









This study evaluates the knowledge of Spanish surgeons regarding data governance and Digital Surgery, their usage, errors, and training deficiencies, as well as differences in knowledge between those who perform robotic surgery and those who do not.
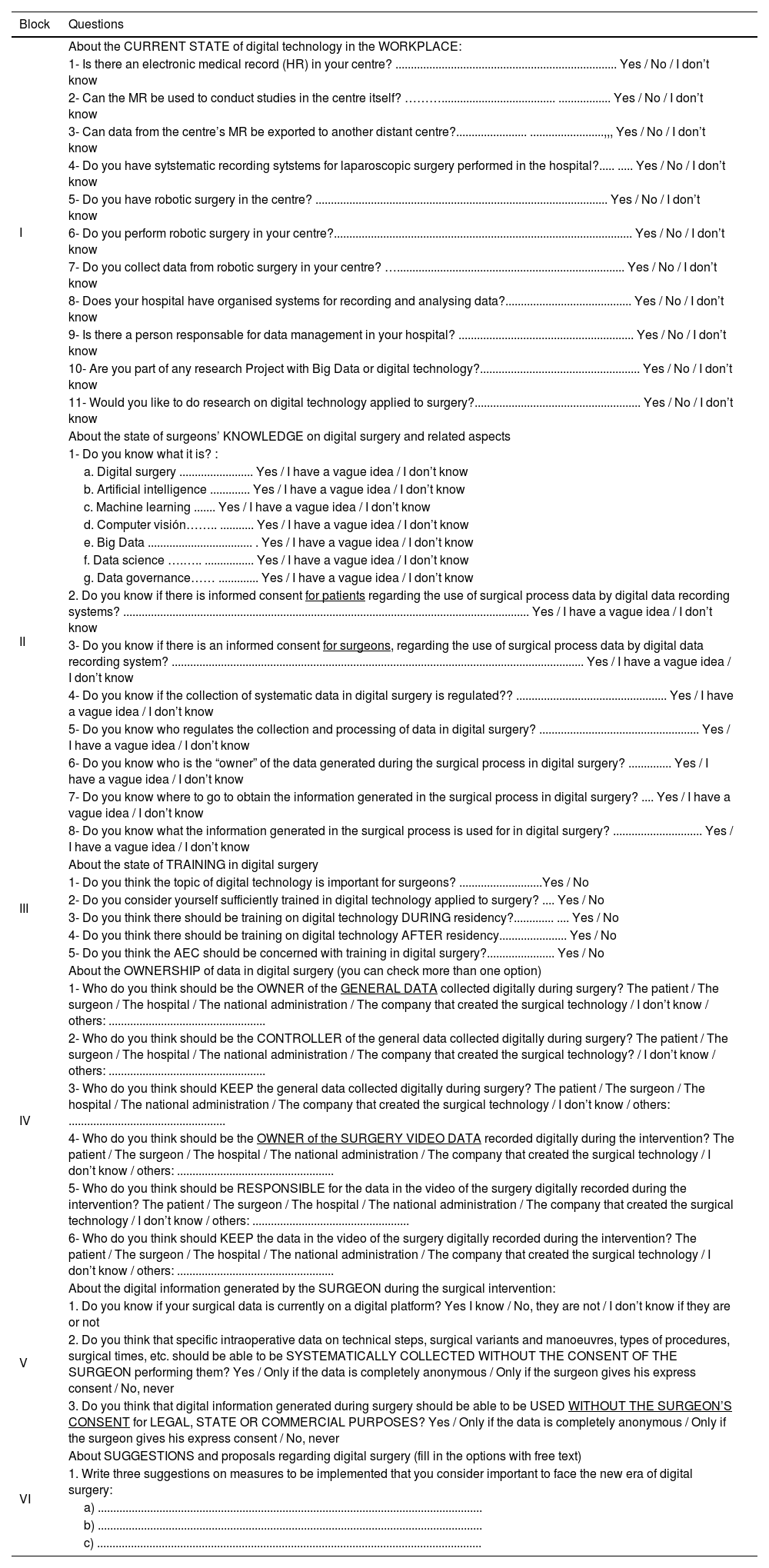
MethodsA descriptive study was conducted using a closed survey promoted by the Minimally Invasive Surgery and Technological Innovation Section of the Spanish Association of Surgeons, directed at its members between February and March 2024.
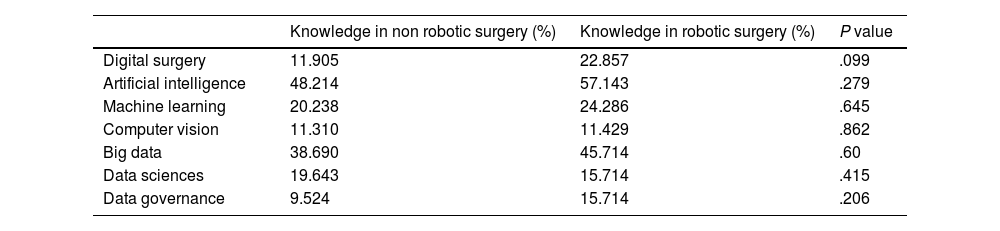
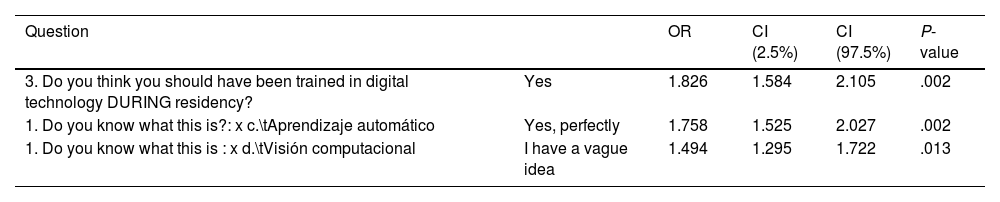
ResultsOut of 1086 surgeons contacted, 396 responded (36.46%). While 98.3% use electronic medical records, 45.4% lack organized data recording systems. Although 55.9% have access to robotic technology, 70.6% do not use it directly. Surgeons who perform robotic surgery show a higher general knowledge of Digital Surgery terms (7.2 vs 6.619; P = .215) and specifically of “Artificial Intelligence” (57.14% compared to less than 25% for other terms), although these differences are not significant. However, there are significant differences in interest in digital technology between those who perform robotic surgery and those who do not (P = .023). Additionally, surgeons who support training in digital technology during residency are nearly twice as likely to research Digital Surgery.
ConclusionSurgeons are crucial for the digital transformation in surgery, but many are poorly prepared and insufficiently involved. Those who practice robotic surgery have more knowledge and interest in digital technology, highlighting the need for improved training and governance frameworks to better integrate surgeons into the digital era.
Este estudio evalúa el conocimiento de los cirujanos españoles sobre la gobernanza de datos y la Cirugía Digital, su uso, errores y carencias formativas, así como las diferencias en conocimiento entre quienes realizan cirugía robótica y quienes no.
MétodosEstudio descriptivo mediante una encuesta cerrada, promovida por la Sección de Cirugía Mínimamente Invasiva e Innovación Tecnológica de la Asociación Española de Cirujanos, dirigida a sus miembros entre febrero y marzo de 2024.
ResultadosDe los 1086 cirujanos contactados, 396 respondieron (36.46%). Aunque el 98.3% utiliza historias clínicas electrónicas, el 45.4% carece de sistemas organizados de registro de datos. El 55.9% tiene tecnología robótica, pero el 70.6% no tiene acceso directo a ella. Los cirujanos que realizan cirugía robótica muestran mayor conocimiento general sobre términos de Cirugía Digital (7.2 vs 6.619; P = .215) y específicamente sobre «inteligencia artificial» (57.14% frente a menos del 25% para otros términos), aunque las diferencias no son significativas. Sin embargo, sí hay diferencias significativas en el interés por la tecnología digital entre quienes realizan cirugía robótica y quienes no (P = .023). Además, los cirujanos que apoyan la formación en tecnología digital durante la residencia tienen casi el doble de probabilidades de investigar sobre Cirugía Digital.
ConclusiónLos cirujanos son clave para la transformación digital en cirugía, pero muchos están mal preparados y poco involucrados. Quienes practican cirugía robótica tienen más conocimiento e interés en la tecnología digital, destacando la necesidad de mejorar la formación y establecer marcos de gobernanza para integrar mejor a los cirujanos en la era digital.

