





To study the relationship between the appearance of end-of-stem pain with a preoperative decrease in local bone strength by using the bone microindentation technique. The potential usefulness of pressure algometry in the diagnosis and monitoring of this group of patients is also determined.
Materials and methodsA preliminary intra- and inter-rater correlation study was performed in a group of 50 healthy volunteers in order to validate the algometry technique. A prospective study was then conducted on 20 patients with a mean age of 74 years (range 57–84) undergoing knee prosthetic surgery with use of a cementless tibial stem. Bone microindentation and pressure algometry measurements were made preoperatively, and after one year of follow-up. The statistical analysis was performed using the Intraclass correlation coefficient and the Student's t-test for paired data.
ResultsThe intra- and inter-rater correlation values were excellent; 0.91 (0.84–0.95) and 0.86 (0.74–0.92), respectively. No significant variations were found in the microindentation (P=0.11) or in the pressure algometry (P=0.6) values after one year of follow-up. Nevertheless, a significant correlation was observed between the values for pressure algometry and the EVA (P=0.002) and functional scale (P=0.02) at the end of follow-up.
ConclusionsPressure Algometry is a useful tool to evaluate this group of patients. Bone microindentation does not seem to be useful in identifying patients with increased risk of developing tibial end-of-stem pain.
Valorar la relación entre la aparición de dolor en punta de vástago tibial con una disminución de la resistencia ósea preoperatoria mediante microindentación ósea. En segundo lugar, conocer la utilidad potencial de la algometría de presión en el diagnóstico y seguimiento de este grupo de pacientes.
Material y métodoSe realizó un estudio de correlación intra- e interobservador preliminar, para validar el método de la algometría en un grupo de 50 voluntarios sanos. Posteriormente se realizó un estudio prospectivo en un grupo de 20 pacientes con una media de edad de 74 años (57–84), sometidos a cirugía protésica de rodilla con utilización de un vástago tibial no cementado. Se realizaron mediciones de microindentación y algometría preoperatoriamente y después de un año. Para el análisis estadístico se utilizó el coeficiente de correlación intraclase y la t de Student para datos apareados.
ResultadosEn el trabajo preliminar, los valores de correlación intra- e interobservador obtenidos fueron excelentes; 0,91 (0,84–0,95) y 0,86 (0,74–0,92), respectivamente. En el grupo prospectivo no se observaron modificaciones significativas en los valores de microindentación (p=0,11) ni algometría (p=0,6) después de un año. Se observó una correlación significativa entre los valores de la algometría y las escalas de EVA (p=0,002) y funcional (p=0,02) en el control anual.
ConclusionesLa algometría de presión fue una herramienta útil en el seguimiento de estos pacientes. La microindentación no fue adecuada para identificar pacientes en situación de riesgo de presentar dolor en punta de vástago tibial.
One of the complications reported in relation to the use of cementless tibial stems in revision knee surgery is the onset of localized pain in the tip of the stem, which appears in 11–18% of the cases according to the different series.1–4 One of the reasons proposed for this disorder is a decrease in bone mineral density (BMD) in the proximal tibia following the placement of the tibial stem due to an alteration of load transmission directly onto the distal end of the implant,4,5 which in most cases is associated to a reinforcement reaction of the bone cortex at that level. It is currently unknown whether a decrease in preoperative tibial bone mechanical resistance could be considered as a risk factor for the onset of pain in the tibial stem tip. One of the techniques used recently in clinical practice to measure bone strength is microindentation, which, when applied on the tibial diaphysis, has proved useful in differentiating patients with increased risk of osteoporotic fracture.6 The first objective of the present study was to assess the relationship between the onset of pain in the tip of the tibial stem and a decrease in preoperative bone resistance using the microindentation technique.
There is no objective and reproducible method which can measure pain in the tip of the tibial stem. Most published series are based on nonspecific assessment systems,7–9 or they combine the use of a function and satisfaction test with anatomical diagrams in which patients locate the painful point.3,4 In this sense, pressure algometry is a noninvasive technique developed several decades ago, which employs progressive pressure stimuli in order to define the pain threshold at a certain point of the human body.10 The test stops when patients consider the pressure to be painful and the pain threshold at that point is recorded, usually in kilopascals (kPa). In recent years, the emergence of digital algometers has allowed greater measurement accuracy and the technique has been used to study various musculoskeletal disorders,11–13 but never for the study of pain in the tip of the tibial stem. The second objective of the study was to assess the potential use of pressure algometry in the diagnosis of pain in the tibial stem tip, and for the monitoring of patients with cementless tibial stems.
Materials and methodsThe study was divided into two parts. The first part studied intra- and interobserver correlation of pressure algometry applied on the tibial diaphysis among a group of 50 healthy volunteers by 2 researchers who had previously received training in the pressure algometry technique. The second part comprised a prospective study among a group of 25 patients awaiting an intervention to place a knee prosthesis with a cementless tibial stem. Both the healthy volunteers in the preliminary study and the patients in the prospective monitoring group received an information sheet and signed an informed consent form prior to their participation in the study. The work was approved by the Ethics Committee of our hospital, with reference number 2012/5058/I.
Preliminary study of intra- and interobserver correlationThe study included a total of 50 volunteers (27 females and 23 males) who gave their consent. The pain threshold for each patient was determined using an electronic pressure algometer, with a spherical head of 1cm2 surface and a predefined pressure increase of 20kPa/s (Algometer®, Somedic Sales, Hörby, Sweden). Measurements were recorded at 13.5cm of the internal joint interline (Fig. 1). This distance was decided after reviewing the last 50 cases of knee revision surgery at our department. We used 2 prosthesis models (Triathlon TS Stryker® and LCCK Zimmer®) and 100mm long stems in 94% of the cases. We added 35mm to this length, considering a length of 25mm for the tibial component and 10mm for the polyethylene. At that point we marked a circle on the skin in the anteromedial side of the tibia to define the point of study. During the measurement, the algometer increased the pressure at a rate of 20kPa/s until such time as the volunteer experienced local pain and decided to end the test. At this point, the pain threshold in kPa was recorded in the apparatus. Based on the study by Nussbaum and Downes,14 the final value of the pain threshold was the mean result of the second and third measurements, since the initial measurement was considered as a test. Each researcher recorded the threshold twice, with an interval of 3–6h between them. All the values were recorded in a database by a third researcher. The study of the three measurements by the two observers yielded intra- and interobserver correlation values. The intraclass correlation coefficient (ICC) was classified as poor (<0.4), moderate (0.4–0.75) or excellent (>0.75).15
Prospective study
The prospective study included an initial group of 25 patients (13 females and 12 males) awaiting placement of a knee prosthesis with a cementless tibial stem. Inclusion criteria were patients suffering pain of an unknown origin in a primary prosthesis, aseptic loosening of a primary total knee prosthesis or severe deformity of the limb candidate for treatment by total knee prosthesis with a tibial stem. As exclusion criteria we considered patients following medical treatment for osteoporosis during the inclusion period or cases with severe metaphyseal bone defect (type III in the Anderson Orthopedic Research Institute classification).
The microindentation protocol comprised several steps. An Osteoprobe® type microindentator (Active Life Scientific, Santa Barbara, California, USA) was used. After antiseptic preparation of the skin in the studied area, the device was positioned with maximum perpendicularity with respect to the tibial diaphysis (Fig. 2). At that moment, the instrument applied an initial force of 11N to traverse soft tissues and reached the cortical surface. Subsequently, it applied an impact of 18N for 1ms to evaluate the indentation distance. Several measurements in the tibial diaphysis were taken in each case and the final value was the result of their arithmetic mean. The test lasted less than 10min and no complications associated with it have been described so far.

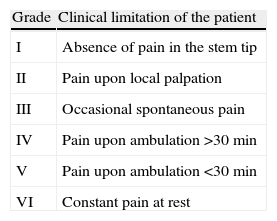
We recorded algometry and microindentation results both preoperatively and 1 year after the intervention. Algometry was applied on the tip of the stem, contralateral tibia and under the clavicle. Microindentation measurements were taken at the level of the stem tip and at the contralateral and ipsilateral tibial diaphysis. In addition, demographic data such as age, gender, BMI and medical and surgical history of interest were also recorded. In the postoperative management we employed VAS and clinical-functional scales specifically designed for the study (Table 1) to assess pain in the tip of the stem.
Clinical–functional scale used to assess pain in the tip of the tibial stem.
| Grade | Clinical limitation of the patient |
| I | Absence of pain in the stem tip |
| II | Pain upon local palpation |
| III | Occasional spontaneous pain |
| IV | Pain upon ambulation >30min |
| V | Pain upon ambulation <30min |
| VI | Constant pain at rest |
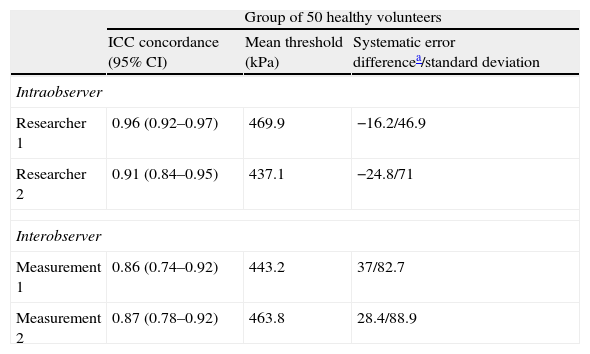
The mean age of the group was 47 years (range: 30–63 years). The mean value of the pain threshold in the tibial diaphysis was 453.5kPa. The values obtained for intra- and interobserver correlation were excellent in all cases, and no systematic error was found in the results summarized in Table 2.
Correlation values obtained in the preliminary group of healthy volunteers.
| Group of 50 healthy volunteers | |||
| ICC concordance (95% CI) | Mean threshold (kPa) | Systematic error differencea/standard deviation | |
| Intraobserver | |||
| Researcher 1 | 0.96 (0.92–0.97) | 469.9 | −16.2/46.9 |
| Researcher 2 | 0.91 (0.84–0.95) | 437.1 | −24.8/71 |
| Interobserver | |||
| Measurement 1 | 0.86 (0.74–0.92) | 443.2 | 37/82.7 |
| Measurement 2 | 0.87 (0.78–0.92) | 463.8 | 28.4/88.9 |
95% CI: 95% confidence interval; ICC: intraclass correlation coefficient.
Out of the initial group of 25 patients, 5 did not attend the second microindentation or algometry control (they reported excessive local pain during one of the tests), and were excluded from the series, which finally included 20 patients. The mean age was 74 years (range: 57–84 years) and the mean BMI was 30.8 (range: 23.1–42.4). The reasons for placing a cemented tibial stem were aseptic prosthetic loosening in 13 cases, painful prosthesis without radiographic signs of loosening in 4 cases and primary severe deformities in 3 cases.
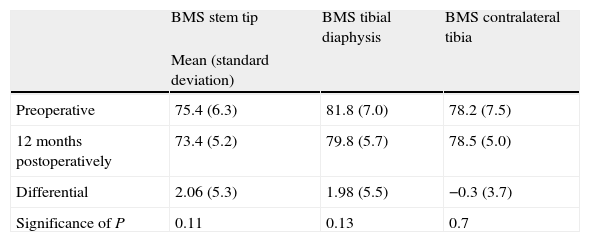
No significant changes were observed in the microindentation values 1 year after the intervention. The values obtained are summarized in Table 3. Neither was a significant correlation observed between the change in the microindentation values and the BMI (P=0.4) or the age of the patients (P=0.2).
Evolution of the microindentation values in the 3 study points 1 year after the intervention.
| BMS stem tip | BMS tibial diaphysis | BMS contralateral tibia | |
| Mean (standard deviation) | |||
| Preoperative | 75.4 (6.3) | 81.8 (7.0) | 78.2 (7.5) |
| 12 months postoperatively | 73.4 (5.2) | 79.8 (5.7) | 78.5 (5.0) |
| Differential | 2.06 (5.3) | 1.98 (5.5) | −0.3 (3.7) |
| Significance of P | 0.11 | 0.13 | 0.7 |
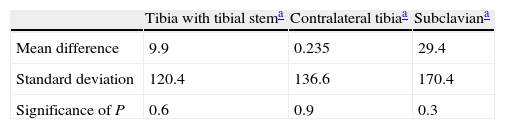
Regarding the values obtained with the algometry technique, these did not suffer significant changes after 1 year. The results are summarized in Table 4.
The mean values of the VAS functional scale at the level of the stem tip 1 year after the intervention were 2.2 (1–5) and 5.38 (0–8), respectively. Furthermore, a significant correlation was observed between the values of algometry after 1 year and the VAS scale (P=0.002) with the clinical-functional scale (P=0.02). None of the patients in the series was intervened due to pain in the tibial stem tip during the follow-up period.
DiscussionIn the preliminary correlation work, pressure algometry applied at the level of the tibial diaphysis presented excellent intra- and interobserver correlation values. These results matched those obtained by other authors who used the same technique applied to different anatomical regions. Wilgen et al.12 studied the correlation values applied to patellar tendinopathy among a group of volleyball players, obtaining intra- and interobserver correlation values of 0.6 and 0.93, respectively. These authors concluded that the technique could be useful for the diagnosis and assessment of treatment outcomes in this group of patients. Farasyn et al.16 obtained intra- and interobserver correlation values of 0.98 and 0.97, respectively, in a group of patients with nonspecific lumbar pain. Other authors reported similar correlation values using the algometry technique in different locations, such as the dorsal interosseous musculature, head, neck, deltoid and middle finger.17,18 In this regard, the results obtained by the preliminary study were consistent with those described previously in the literature for other anatomical locations, and this confirmed that algometry was a valid technique for the study of pain in the tibial diaphysis.
Regarding the prospective study group, we observed no significant changes in the pain thresholds measured by algometry after 1 year of follow-up. To date, the literature contains no studies with similar characteristics. However, there are similar series which have used pressure algometry to study postoperative pain in knee prostheses or for therapeutic assessment of patellar tendinitis. In the first case, Lunn et al.19 linked early mobilization after knee arthroplasty with less postoperative pain. In a study comparing a group of 54 jumpers with symptomatic patellar tendinopathy and a control group of 20 subjects with no pain, Wilgen et al.12 found significant differences in the algometry values of both groups, and also used the technique to study their evolution after applying specific treatment. Fredberg et al.13 also used algometry in a group of 24 patients with patellar tendinopathy and 24 with Achilles tendinopathy to study the results of corticosteroid injections compared to a placebo group. These authors also concluded that algometry was a useful technique for the diagnosis and assessment of treatment outcomes. In our series, although none of the patients required surgery due to pain in the tip of the stem, two subjects presented a value of five in the functional scale (tibial pain with ambulation under 30min). Considering these two cases as “established” stem tip pain, the percentage in our series would be of 10%, and would therefore justify not influencing the values of the entire series significantly. On the other hand, based on the previous work by Fisher,20 we consider as clinically relevant changes those differences of over 200kPa between the preoperative pain threshold and the values obtained after 1 year of follow-up. In our series, although the two cases mentioned presented a decrease over 200kPa in the pain threshold, the mean values of the series did not present significant changes. Nevertheless, algometry showed a significant correlation with the VAS and functional scale values obtained after 1 year and, therefore, we believe it can be considered useful. In addition, it also offers greater measurement precision and is a less “patient dependent” test. It is likely that a larger sample or else the specific study of a group of patients with established stem tip pain would improve the accuracy of these results.
Regarding the bone microindentation values obtained, we did not find significant changes 1 year after surgery. We could not establish a relationship between the microindentation preoperative values and the onset of pain at the stem tip. To date, there is scarce literature regarding the clinical use of bone microindentation. In their work using the same indenter at the level of the tibia, Díez-Pérez et al.6 observed significant differences when studying a group of 20 patients with osteoporotic fracture compared to a control group without osteoporosis. In the same line, Güerri-Fernández et al.21 found no significant differences in the tibial microindentation values when they compared a group of patients who had suffered an osteoporotic fracture of the proximal femur with others who had received long-term treatment with bisphosphonates and who had suffered an atypical diaphyseal fracture associated with this treatment, thus indicating that microindentation detected a deterioration of the material properties of bone which was not identified by densitometry. It is likely that, in our series, studying a complication which only appeared clinically in 10% of the cases impacted the overall results. Another possible explanation for the absence of changes in the material properties of external cortical bone could be the fact that the microstructural changes took place more significantly in the internal part of the cortical bone in contact with the stem, as opposed to the surface. However, based on the results obtained in this preliminary group, we cannot recommend the use of this technique for the diagnosis and detection of patients at risk of suffering pain in the tip of the tibial stem.
Limitations of the studyOne of the weaknesses of the preliminary correlation study was the impossibility to carry out blind measurements, since the pressure increase at a rate of 20kPa/s required observing the algometer screen and, therefore, the measurement was not blind.
Secondly, the recording of measurements at 13.5cm of the joint interline was based on a fixed length of the tibial stem of 100mm and a tibial component of 25mm. However, different polyethylene widths or else the use of offset for the stem could significantly alter the distance between the joint interline and the tip of the stem.
Regarding the prospective group, another limitation to take into account is the fact of having studied a complication with a relatively low incidence, using a small group of patients. It is likely that an increase in the sample size would help to define the results obtained more accurately.
ConclusionsPressure algometry presented an excellent intra- and interobserver correlation when applied to the tibial diaphysis, and was as useful to measure pain in the tip of the stem as VAS and functional scales. Bone microindentation did not prove to be a useful technique in identifying patients at risk of suffering pain in the tip of the tibial stem.
Level of evidenceLevel of evidence II.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation adhered to the ethical guidelines of the Committee on Responsible Human Experimentation, as well as the World Medical Association and the Declaration of Helsinki.
Confidentiality of dataThe authors declare that they have followed the protocols of their workplace on the publication of patient data and that all patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare having obtained written informed consent from patients and/or subjects referred to in the work. This document is held by the corresponding author.
FundingThis project obtained a grant from the Spanish Society of Orthopedic Surgery and Traumatology (SECOT) as part of the Research Projects of SECOT Foundation in 2011. The results of the study were presented at the last SECOT Congress held in Barcelona in 2013.
Conflict of interestsThe authors have no conflict of interests to declare.
The authors thank SECOT Foundation for their sponsorship through a Research Project grant in 2011, as well as Sergi Mojal, for his valuable advice and help with the statistical study.
Please cite this article as: Pelfort X, Güerri RC, Sanchez JF, Dürsteler C, Valverde D, Hinarejos P, et al. Técnica de microindentación ósea y algometría de presión aplicada al recambio protésico de rodilla y dolor en punta de vástago tibial. Resultados preliminares en un grupo de 20 pacientes. Rev Esp Cir Ortop Traumatol. 2014;58:206–211.
