





The use of deep brain stimulation (DBS) has been recently extended for treating resistant psychiatric disorders, but the experience in patients with schizophrenia-related disorders and bipolar disorder (BD) is scarce.
MethodWe conducted an observational, one-year longitudinal study to evaluate the effects of DBS in four treatment-resistant patients with schizophrenia, schizoaffective, and BD, included in a pilot, last-resource protocol. Patients were digitally monitored for objective assessment of behavioral changes.
ResultsAfter one year of its initiation, DBS of the nucleus accumbens (in subjects N2, N3, and N4) and subgenual anterior cingulate cortex (in N1) produced a significant clinical improvement, associated with decreases in the Clinical Global Impression (from 5.25±0.5 to 3.5±1, p=0.035) and in the Hamilton Depression Rating Scale (HADRS scores, from 14.5±6.56 to 1.5±1.29, p=0.020). We observed a notable, durable therapeutic response in two patients from this cohort (N1 and N3), a clinically relevant relief in a third (N2), and a lack of a significant response in the last one (N4). Maintenance electroconvulsive therapy sessions could be discontinued in the three patients that responded to DBS (N1–3). There were no side effects or relevant changes in cognitive functioning. There were relevant differences between physical activity and sleep time among the four participants.
ConclusionsThese results suggest initial evidence that DBS may be an effective and safe alternative for treating complex and resistant forms of schizophrenia-related disorders and BD. Digital monitoring may help to capture objective measures of behavioral changes after the intervention.
Up to 30% of patients with schizophrenia and 15% with bipolar disorder (BD) are considered treatment-resistant.1,2 Although some strategies have been described for resistant forms,3–5 there is a need of new therapeutic strategies.
Deep brain stimulation (DBS) is a neurosurgical procedure originally developed for treating neurological disorders that involves the implantation of electrodes into brain subcortical nuclei or white matter to deliver electrical stimulation.6 This high frequency stimulation produces functional inhibition in the brain tissue around the electrode, while local and distant excitatory effects may also play a role.6 DBS is adjustable and can be turned-off without any permanent loss of function.
Though DBS has been extended in recent years for treating resistant psychiatric disorders with broadly encouraging results,7,8 but very few trials have been carried out in schizophrenia and BD patients. The only completed trial in schizophrenia reported significant improvement stimulating the nucleus accumbens (NAcc, n=3) and the subgenual anterior cingulate cortex (SACC, n=4), showing NAcc more benefits.9 There is also little evidence of the effects of DBS in patients with BD, being only a minority of the patients included in studies of DBS in mood disorders.7
This manuscript contains a series of the first four clinical cases treated with DBS in Hospital Clínic de Barcelona for these conditions and followed-up for one year.
Subjects and methodsParticipantsThis was an observational, one-year longitudinal study evaluating the effects of DBS in four treatment-resistant patients with schizophrenia-related disorders or BD included in a pilot, last-resource protocol.
Participants were recruited from our psychiatric facilities from 2019 to 2021. The inclusion criteria were: age 20–60 years, ≥5 years of duration of the disorder, DSM-5 diagnosis of schizophrenia, schizoaffective disorder or BD, meet criteria for treatment-resistant schizophrenia or BD,1,2 and ability to fulfill all tests and follow-up visits. The exclusion criteria were: contraindications for DBS surgery, concomitant neurological pathology, brain morphological abnormalities, and active suicidal ideation or substance use disorder.
Only patients able to fully understand the potential benefits and risks of treatment were considered for the study. All participants gave written informed consent before their inclusion. The protocol was conducted in accordance with the ethical principles of the Declaration of Helsinki (Fortaleza version, Brazil, October/2013) and in accordance with Spanish Law 14/2007 on Biomedical Research. The study was approved by the Ethics Committee of the Hospital Clínic de Barcelona.
Clinical and neuropsychological evaluationSymptom severity, quality of life and functioning levels were assessed before the surgical intervention and every month during the follow-up with the Clinical Global Impression Scale (CGI), the Positive and Negative Symptom Scale (PANSS), the Young Mania Rating Scale (YMRS), the Hamilton Depression Rating Scale (HDRS), the Quality-of-Life Scale (QLS), The WHO-5 Well-Being Index, and the Functional Assessment Short Test (FAST). Adverse drug reactions were assessed using the Udvalg for Kiniske Undersogelser (UKU) rating scale.
All patients completed a neuropsychological battery before and one year after the surgery (Supplementary info 3).
Wearable and smartphone app monitoringA smartphone app assessed daily moods symptoms and weekly mood episodes.10 A commercial wearable device (Withings Move®) passively collected the physical activity and sleep patterns.
Surgical and programming procedureAll participants underwent presurgical 3-T MRI under sedation. The stereotactic targeting was planned on the Stealth Station S8 (Medtronic®). Targets were identified using MRI-Direct visual anatomical targeting assisted by Sure Tune™ 4 (Medtronic®) pre-implant reconstructions.
All patients were operated under general anesthesia in an MRI-guided and intraoperative image-verified procedure. The procedure began affixing the Leksell-G stereotactic ring (Elekta AB®) to the patient's head.
Tetra-polar electrodes (Model 3389-40, Medtronic®) were inserted through two frontal horizontal incisions and 14mm burr holes. Each electrode position was verified intraoperatively with the O-ARM 3D fluoroscopic system (Medtronic®) through co-registration with the preoperative MRI planning (Supplementary info 1). Extension wires (7495-51cm, Medtronic®), and implantable pulse generator Activa RC37612 (Medtronic®) were placed in the lateral neck and infra-clavicle subcutaneous tissue, respectively.
Patients remained hospitalized 2–5 days without stimulation to assess the mechanical effect of the electrodes’ introduction. The initial stimulation parameters were: frequency of 130Hz, pulse width of 90μs and current intensity of 0.5V with a gradual increase up to 3V, with bipolar stimulation (contact-cathode; battery-anode). Stimulation parameters were modified individually, depending on clinical state. The sequence of changes was (1) increasing voltage up to 7.5V, (2) increasing pulse width or frequency up to 210μs/Hz, and (3) changing active contacts or mode.
Statistical methodsA one-way repeated measures ANOVA compared scores on the clinical scales at Time-1 (prior to the intervention), Time-2 (one-month follow-up) and Time-3 (one-year follow-up). Wilcoxon signed-rank test was applied to compare neuropsychological tests between Time-1 and Time-3.
Being exploratory analysis of multiple dependent and naturally correlated variables corrections for multiple comparisons were not made.11 A p<0.05 value was considered statistically significant in all analysis.
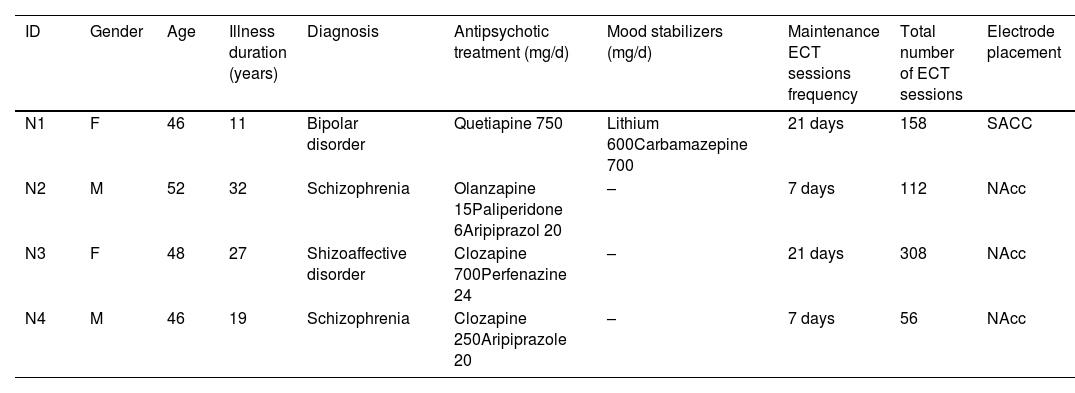
ResultsParticipants main baseline clinical and treatment characteristics and electrode placement are shown in Table 1.
Patients’ baseline characteristics and electrode placement.
| ID | Gender | Age | Illness duration (years) | Diagnosis | Antipsychotic treatment (mg/d) | Mood stabilizers (mg/d) | Maintenance ECT sessions frequency | Total number of ECT sessions | Electrode placement |
|---|---|---|---|---|---|---|---|---|---|
| N1 | F | 46 | 11 | Bipolar disorder | Quetiapine 750 | Lithium 600Carbamazepine 700 | 21 days | 158 | SACC |
| N2 | M | 52 | 32 | Schizophrenia | Olanzapine 15Paliperidone 6Aripiprazol 20 | – | 7 days | 112 | NAcc |
| N3 | F | 48 | 27 | Shizoaffective disorder | Clozapine 700Perfenazine 24 | – | 21 days | 308 | NAcc |
| N4 | M | 46 | 19 | Schizophrenia | Clozapine 250Aripiprazole 20 | – | 7 days | 56 | NAcc |
ECT: electroconvulsive therapy; F: female; M: male; NAcc: nucleus accumbens; SACC: subgenual anterior cingulate cortex.
All participants were on maintenance ECT. N3 and N4 were on clozapine treatment, while N2 had to be withdrawn twice due to the presence of neutropenia. After 12-month follow-up, no significant psychopharmacological treatment changes were registered.
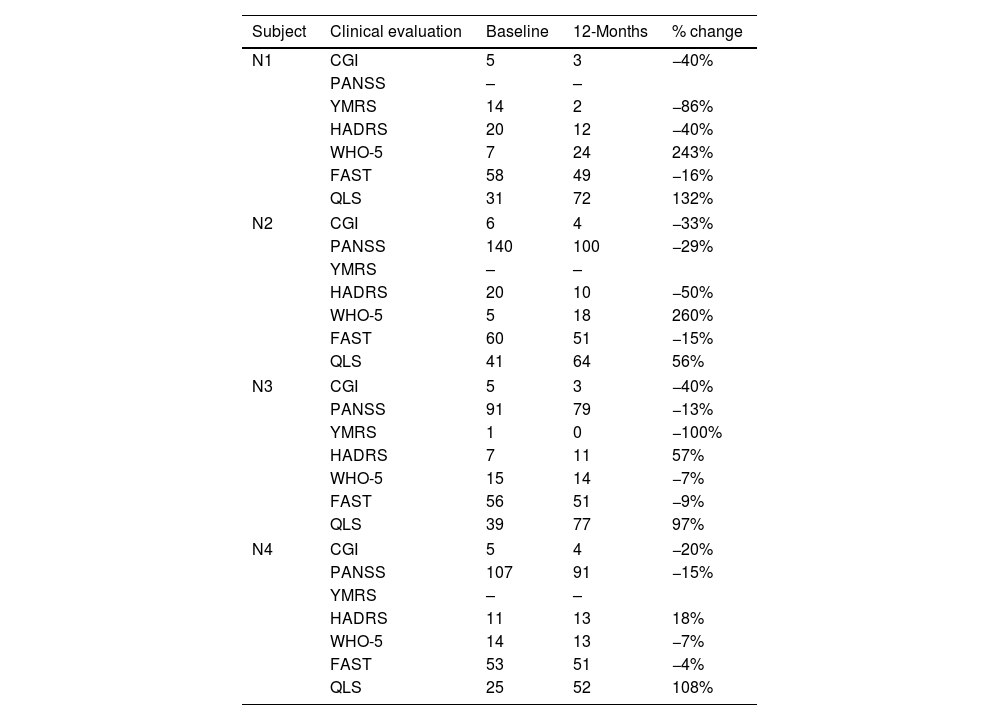
Clinical outcomesIndividual scores in clinical scales at baseline and 12 months follow-up visits are shown in Table 2.
Individual scores in symptomatic and functioning scales in the 4 patients treated with deep brain stimulation over the first 12 months of follow-up.
| Subject | Clinical evaluation | Baseline | 12-Months | % change |
|---|---|---|---|---|
| N1 | CGI | 5 | 3 | −40% |
| PANSS | – | – | ||
| YMRS | 14 | 2 | −86% | |
| HADRS | 20 | 12 | −40% | |
| WHO-5 | 7 | 24 | 243% | |
| FAST | 58 | 49 | −16% | |
| QLS | 31 | 72 | 132% | |
| N2 | CGI | 6 | 4 | −33% |
| PANSS | 140 | 100 | −29% | |
| YMRS | – | – | ||
| HADRS | 20 | 10 | −50% | |
| WHO-5 | 5 | 18 | 260% | |
| FAST | 60 | 51 | −15% | |
| QLS | 41 | 64 | 56% | |
| N3 | CGI | 5 | 3 | −40% |
| PANSS | 91 | 79 | −13% | |
| YMRS | 1 | 0 | −100% | |
| HADRS | 7 | 11 | 57% | |
| WHO-5 | 15 | 14 | −7% | |
| FAST | 56 | 51 | −9% | |
| QLS | 39 | 77 | 97% | |
| N4 | CGI | 5 | 4 | −20% |
| PANSS | 107 | 91 | −15% | |
| YMRS | – | – | ||
| HADRS | 11 | 13 | 18% | |
| WHO-5 | 14 | 13 | −7% | |
| FAST | 53 | 51 | −4% | |
| QLS | 25 | 52 | 108% | |
CGI: Clinical Global Impression; PANSS: Positive and Negative Symptom Scale; YMRS: Young Mania Rating Scale; HADRS: Hamilton Depression Rating Scale; WHO-5: WHO-5 Well-Being Index; FAST: Functional Assessment Staging; QLS: Quality-of-Life Scale.
Affective patients N1 (BD) and N3 (schizoaffective disorder) reached clinical stabilization with voltages of 3.8 and 3.5V, respectively. N1 specially improved in affective symptoms and N3 in psychotic and general symptoms. N2 (schizophrenia) needed 4.5V for presenting a mild clinical response. These three patients could stop ECT sessions after the DBS activation.
Patient N4 (schizophrenia) showed no relevant response to DBS, despite increasing voltage to 7V. He required two hospital admissions during follow-up and 59 more ECT sessions, similarly to the previous years before the surgical intervention. The pulse generator was turned-off for each ECT session and reactivated after 2h.
An ANOVA analysis compared the group scores on the clinical scales over three visits, showing a significant effect for CGI and HADRS scores, and a statistical tend for QLS (Supplementary info 2).
No significant cognitive decline was seen after DBS surgery (Supplementary info 3).
Smartphone app and wearable resultsThe use of the smartphone app among the 3 participants who were able to install it was inconsistent and poor (only 7 tests completed, average use of 13 days).
The four participants used the wearable device (mean time: 87.25 days). There were relevant differences between physical activity and sleep time among them (Supplementary info 4).
Surgical and adverse effects resultsMean surgical time was of 230min (±27) and mean hospital stay length of 5 days (3–8). No adverse effects related to the surgery, the implanted hardware or to neurostimulation were registered.
No significant changes were detected in medication-related side effects recorded with the UKU scale, remaining at a mean average score of 2 (±4) one month after surgery and decreasing to 1.25 (±1.89) at 12 months.
DiscussionWe present a case series of four patients with treatment-resistant schizophrenia and BD treated with DBS, included in a pilot, last-resource protocol. At the one-year follow-up we observed: (i) A notable and durable therapeutic response in two patients (N1 and N3), a clinically relevant relief in a third (N2) and a lack of a significant response in the last one (N4); (ii) Maintenance ECT could be discontinued in the three responders to DBS, while it was reintroduced in the non-responder participant, without any particular incidence of security; (iii) No surgery related complications or side effects appeared; (iv) No relevant changes in cognitive functioning; (v) Relevant differences between physical activity and sleep time among participants.
Available, limited literature points out to DBS effectiveness for certain serious mental disorders. In the only clinical trial reported so far of DBS in schizophrenia, 4/7 patients met the study symptomatic improvement criteria.9 Similarly, different meta-analysis show that DBS seems effective in reducing resistant depressive symptoms in samples including few BD patients.8,12
Individualizing both the location and the stimulation programming is a key aspect in DBS application. According to available literature, we decided to stimulate SACC in the patient with predominant affective symptoms (N1), while in the rest of participants, where psychotic symptoms predominated, it was decided to stimulate NAcc.8,9 The stimulation plan was designed based on our previous experience using for DBS in neurological diseases and other published protocols with psychiatric patients.9,13 There is initial evidence indicating individual variations in the clinical response to electrical dosing of DBS in depression,13 pointing that future modifications of the stimulation parameters or of the contact locations could improve initial poor clinical responses.
An innovation in the present study was the use of digital monitoring. Though digital tools proved useful only for passive capturing data, the combination of neuromodulation techniques and digital innovation may help to advance in the precision psychiatry paradigm.14
Some limitations should be considered. Firstly, the small sample size. Secondly, the cohort heterogeneity in terms of diagnosis and DBS targets. Thirdly, the relatively short duration of follow-up. Fourthly, studying last resort therapies could generate expectation bias. Finally, the lack of multiple comparisons analysis could limit the interpretation of the grouped findings.
The possibility of finding therapeutic alternatives, such as DBS, for the treatment of resistant forms of schizophrenia and BD raises great interest. This study, along with others, may open the door to a new therapy for these disorders, eventually helping to incorporate these treatments into the daily clinical practice.
Authors’ contributionsMB collected the clinical data, managed and analyzed the clinical data and wrote the first version of the paper; JR & PR collected the neurosurgical data and wrote the first version of the paper; LM collected the neuropsychological data and wrote the first version of the paper; DHM collected the wearable and apps data and wrote the first version of the paper; all the authors contributed to the final version of the paper.
FundingThis project was totally funded by the Pons-Balmes family legacy donated to the Psychiatry Department at the Hospital Clínic de Barcelona.
Conflicts of interestMB has been a consultant for, received grant/research support and honoraria from, and been on the speakers/advisory board of has received honoraria from talks and/or consultancy of Adamed, Angelini, Casen-Recordati, Exeltis, Ferrer, Janssen, Lundbeck, Neuraxpharm, Otsuka, Pfizer and Sanofi, and grants from Spanish Ministry of Health, Instituto de Salud Carlos III (PI20/01066).
JGB has received financial support for educational activities from Takeda, Lundbeck, and Janssen. JGB has served as a consultant or provided teaching materials to Janssen, Sanofi and Casen Recordati.
DHM received CME-related honoraria and participation on advisory boards from Abbott, Angelini, Janssen-Cilag and Ethypharm with no financial or other relationship relevant to the subject of this manuscript.
EP has received honoraria and/or research grants and/or financial support for the Basic and Translational Research Laboratory in Schizophrenia from the following entities and companies: Fondo de Investigación Sanitaria of the Spanish Ministry of Science and Innovation, the Catalan Pons Balmes Grant, Fundació la Marató de TV3 of Catalonia, Relats, Assegurances Santasusana, Fundació Vila-Saborit, Janssen-Cilag, Adamed, Rovi, Lundbeck-Otsuka, Angelini, Sanofi, Kern, Casen Recordati, Glaxo-Smith Kline, Ferrer, Takeda, Biogen, GWAP and Acadia.
JR has been a consultant for, received grant/research support and honoraria from, and been on the speakers/advisory board of has received honoraria from talks and/or consultancy of Medtronic and Boston Scientific, with no financial or other relationship relevant to the subject of this manuscript.
EV has received grants and served as consultant, advisor, or CME speaker for the following entities: AB-Biotics, AbbVie, Adamed, Angelini, Biogen, Boehringer-Ingelheim, Celon Pharma, Dainippon Sumitomo Pharma, Ferrer, Gedeon Richter, GH Research, Glaxo-Smith Kline, Janssen, Lundbeck, Merck, Novartis, Orion Corporation, Organon, Otsuka, Rovi, Sage, Sanofi-Aventis, Sunovion, Takeda, and Viatris, outside the submitted work.
The rest of the authors report no biomedical financial interests or potential conflicts of interest.
Authors want to thank Dr. Valldeoriola, neurologist at the Parkinson's Unit of the Hospital Clínic de Barcelona, for his advice and sharing his experience on DBS in the initial phase of the project and Monica Farrés for the technical assistance throughout the project. Dr. Hidalgo-Mazzei's research is supported by a Juan Rodés JR18/00021 granted by the Instituto de Salud Carlos III (ISCIII).
The following are the supplementary data to this article:
