


Osteoarthritis (OA) is a common degenerative disease associated with functional impairment, activity limitation, participation restriction, and poor quality of life. Therefore, comprehensive assessment is important to determine how complex problems affect patients with OA.
ObjectivesThe first aim of this study was to link and allocate items of The Western Ontario and McMaster Universities (WOMAC) OA index with the ICF Comprehensive Core Set for OA. The second aim was to examine the relationship between quality of life and each ICF component score based on WOMAC clinical data in OA.
MethodsHealth status was evaluated with WOMAC and quality of life with the Nottingham Health Profile (NHP). The WOMAC items were linked with codes of the ICF Comprehensive Core Set for OA and allocated with the ICF components by three researchers. The relationship between WOMAC scores and the NHP was determined by Pearson correlation analysis.
Results87 patients with OA were included. As distinguished by the researchers, 7 items of WOMAC covered body function and 17 covered activity-participation. Body function and activity-participation had a moderate correlation with the pain subtest of the NHP and low correlation with the energy level subtest and total score of the NHP. Activity-participation had a high correlation with the physical abilities subtest of the NHP.
ConclusionAlthough WOMAC does not cover environmental factors, it is a comprehensive tool to assess health status and quality of life. Our results showed that in OA physical abilities can lead to limitations in activity and participation, and these limitations are associated with the individual's pain, energy level, and quality of life.
Clinical trial registration number: NCT04956510.
La osteoartritis (OA) es una enfermedad degenerativa común asociada con deficiencias funcionales, limitaciones en la actividad, restricciones en la participación, así como una mala calidad de vida. Por tanto, la evaluación integral es importante para determinar cómo los problemas complejos afectan a los pacientes con OA.
ObjetivosEl primer objetivo de este estudio fue vincular y asignar elementos del índice OA de las universidades de Western Ontario y McMaster (WOMAC) con el conjunto básico completo de ICF para OA, mientras que el segundo objetivo fue examinar la relación entre la calidad de vida y las puntuaciones de cada componente de la ICF en función de los datos clínicos de WOMAC en OA.
MétodosSe evaluó el estado de salud con WOMAC y la calidad de vida con Nottingham Health Profile (NHP). Los ítems de WOMAC se vincularon con códigos de ICF Comprehensive Core Set for OA y 3 investigadores los asignaron con los componentes de ICF. La relación entre las puntuaciones WOMAC y NHP se determinó mediante el análisis de correlación de Pearson.
ResultadosSe incluyeron 87 pacientes con OA. Según la distinción de los investigadores, 7 ítems de WOMAC cubrieron la función corporal y 17 cubrieron la actividad-participación. La función corporal y la participación en la actividad tuvieron una correlación moderada con la subprueba de dolor de NHP y una correlación baja con la subprueba de nivel de energía y la puntuación total de NHP. La actividad-participación tuvo una alta correlación con la subprueba de habilidades físicas de NHP.
ConclusiónAunque WOMAC no cubre los factores ambientales, es una herramienta integral para evaluar el estado de salud y la calidad de vida. Nuestros resultados mostraron que en la OA, las habilidades físicas pueden conducir a limitaciones en la actividad y la participación, y estas limitaciones se asocian con el dolor, el nivel de energía y la calidad de vida del individuo.
Número de registro de ensayo clínico: NCT04956510
Osteoarthritis (OA) is the most common degenerative joint disease characterized by joint pain, tenderness, crepitation, stiffness and effusion in the clinic, leading to loss of functional status and quality of life.1,2 Individuals with OA can also be restricted in terms of activity in mobility and self-care, and in terms of participation in activity, social and occupational roles.3
Classification of Functioning, Disability and Health (ICF), which belongs to WHO's international classification family, is designed to provide a standard and framework for the description of health and health-related conditions. It includes more than 1400 codes in four components (activity and participation, body functions, body structure, environmental factors). Impairment of body structure and functions can be used to describe problems in physiological functions and anatomical parts of the body as a significant deviation or loss. Activity limitation and participation restrictions are described as difficulties in daily life activities and participation in social life situations. Environmental and personal factors can have positive or negative effects on the individual's performance in society, capacity to perform actions or tasks, or on body function or structure.4,5
Using such a comprehensive classification in clinics and research can cause difficulties. Therefore, ICF Core Sets, which is a smaller form of ICF, has been developed to make practical use easy. Comprehensive ICF Core Set is a list of ICF codes that consists of comphrehensive, multidisciplinary assessments for specific chronic condition including OA.5–7 Comprehensive ICF Core Set for OA consists of a total of 55 codes. Of these codes, 13 are body functions, 6 are body structure, 19 are activity and participation and 17 are environmental factors.7
Specific domains of health status criteria are systematically associated with the relevant parts of the ICF. This relation creates a common conceptual understanding in patient-reported outcome measures and facilitates clinical practice easy.8 The Western Ontario and McMaster Universities (WOMAC) OA index, which is recommended by the OMERACT (Outcome Measures in Rheumatology Clinical Trials) for assessment of hip and knee OA, is the most preferred form the patient-reported outcome measures used in clinical studies.9–11
Povlak and Valdes stated that the aim of ICF is to define health and lived health experience by focusing on a person's ability to interact with the environment and functions.12 They also recommended using of more outcome measures including quality of life or environmental factors in relation to ICF for future research on outcome measures related to OA.
The aim of this study was to link and allocate items of WOMAC with body function, activity-participation and environmental factors based on ICF Comprehensive Core Set for OA. The other aim of this study was to examine the relationship between the quality of life and body function, activity-participation and environmental factors scores determined based on clinical data of WOMAC in individuals with OA.
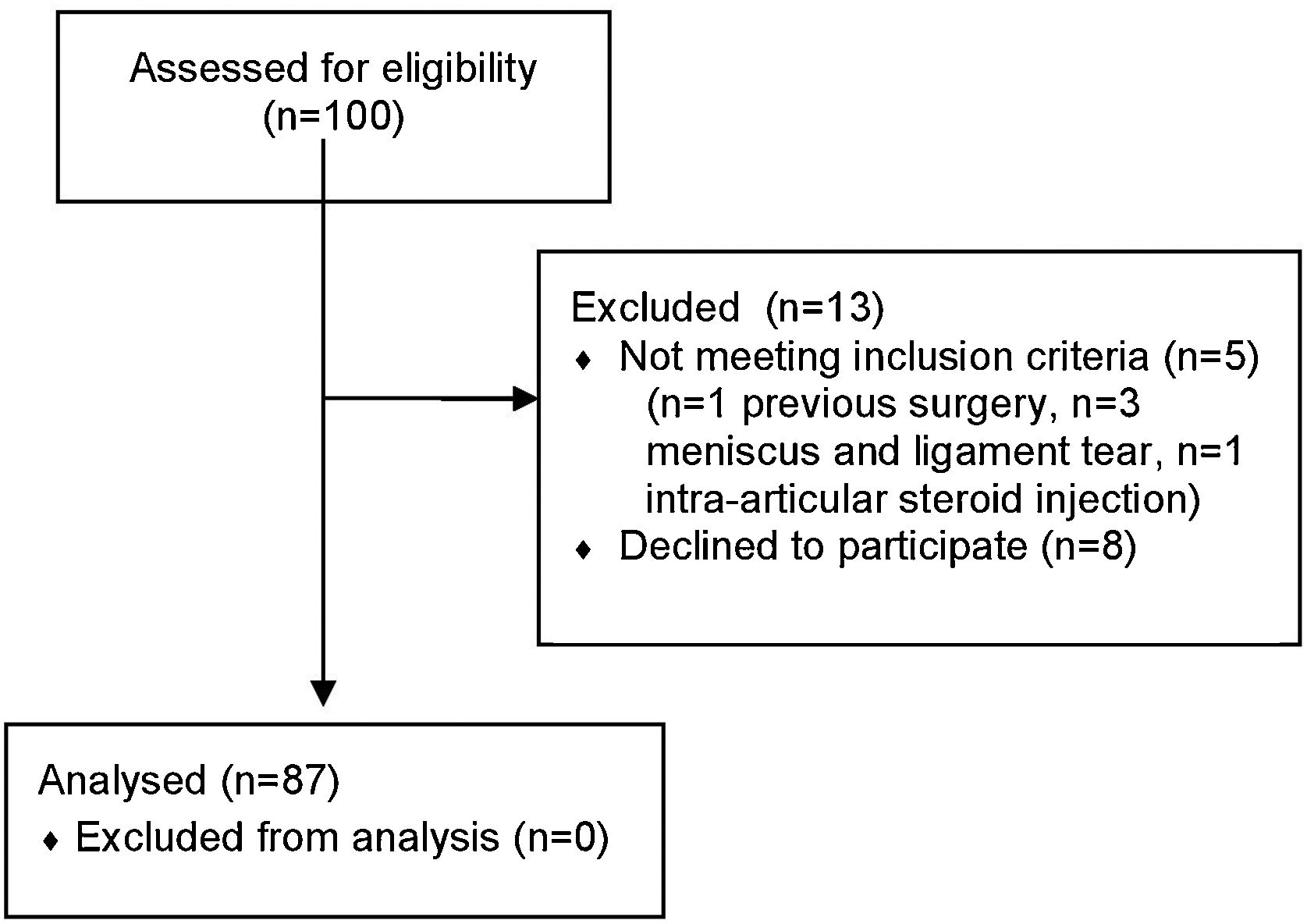
MethodsParticipantsPatients with OA were included, who met inclusion criteria and were diagnosed with OA by the same rheumatologist according to the American College of Rheumatology (ACR) Clinical Classification Criteria for OA. The individuals participating in the evaluation were diagnosed at Pamukkale University Medical Faculty Hospital (Denizli, Turkey) and their evaluations were made by the same physiotherapist working in the Rheumatological Physiotherapy and Rehabilitation unit of the same university. Figure 1 shows a flow chart of the study design. Inclusion criteria were: (a) diagnosed with OA according to ACR clinical criteria for OA of the knee or hip;13,14 (b) being in the age range 18–65; and (c) absence of other diseases affecting functions and daily life (orthopedic, neurological, cardiovascular, metabolic disease and lung pathology). Exclusion criteria were: (a) comorbidity affecting lower extremity and functions (patellofemoral pain syndrome, rheumatoid arthritis, ligament tear, meniscus); (b) previous lower extremity surgery; (c) Intra-articular steroid or hyaluronic acid injection in the last three months (d) cognitive impairments; (e) pregnancy; and (f) illiteracy.

All the participants provided a verbal and written informed consent at the first interview. The study was performed in compliance with the Declaration of Helsinki. Ethical approval was obtained from Local Ethics Committee for Noninvasive Clinical Research.
MeasuresOA diagnosed individuals were called separately for assessment by giving an appointment on different days. All the evaluations for each individual were completed on the their appointment day and by the same researcher, who works at Pamukkale University, Rheumatological Physiotherapy and Rehabilitation Unit, in approximately 40minutes by face-to-face interview method.
Demographic characteristics of participants with OA were recorded. Then, health status with WOMAC OA Index and quality of life with NHP were evaluated. Individuals with OA were asked to fill in the questionnaires used in the assessment themselves. However, the physiotherapist was with the individual while filling out the questionnaires and made the necessary explanations for the question individuals with OA did not understand.
The Western Ontario and McMaster Universities (WOMAC) OA Index: The WOMAC Index is a self-administered, disease-specific questionnaire consisting of 24 items which are widely used in the evaluation of hip and knee OA. It consists of 24 items: pain (5 items), stiffness (2 items), and physical function (17 items). High score indicates worse pain, stiffness, and functional limitations.15,16
Nottingham Health Profile (NHP): NHP is a widely used measure of perceived distress of patients in physical, emotional and social domains. It consists of 38 items which are physical mobility (8 items), pain (8 items), sleep (5 items), emotional reactions (9 items), social isolation (5 items) and energy level (3 items). Questions have “yes” or “no” answers. Higher score indicates greater distress.17 In our study, we used the NHP to evaluate the quality of life in individuals with OA. The NHP, particularly has been found reliable in individuals with OA to the assessment of perceived health status.18
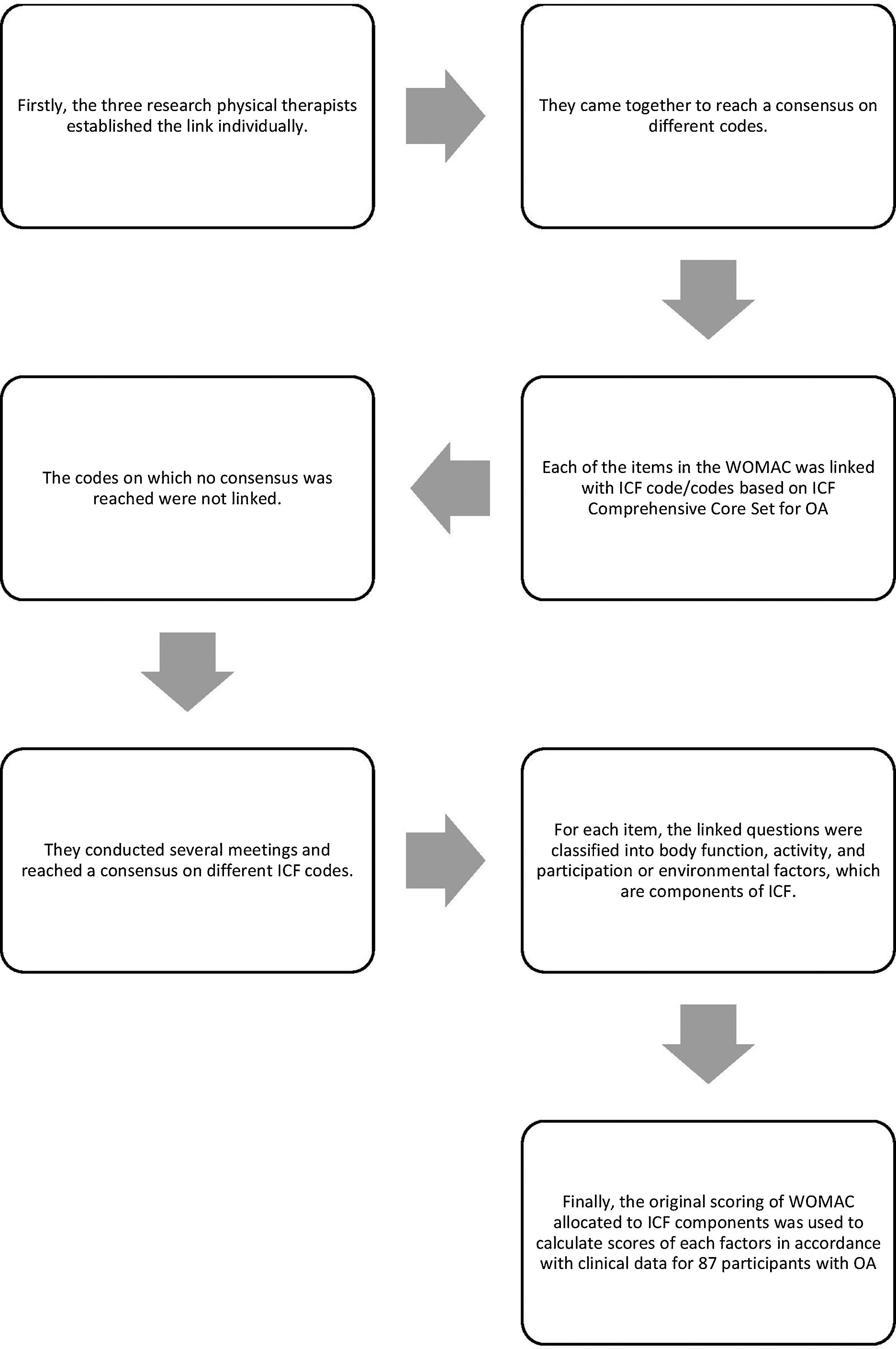
Linking ICF codes with WOMAC score itemsICF coding system is divided into two parts. The first part deals with the process of functioning and disability; b (body functions), s (body structures) d (activities and participation). The second part deals with environmental and personal factors; e (environmental factors). The items of WOMAC were linked with ICF codes based on ICF Comprehensive Core Set for OA by three experienced research physical therapists. The linking steps were based on the linking rules of Cieza et al.19 In the first step of linking, the research physical therapists individually established the link. In the second step, three investigators came together to reach a consensus on different codes. Each of the items in the WOMAC was linked with ICF code/codes based on ICF Comprehensive Core Set for OA, and the codes on which no consensus was reached were not linked. Then, three investigators conducted several meetings and reached a consensus on different ICF codes. For each item, the linked questions were classified into body function, activity, and participation or environmental factors, which are components of ICF. Finally, the original scoring of WOMAC allocated to ICF components was used to calculate scores of body function, activity/participation, and environmental factors in accordance with clinical data for 87 participants with OA. The linking steps were shown in Figure 2.
Statistical analysis
Statistical analysis was made using SPSS packet program (Version 21.0). Continuous variables with normal distribution were reported using mean and standard deviation, and non- normal distribution variables with median, minimum and maximum values. Normal distribution was assessed using the Kolmogorov-Smirnov test. The categorical variables were expressed in numbers and percentages. Bivariate analysis using Pearson's Correlation coefficients was calculated using the WOMAC with NHP scores. Correlation was categorized as low (r 0.10-0.49), moderate (r 0.50-0.69), or high (r 0.70-1.00).20 P value <0.05 was considered as statistically significant.
ResultsAt first 100 patients with OA were evaluated. 5 participants who did not meet the inclusion criteria and 8 who declined to participate were excluded from the study. Finally, eighty-seven patients with OA were included in the study. The median age of the patients who met the inclusion criteria was 61 (31-80) years, of whom 81 (93.1%) were women and 6 (6.9%) were men. 31.25 (17.8-54.78) kg/m2 was the median BMI value of patients. The majority of the affected body side of patients was bilateral (66.7%) and the body part was knee (66.7%) Demographic characteristics of the patients are shown in Table 1.
Demographic characteristics of the patients.
| Median (min-max) | |
|---|---|
| Age (years) | 61 (31-80) |
| Body weight (kg) | 76 (45-120) |
| Height (m) | 1.57 (1.42-1.80) |
| BMI (kg/m2) | 31.25 (17.8-54.78) |
| Disease duration (years) | 2 (0.08-25) |
| n (%) | |
| Gender | |
| Female | 81 (93.1) |
| Male | 6 (6.9) |
| Affected body side | |
| Right | 19 (21.8) |
| Left | 10 (11.5) |
| Bilateral | 58 (66.7) |
| Affected body part | |
| Hip | 13 (14.9) |
| Knee | 58 (66.7) |
Based on expert distinction, the 7 items of WOMAC covered body function (BF) component and the 17 items of WOMAC covered activity-participation (AP) component in ICF Comprehensive Core Set for OA. According to the results of linking and allocating, the median scores of WOMAC BF and WOMAC AP were 14 (range from 2 to 14) and 32 (range from 0 to 136), respectively (Table 2).
Results and scores of linking and allocating items of WOMAC OA Index with components of ICF Comprehensive Core Set for OA and scores.
| Items | ICF Code | ICF Component | WOMAC BFMedian (min-max) | WOMAC APMedian (min-max) |
|---|---|---|---|---|
| 1. Pain walking on a flat surface | b28016b7603 | BF | 14 (2-61) | |
| 2. Pain going up or down stairs | BF | |||
| 3. Pain at night while in bed | BF | |||
| 4. Pain sitting or lying | BF | |||
| 5. Pain standing upright | BF | |||
| 6. Stiffness after first wakening in the morning | b7800 | BF | ||
| 7. Stiffness after sitting, lying or resting later in the day | b7808 | BF | ||
| 8. Descending stairs | d4551 | A | 32 (0-136) | |
| 9. Ascending stairs | d4551 | A | ||
| 10. Rising from sitting | d4103 | A | ||
| 11. Standing | d4154 | A | ||
| 12. Bending to floor | d4105 | A | ||
| 13. Walking on flat surface | d4500 | A | ||
| 14. Getting in/out of car | d410 | A | ||
| 15. Going shopping | d620 | P | ||
| 16. Putting on socks/stockings | d5402 | A | ||
| 17. Rising from bed | d4103 | A | ||
| 18. Taking off socks/stockings | d5403 | A | ||
| 19. Lying in bed | d4150 | A | ||
| 20. Getting in/out of bath | d410 | A | ||
| 21. Sitting | d4153 | A | ||
| 22. Getting on/off toilet | d530 | A | ||
| 23. Heavy domestic duties | d6409 | A | ||
| 24. Light domestic duties | d6409 | A |
BF: Body Function, A: Activities, P: Participation, EF: Environmental factors; WOMAC: The Western Ontario and McMaster Universities Arthritis Index; ICF: International Classification of Functioning, Disability and Health.
The median WOMAC total score was 47 and NHP total score was 312. The median scores of NHP subtests were energy level (100), pain (80.26), emotional reactions (41.44), social isolation (20.13), sleep (43.36) and physical abilities (41.86). Detailed descriptive statistics of WOMAC, NHP total and subtests in patients are shown in Table 3.
Descriptive statistics of WOMAC and NHP.
| Median (min-max) | |
|---|---|
| WOMAC Total | 47 (4-152) |
| NHP Total | 312 (20.46-566.01) |
| Energy Level | 100 (0-100) |
| Pain | 80.26 (8.96-100) |
| Emotional Reactions | 41.44 (0-100) |
| Social Isolation | 20.13 (0-100) |
| Sleep | 43.36 (0-100) |
| Physical Abilities | 41.86 (0-428.43) |
WOMAC: The Western Ontario and McMaster Universities Arthritis Index; NHP: Nottingham Health Profile.
In the Pearson correlation analysis among body function and activity-participation of WOMAC with total and subtests of NHP, body function had a moderate correlation with activity-participation (r=0.500; p=0.001). Furthermore, body function had a moderate correlation with pain subtest of NHP and had low correlation with energy level subtest and total of NHP (r=0.562, p=0.001; r=0.327, p=0.006; r=0.365, p=0.002; respectively). Activity-participation had high correlation with physical abilities subtest of NHP, moderate correlation with pain subtest of NHP and low correlation with energy level subtest and total of NHP (r=0.764, p=0.001; r=0.566, p=0.001; r=0.346, p=0.004; r=0.472, p=0.001; respectively) (Table 4).
Correlation between study variables.
| WOMAC BF | WOMAC AP | |||
|---|---|---|---|---|
| r | p | r | p | |
| WOMAC BF | 0.500 | 0.001 | ||
| NHP Total | 0.365 | 0.002 | 0.472 | 0.001 |
| Energy Level | 0.327 | 0.006 | 0.346 | 0.004 |
| Pain | 0.562 | 0.001 | 0.566 | 0.001 |
| Emotional Reactions | 0.168 | 0.163 | 0.195 | 0.110 |
| Social Isolation | 0.184 | 0.127 | 0.157 | 0.200 |
| Sleep | 0.115 | 0.345 | 0.200 | 0.103 |
| Physical Abilities | 0.202 | 0.094 | 0.764 | 0.001 |
Pearson correlation analysis. BF: Body function; AP: Activity-participation; NHP: Nottingham Health Profile.
The study aimed to link and allocate the items of WOMAC with body functions, activity/participation and environmental factors based on ICF Comprehensive Core Set for OA and to examine the relationship between quality of life and ICF component scores determined based on clinical data of WOMAC in individuals with OA. Our results showed that seven items of WOMAC covered body function, seventeen items covered activity-participation category of ICF. There were no items that covered the environmental factors.
OA causes global disability and leads to limitations in daily activities and restrictions on participation. The quality of life is also decreased due to this restriction in participation and impairment of body function in individuals with OA.21,22 The most reliable evaluation of functional capacity can be obtained with objective measurements and as a result of evaluating the patient's self-perceived function with various methods.23 It is argued that using valid and reliable measures in evaluating the effect of the problems on functionality and quality of life is necessary to evaluate the effectiveness of the treatment, to monitor the progression of the disease and to make clinical decisions.24-26 Also linking of ICF, which is described as the general health-status framework, with these disease-specific outcome measures may help create a common language for clinical practice and research.27 Based on the ICF assessment, a functional profile can be created and then used as a reference for patient follow-up and determining intervention targets for treatment.19 It can be contributed both individually and socially by controlling the effects of the disease during the progression in consequence of a good analysis.
One-way assessments may not reflect the complex nature of interventions for multiple problems.28 Handling the relevant structures insufficiently and using the inappropriate measurements may create a deficiency in the evaluation of intervention and outcomes.19 ICF helps to overcome the difficulties encountered in defining the complex relationship among disease, treatment and evaluation results.8 ICF focuses on the individual and their functions in society as a whole, rather than a single part of the body.
Weigl and Wild linked 28 different ICF categories with items of WOMAC in their study including patients with knee and hip OA for European population from different regions.21 In this study, while the researchers stated that interregional distribution was insufficient and the results were affected by cultural and ethnic differences, our study was performed in a single center and only in individuals with knee OA, representing more homogeneous results. Weigl et al. stated that 5 items were linked with body function, 19 were linked with activity and participation, and there were no items linked with environmental factors, also 3 of 24 items were linked with both body function and activity/participation. As a result, they stated that using disease-specific outcome measures, which determine changes in the short term, with ICF together may become useful in clinical studies. In our study, WOMAC was linked with 7 of body function, 16 of activities and 1 of participation categories. We also concluded that WOMAC was related to none of the environmental factors. According to this result, we consider that WOMAC might be an adequate outcome measure that could evaluate functional disability in OA patients because of evaluating body function and activity problems related to disability comprehensively. However, we consider that it does not adequately assess participation restrictions and provide any data about environmental factors. In this respect, we recommend that the WOMAC would be re-examined in terms of these parameters. Considering this contextual component (environmental factors) of the functionality is significant because this information is important in the evaluation process.
In our study, we also used the original scoring of WOMAC whose items were linked with ICF Comprehensive Core Set for OA and allocated to ICF components to calculate the scores of body function, activity/participation in accordance with clinical data. However, the methodological perspectives of the two studies in this field differ from our study. The validity and reliability of the ICF comprehensive core set for OA was performed in these two studies by Kurtais et al. and Weigl and Wild.
Kurtais et al. examined the relationship between body function, body structure, activities, participation and environmental factor scores which were obtained using the comprehensive core set for OA with WOMAC and SF-36.29 They showed body function, body structure, activities and participation components had a moderate correlation with WOMAC and SF-36. Also, they showed that environmental factors score had no relation with the total scores of WOMAC and had a weak correlation with SF-36.
Weigl and Wild examined the correlation between ICF comprehensive core set for OA categories and the physical and mental component of the SF-36. They reported that body functions and activity-participation categories showed significant correlation with physical component of SF-36.21
The original scoring of WOMAC allocated to ICF components was used to calculate scores of body function, activity/participation, and environmental factors in accordance with clinical data of participants with OA in our study. We found that the body function score of WOMAC was moderately correlated with activity-participation score of WOMAC. It was observed that OA patients felt more limitation in daily life activities as the level of structural disorders increased and this situation restricted the participation in life. Since WOMAC did not cover any environmental factors, its relation with environmental factors could not be determined.
NHP was used to evaluate the quality of life of participants with OA. According to our results, body function and activity-participation were moderately correlated with the pain subtest of NHP and were poorly correlated with the energy level subtest and the total of NHP. Furthermore, activity-participation was highly correlated with the physical abilities subtest of NHP. It was concluded that in OA patients, physical mobility ability was one of the most important indicators of how active one was in daily life and how much was involved in life. The pain was seen as another important indicator of activity and participation. The individuals having pain avoid activities and withdraw from social life. We think that inactivity and social isolation may cause people to energy levels to decrease. It is known that decreasing the quality of life in a person who has this clinical picture will be inevitable.
The limitations of this study are that investigators that established the link were from the same discipline. This study was planned and carried out in cooperation with a rheumatologist and physiotherapist. If there were researchers from different disciplines such as occupational therapist, social worker, it could be linked with a multidimensional perspective. The other limitation is that due to using questionnaires as a measurement tools, it takes a long time to ensure participants’ understanding and remains subjective compared to a functional measurement tools according to ICF assessment.
Our findings can be used as a guideline for health professionals and researchers to use patient-reported outcome measures in assessing patients with their bio-psycho-sociological aspects. With these studies, arrangements can be made in existing outcome measures by determining the limitations of scales. Furthermore, more qualified scales, which evaluate the patients more comprehensively, can be developed by considering these limitations. Thus, it enables to use of a more qualified single scale instead of several scales and saves time for clinicians and researchers’ needs.
ConclusionThe results of this study demonstrate that the WOMAC, which is the most common measure correlated with OA, covers mostly activity components, then body function components, but least participation components and no environmental factors of ICF categories. Activity limitations and participation restrictions are highly correlated with physical skill; body function disabilities, activity limitations and participation restrictions are correlated with pain, energy level and quality of life. As a result of this study, it was seen that improving the quality of life in pain and energy level sub-parameters is important in increasing body function and activity/participation in individuals with OA. For this reason, we recommend that these individuals be evaluated with a biopsychosocial aspect in the clinic.
FundingThis study did not receive any specific grant from funding agencies.
Conflict of interestAuthor's declare that they have no conflict of interest.
Data availabilityData can be supplied on request to the authors.
Ethical considerationsThe study was performed in compliance with the Declaration of Helsinki. Ethical approval was obtained from Local Ethics Committee for Noninvasive Clinical Research of Pamukkale University.
