



This study aimed to investigate the association between occupation and depressive/anxiety symptoms, and education levels, among professionals from a Brazilian General Hospital in need of mental health treatment.
Design and settingThis is a cross-sectional study, involving professionals from a teaching hospital in São Paulo.
MethodsSocio-demographic data were collected as well as two standardized scales for depression and anxiety symptoms.
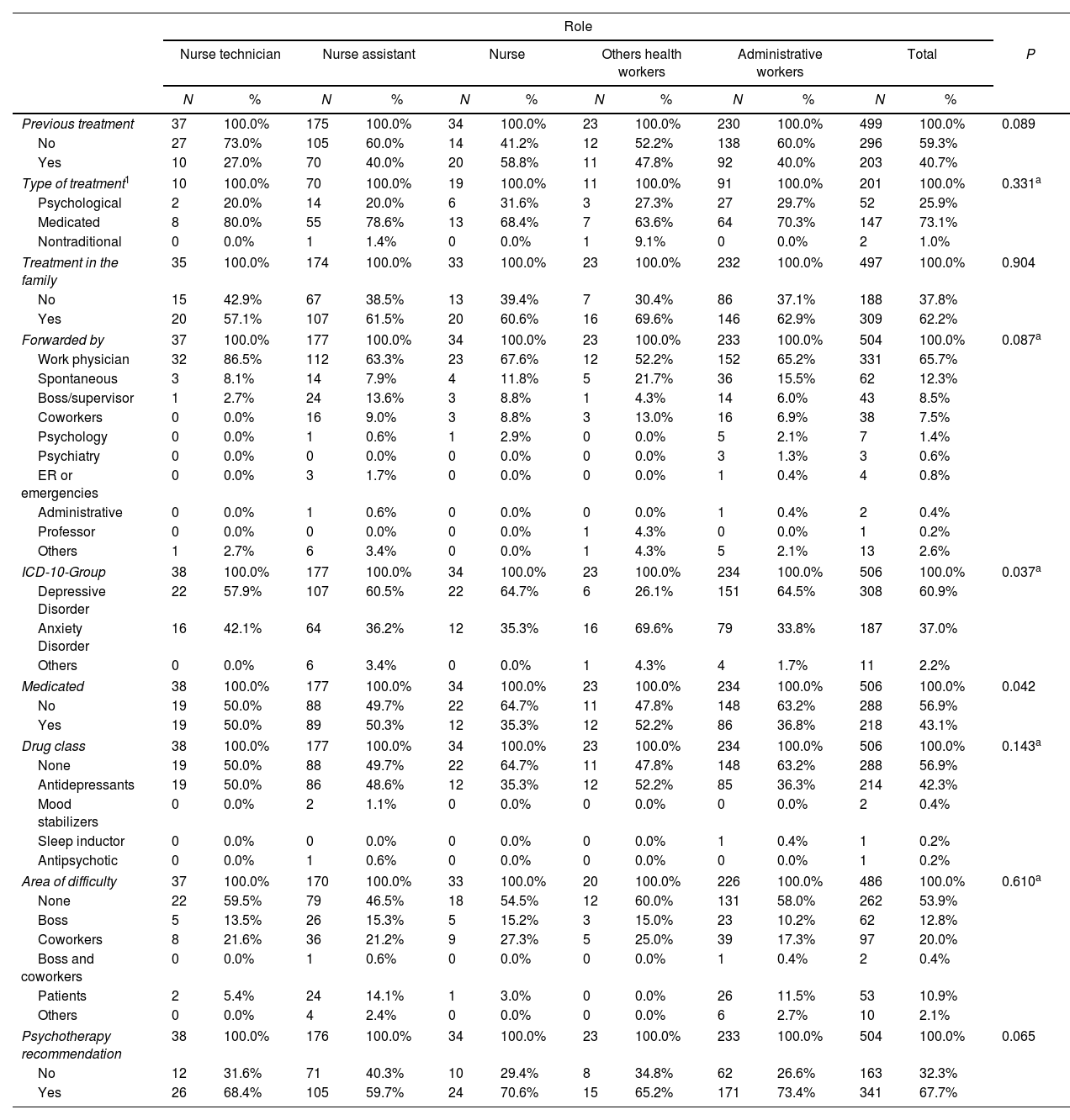
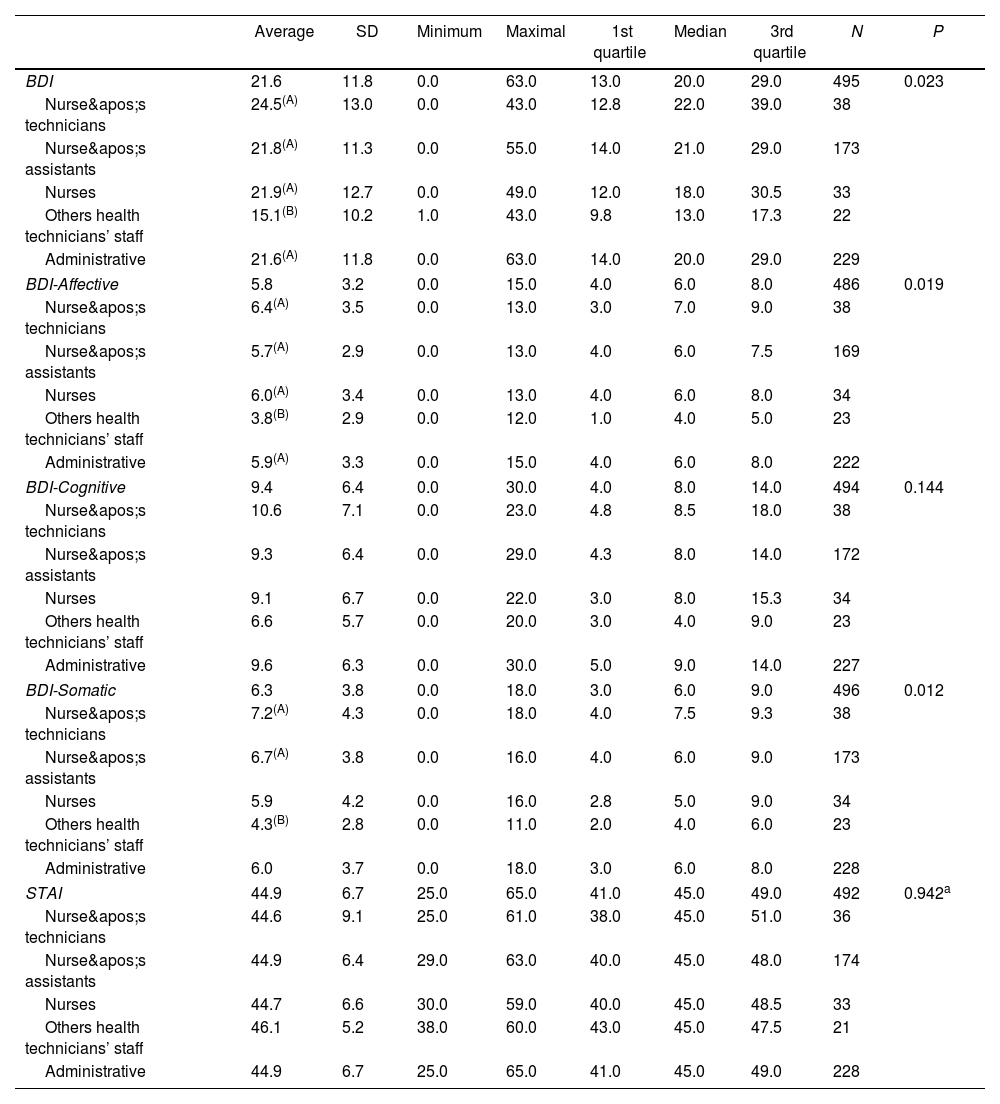
ResultsData from 506 employees seeking mental health assistance have been described: mean age was 34.6 years, 46.2% of them worked in the administrative sector, 35.0% were nursing assistants, 7.5% were nursing technicians, 6.7% were nurses, and 4.5% reported other occupations. According to the International Classification of Diseases-10th edition (ICD-10) criteria, the rates of diagnosis of depressive disorders and anxiety disorders were 60.9% and 37%, respectively. Nursing technicians and nursing assistants reported higher somatic cluster Beck Depression Inventory (BDI) scores (P=0.012) than other professionals of technical staff, but they were less inclined to receive a psychiatric diagnosis.
ConclusionsOur study demonstrated prevalence rates higher than similar studies in university hospitals, fact that associated with difficulties of the studied population as seeing themselves as sick, and the social discrimination suffered by people with mental disorders can make this problem even worse.
Este estudio tuvo como objetivo investigar la asociación entre la ocupación y los síntomas depresivos/ansiosos, los niveles de educación, entre los profesionales de un hospital general brasileño en necesidad de tratamiento de salud mental.
Diseño y escenarioEste es un estudio transversal, involucrando profesionales de un hospital escuela en São Paulo.
MétodosSe recogieron datos sociodemográficos y dos escalas estandarizadas para síntomas de depresión y ansiedad.
ResultadosSe describen datos de 506 empleados que buscaban asistencia en salud mental: la edad media fue de 34,6 años, el 46,2% trabajaba en el sector administrativo, el 35,0% eran auxiliares de enfermería, el 7,5% eran técnicos de enfermería, el 6,7% eran enfermeros y el 4,5% reportaron otras ocupaciones. Según los criterios de la Clasificación Internacional de Enfermedades, 10.ª edición (CIE-10), las tasas de diagnóstico de los trastornos depresivos y los trastornos de ansiedad fueron del 60,9% y del 37%, respectivamente. Los técnicos y auxiliares de enfermería relataron puntajes más altos (P=0,012) del Inventario de Depresión de Beck del clúster somático que otros profesionales del cuerpo técnico, pero se mostraron menos inclinados a recibir un diagnóstico psiquiátrico.
ConclusionesNuestro estudio demostró tasas de prevalencia superiores a estudios similares en hospitales universitarios, hecho que asociado a las dificultades de la población estudiada para verse a sí mismos como enfermos, y la discriminación social que sufren las personas con trastornos mentales puede agravar aún más este problema.

