




There are two techniques to assess the effectiveness of the management plan on glycaemic control: patient self-monitoring of blood glucose and glycated hemoglobin (HbA1c).1 This last one reflects the average glycaemia along several months and it has a strong predictive value for diabetes complications.2 However, the HbA1c test is subjected to certain limitations related to erythrocyte lifespan: hemolytic anemia, iron deficiency, blood transfusion, and hemoglobinopathies must be considered, particularly when the HbA1c result does not correlate with the patient's blood glucose levels.1
Mutations in genes encoding hemoglobin chains are present in about 7% of the worldwide population, and hemoglobinopathies are the more common single-gene genetic disorders in humans.3 These genetic alterations can affect the production rate of globin chains and cause thalassemia, or they can modify the molecule structure and generate hemoglobin variants. Hemoglobin variants are usually the consequence of a single amino acid substitution caused by point mutations in genes encoding globin chains, resulting in a tetramer with different physicochemical characteristics. Most of the hemoglobin variants described do not cause symptomatic clinical manifestations.3
Hemoglobin D was first described in 1951. The most frequent denominations found in the literature for this mutant hemoglobin are hemoglobin D-Los Angeles or hemoglobin D-Punjab. Hb D-Los Angeles contains a substitution of glutamine for glutamic acid at position 121 of the beta globin chain [β121(GH4)Glu>Gln].4 Hb D-Los Angeles is the fourth most often occurring hemoglobin variant worldwide. It is primarily found in the Punjab region of Pakistan and Northwestern India, with an estimated frequency of 2%, but is also common in persons from China, England, Holland, Australia, Greece, Yugoslavia, Turkey, etc. When Hb D-Los Angeles is inherited in heterozygous form does not present clinical or hematological alterations.4
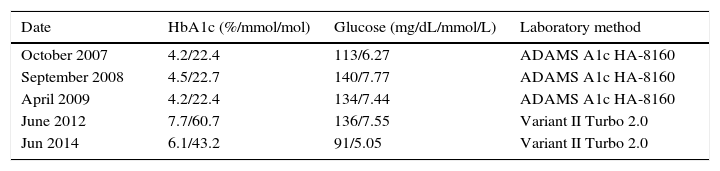
A 77-year-old white man, native from San Pedro (Albacete, Spain), with a history of diabetes type 2 for over 25 years and treated with insulin for over 15 years, was attended in our outpatient department between 2004 and 2014. He also suffered from hypertension and hypercholesterolemia and he had history of myocardial infarction. His latest medications included byphasic insulin 30/70 three times a day, atorvastatin, olmesartan, amlodipine, hydrochlorothiazide, carvedilol and aspirin. Between 2007 and 2009, using the HA-8160 for the HbA1c assay, HbA1c levels were relatively low compared to those of serum glucose (Table 1). A further molecular study showed that the patient was heterozygous for Hb D-Los Angeles [β121 Glu>Gln; HBB: c.364 G>C].
HbA1c results and laboratory method.
| Date | HbA1c (%/mmol/mol) | Glucose (mg/dL/mmol/L) | Laboratory method |
|---|---|---|---|
| October 2007 | 4.2/22.4 | 113/6.27 | ADAMS A1c HA-8160 |
| September 2008 | 4.5/22.7 | 140/7.77 | ADAMS A1c HA-8160 |
| April 2009 | 4.2/22.4 | 134/7.44 | ADAMS A1c HA-8160 |
| June 2012 | 7.7/60.7 | 136/7.55 | Variant II Turbo 2.0 |
| Jun 2014 | 6.1/43.2 | 91/5.05 | Variant II Turbo 2.0 |
The HbA1c measurement is highly method-dependent and it can be adversely affected by the presence of hemoglobin variants, which may be an incidental finding during the HbA1c analysis. An A1c deviation of 1% reflects a change of 1.4–1.9mmol/L (25–34mg/dL) in the average blood glucose concentration. Therefore, a falsely high or low HbA1c value caused by the presence of a clinically silent hemoglobin variant may lead to over- or under-treatment of diabetic patients. It has been reported a non-estimation or under-estimation of HbA1c fraction using the ADAMS A1c HA-8160 (Arkray, Kyoto, Japan) in the presence of Hb D-Los Angeles.5–9 Nevertheless, the Variant II Turbo 2.0 (Bio-Rad Laboratories, Hercules, CA), our assay method for HbA1c since 2011, do not show any clinically significant interference in the presence of Hb D-Los Angeles trait.10
In conclusion, to avoid reporting inaccurate results, laboratories should be aware of the limitations of their methods with respect to hemoglobin variants, and indicate this information in reports to physicians. On the other hand, physicians should consider the possibility of interference by an hemoglobin variant if a patient's HbA1c results is significantly different from what is expected on the basis of blood glucose self-monitoring.
