














Early treatment of skeletal class II malocclusions with functional orthopedics is a useful means that together with a correct diagnosis, treatment plan and patient cooperation may lead to reducing or eliminating the need for surgery in the future to treat the patient's problem. Functional orthopedic appliances such as the Bionator promote the adaptive ability of the tissues especially during the early growth spurt and may improve the profile and the skeletal relationship.
El manejo temprano de las maloclusiones clase II esquelética con ortopedia funcional de los maxilares es una herramienta que, con el correcto diagnóstico, plan de tratamiento y colaboración del paciente, permite disminuir o eliminar una cirugía a futuro para la corrección de dicho problema. Los aparatos ortopédicos funcionales como el Bionator potencian la capacidad adaptativa de los tejidos especialmente durante el periodo de pico de crecimiento mejorando el perfil y la relación esquelética.
Treatment of malocclusions in early ages is becoming increasingly prevalent in current orthodontics. Functional maxillary orthopedics (FMO) provides different therapies that facilitate the correction of malocclusions by establishing a correct function and harmony of the jaws.
FMO is the science that comprises a set of therapeutic means which contribute essentially in the use of forces or movements that arise during the execution of the physiological actions such as chewing, swallowing, breathing, phonation and facial adaptation in order to obtain a morpho-functional balance of the structures of the stomatognathic system.1
FMO guides the normal maxillofacial development of growing patients through the use of appliances that cause favorable tissue changes, solving the imbalance caused by malocclusions in the transverse, sagittal and/or vertical planes.1
Malocclusions are alterations in bone growth of the maxilla, the mandible and/or of dental positions that prevent the correct function of the masticatory apparatus.2
When considering as a whole the growth of the maxilla and the mandible, these are perfectly synchronized in pace and intensity while maintaining a class I relationship throughout the evolutionary process.3
Early intervention of malocclusions was defined by Moyers as the orthodontic therapy performed during the most active stages of craniofacial, skeletal and dental growth with the purpose of changing the skeletal and dental anomalies.4
One way to treat malocclusions at early ages is by means of functional orthopedic appliances, which have a bimaxillary anchorage and do not depend exclusively on dental support.5
The Bionator appliance is a functional appliance that was described in 1952 by Balters, as a comprehensive functional device, named by the Balters himself as a «vital alarm clock».6
According to Balters there should be a balance between the tongue and the perioral mechanism with anterior lip closure for respiration, responsible for the development of the arches and intercuspation.7
The appliance is used for the correction of Class II malocclusions with dental protrusion and maxillary collapse (standard Bionator), class IIIs (reverse Bionator) and open bite (open bite Bionator) (Figure 1).8

The standard Bionator appliance is a small device that covers the lingual faces of the lower teeth from molar to molar, extends to the upper jaw taking the lateral teeth up to the canines. The acrylic involves only the occlusal faces from the lingual cusps and 4mm of the alveolar processes.8
The palatal spring is the 1.2mm wire Coffin, which helps to keep the tongue on the palate, therefore stimulating the expansion of the maxilla. The labial arch is done in 0.9mm wire, crosses from the palate to the labial surface in search of the contact point between the canine and the upper premolar, directing towards the gingiva at the height of the middle third of upper premolar, then distally, up to the mesial third of the first molar, forming a wide loop that extends towards the middle third of the first lower premolar continuing distal to the canine; there the wire is bent in the form of bayonet coming up to the incisal third of upper incisors and canine, continuing symmetrically on the opposite side.8
The therapeutic postural change caused by the appliance must be done within the individual physiological limits with the contact of the incisors in a determined area (DA).5
DA will be determined by the contact in the upper third of the labial and palatal faces of the upper and lower incisors.5
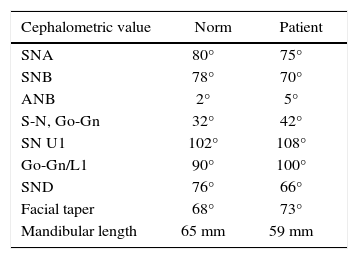
CASE REPORTA female patient of 6 years of age attended the Medical Specialties Clinic of the State of Veracruz «Dr. Rafael Lucio» (CEMEV-UNAM) in 2010 with the reason for consultation referred by the mother: «My daughter does not bite evenly». Upon performing the diagnosis, the patient showed a skeletal class II due to mandibular retrusion, convex profile, bilateral molar class II, non-assessable canine class because the patient had a mixed dentition, vertical growth direction, open bite and lip suction, digital and lingual thrust habits (Figures 2 to 4andTable I).



At the end of 2012, the habits were removed by placing a lingual crib and a lip bumper (Figure 5). We proceeded to treat the skeletal class II.

The patient presented an 8mm overjet that may be observed in figure 6.

The treatment plan consisted in the placement of the Standard Bionator appliance; treatment was performed in two phases (each of six months) where each Bionator appliance had a DA record of 4mm, in order to exercise a physiologic postural change and correct the 8mm overjet (Figures 7 and 8).


Among the obtained results there was the profile change (from convex to straight) and re-direction of the vertical growth. Upper and lower dental proclination was reduced.
Treatment with the Bionator appliance lasted one year and subsequently remained under retention that consisted in the use of the Bionator appliance by night.
Figures 9 to 12 show a comparison between the initial and final frontal, profile and intraoral photographs respectively. The figures show how the patient began, her evolution with the use of the Bionator appliance and the retention stage.




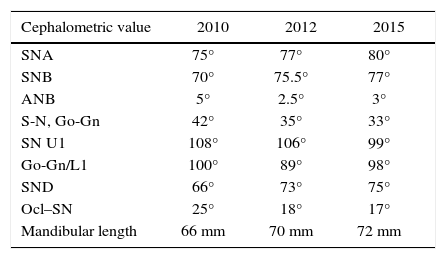
Table II shows the cephalometric data.
CONCLUSIONFMO is an alternative in the treatment of growing patients for the correction of dento-skeletal malocclusions in the transverse and sagittal plane.
Treatments with orthopedic appliances, in this case the Bionator favors a postural change in the mandible, and redirects maxillary growth.