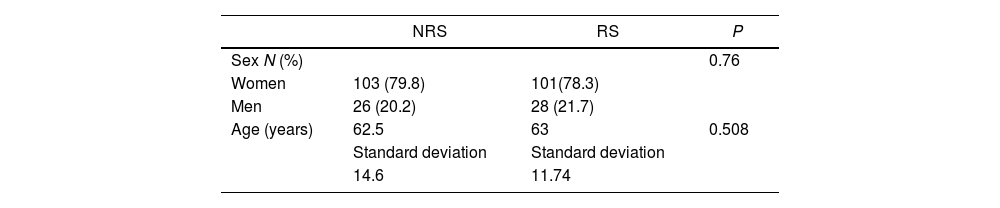
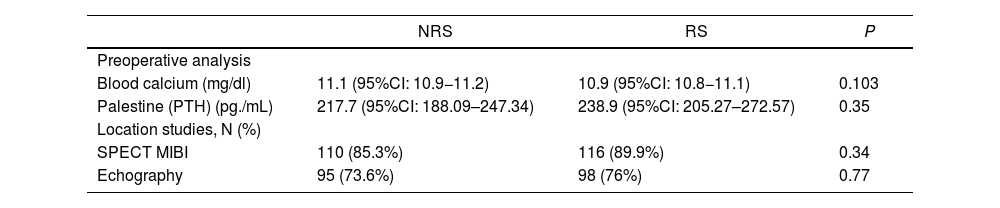
ResultsThere were no differences between the groups in terms of age, sex, preoperative calcium or parathyroid hormone levels, adenoma localization with 99mTc-MIBI-gammagraphy and ultrasound, and surgical morbidity.
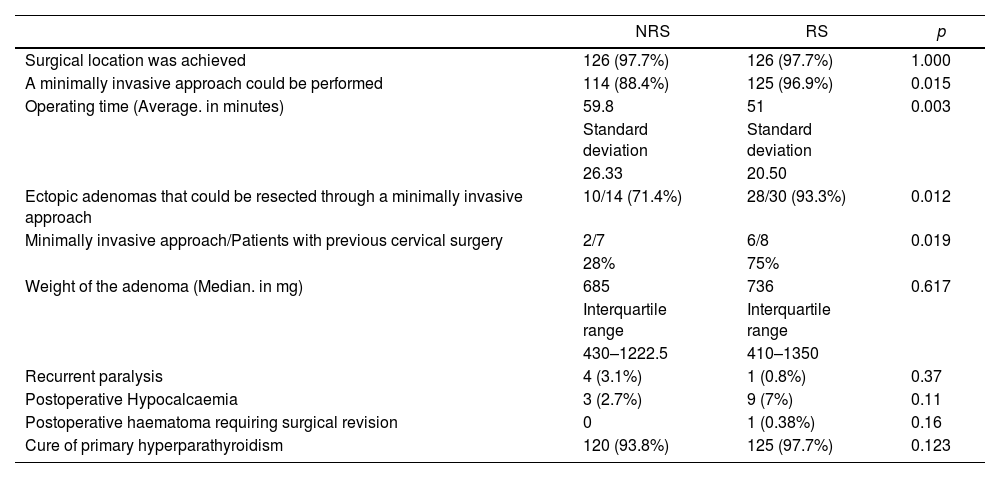
Intraoperative surgical localization was 97.7% in both groups. Statistically significant differences supported RS: It allowed to perform MIP (RS: 96.9%, NRS 88.4%; p = 0.015), also in patients with previous neck surgery (RS: 75%, NRS: 28%; p = 0.019) and with ectopic adenomas (RS: 93.3%, NRS: 71.4%; p = 0.012). The operative time was significantly shorter (RS: 51 min, NRS: 59.79 min; p = 0.005). There were no significant differences in the postoperative complications between the groups.
Biochemical cure at six months was achieved in RS: 97.7% and NRS: 93.8% (p = 0.12).
ConclusionsRadioguided MIP is useful in ectopic adenomas and in patients with previous cervical surgery and allows a minimally invasive approach more frequently. It is a safe surgery, easily reproducible by an endocrine surgeon and requires usual equipment found in operating rooms.
Evaluar si un abordaje radioguiado permite una mayor tasa de detección intraoperatoria del adenoma y una paratiroidectomía mínimamente invasiva (PMI), con la misma o mejor tasa de curación del hiperparatiroidismo primario por adenoma paratiroideo.
MetodologíaEstudio observacional, prospectivo y unicéntrico con 254 pacientes consecutivos afectos de hiperparatiroidismo primario, entre 2017 y 2022. Se realizaron un total de 258 procedimientos: 129 no radioguiados (CNR) y 129 radioguiados (CR) (112 con 99mTc- MIBI intravenoso y 17 con inyección intralesional de 99mTc-MAA) con gammasonda intraoperatoria y gammacámara. Seguimiento postoperatorio durante al menos un año.
ResultadosSin diferencias entre ambos grupos en cuanto a edad, sexo, niveles preoperatorios de calcio u hormona paratiroidea, localización del adenoma con gammagrafía con 99mTc-MIBI y ecografía, y morbilidad quirúrgica.
La localización quirúrgica intraoperatoria fue del 97,7% en ambos grupos. Diferencias estadísticamente significativas a favor de CR: Permitió realizar PMI (CR: 96,9%, CNR 88,4%; p = 0,015), también en pacientes con cirugía previa de cuello (CR: 75%, CNR: 28%; p = 0,019) o adenomas ectópicos (CR: 93,3%, CNR: 71,4%; p = 0,012). El tiempo operatorio fue significativamente menor (CR: 51 min., CNR: 59,79 min.; p = 0,005). No hubo diferencias significativas en las complicaciones postoperatorias entre los grupos.
La curación bioquímica se alcanzó en CR: 97,7% y CNR: 93,8% (p = 0,12).
ConclusionesLa cirugía radioguiada es útil en adenomas ectópicos y en pacientes con cirugía cervical previa y permite un abordaje mínimamente invasivo con mayor frecuencia. Es una cirugía segura, fácilmente realizable por un cirujano endocrino y utiliza equipamiento habitual en los quirófanos de cirugía general.

