



Most of the studies that have examined cognitive and executive functions in conduct disorders (CD) have been conducted on institutionalized male adolescents. In this research the cognitive and executive functions of non-institutionalized Colombian school children with CD were compared with normal school children, all between 6 and 12 years-old.
Materials and methods: We used a case-control design. The cases were participants who met the diagnostic criteria for CD (n=39) and controls who did not meet these criteria (n=39), according to reports of a professional of the participants’ institution, and a structured interview for childhood psychiatric syndromes. The two groups were selected from educational institutions, and there were no differences in age, school grade, or socioeconomic level. The IQ was reviewed, as well as the presence of other mental disorders, serious physical illnesses, and more serious neurological signs. The cognitive and executive functions were evaluated using a child neuropsychological test battery.
ResultsWe found that participants with CD had significantly lower scores in construction abilities, perceptual abilities (tactile, visual and auditory), differed in verbal memory, differed in visual memory, language (repetition, expression and understanding), meta-linguistic abilities, spatial abilities, visual and auditory attention, conceptual abilities, verbal and graphic fluency, and cognitive flexibility. The same differences were found between males, except in repetition, whereas girls showed fewer differences, thus the cognitive and executive performance was poorer in males with CD than in females, especially in verbal and linguistic-related functions.
ConclusionsChildren with CD could show generalized cognitive and executive deficits. These deficits seem to be more frequent in boys than in girls with CD.
La mayoría de los estudios que han examinado las funciones cognitivas y ejecutivas en el trastorno disocial (TD) se han llevado a cabo con adolescentes varones institucionalizados. En esta investigación, se compararon las funciones cognitivas y ejecutivas de escolares colombianos no institucionalizados con TD con las de escolares normales, todos entre 6 y 12 años de edad.
Materiales y métodosSe utilizó un diseño de casos y controles, en el que los casos eran los participantes que cumplían los criterios diagnósticos de TD (n=39) y los controles, aquellos que no cumplían estos criterios (n=39), de acuerdo con el reporte de un profesional de la institución de los participantes y una entrevista estructurada de síndromes psiquiátricos infantiles. Los dos grupos fueron seleccionados de instituciones educativas y no diferían en edad, grado escolar y nivel socioeconómico. El CI fue controlado, así como la presencia de otros trastornos mentales, enfermedades físicas graves y signos neurológicos mayores. Las funciones cognitivas y ejecutivas fueron evaluadas a través de una batería neuropsicológica infantil.
ResultadosLos participantes con TD presentaron puntuaciones significativamente más bajas en habilidades construccionales, habilidades perceptuales (táctiles, visuales y auditivas), memoria verbal diferida, memoria visual diferida, lenguaje (repetición, expresión y comprensión), habilidades metalingüísticas, habilidades espaciales, atención visual y auditiva, habilidades conceptuales, fluidez verbal y gráfica y flexibilidad cognitiva. Estas mismas diferencias se encontraron entre los varones entre sí, excepto en repetición, mientras que las niñas presentaron menos diferencias entre sí, de manera que el desem peño cognitivo y ejecutivo fue más bajo entre los varones que entre las niñas con TD, especialmente en funciones verbales y relacionadas con el lenguaje en general.
ConclusionesLos niños con TD podrían presentar déficits cognitivos y ejecutivos generalizados, que parecen ser mayores entre los niños que entre las niñas con dicho trastorno.
Conduct disorder (CD) is defined as a pattern of behavior that is characterized by persistent enforcement actions affecting social norms and the rights of others, including attacks on humans and animals, destruction of property, dishonesty or theft and serious violations of rules1,2. CD usually appears towards the end of childhood or early adolescence and is divided into childhood-onset subtype if at least one of the antisocial behaviors listed in the diagnosis is made within ten years of age and adolescent onset subtype if such conduct occurred only after they were ten years old1. According to Althoff et al3, prevalence of this disorder rates as high as 16% of the samples, though rates tend to be consistent between different cultures. In Colombia, the National Survey of Mental Health4 found that lifetime prevalence of this disorder amounted to 8.8% of males and 2.7% of women, among 4544 sampled between 18 to 65 years of age, while Pineda et al5 reported a prevalence of 8.4%, among 190 male adolescents, between 12 and 18 from a lower, middle and high socioeconomic strata, at randomly selected educational institutions in Medellin, where scores indicate that this disorder may affect a significant percentage of children and adolescents in Colombia.
CD is ostensibly more frequent among men than among women6–8 and tends to have a high comorbidity with learning disorders, substance use disorders and attention-deficit/ hyperactivity disorder [ADHD]1,9,7, being a comorbid condition with the latter that affects 50% of cases3. CD is associated, too, with poor relationships with peers and adults, academic failure, low emotional reactivity, medical complications during pregnancy and childbirth, difficult temperament in early childhood, low empathy, low tolerance for frustration, impulsivity, irritability, recklessness, sensation seeking, disinhibition, extraversion and low moral development1,6,9–12. Other features that have been associated with CD include parental psychopathology, parent's criminal history, child abuse, inadequate parenting practices, constant marital conflict and belonging to a large family7,9,13.
One of the aspects that has been examined in individuals with CD are the cognitive and executive functions evaluated by neuropsychological tests. According Eme14, researchers have concluded unanimously that there is some type of neuropsychological damage involved in the etiology of CD, which causes deficits in executive and cognitive functioning, deficits in the verbal area being the most consistently reported, but also deficits in spatial and memory functions have been reported. Olvera et al15, for example, found lower scores on cognitive, inhibitory and behavioral change, planning, language and verbal memory performance among 26 juvenile offenders with CD, compared with 16 controls with similar demographic characteristics. Pineda et al16, mean-while, found a verbal IQ, which is general and manipulative, and a degree of language comprehension, verbal fluency and schooling significantly lower in a sample of adolescent male offenders with CD, compared to a control group and exhibited greater conflictual relationships with peers, attention deficits, medical complications during pregnancy, use of psychoactive substances and time required for the resolution of the Complex Figure Test and Trail Making Test. Pajer et al17 also found lower scores on intelligence and poor performance on executive functions and visual-spatial area and a lower academic achievement among 93 adolescent girls with ADHD compared with 41 normal adolescents, while Trujillo et al18 reported a reduced capacity for immediate recall of verbal information with a delay in color naming, memory deficits and slower verbal-visual processing among 117 adolescent offenders with severe CD, compared with 111 controls.
Since the seminal review by Moffitt19,20, it has been considered that these deficits are more characteristic neuropsychological symptoms of childhood-onset subtype of CD, which, compared with adolescent-onset subtype tends to be more persistent over time and it is related to antisocial aggression and more severe symptoms of hyperactivity, comorbidity with ADHD and a higher probability of engaging in criminal activity in adolescence and adulthood and the development of antisocial personality disorder7,9,14,21–23. It is considered that this subtype of CD has a strong biological influence and tends to be more persistent and severe due to this circumstance10,14.
While there is no global agreement regarding the nature and number of processes that are executive functions, there is consensus that such processes facilitate self-regulation necessary to achieve goals successfully, so that a malfunction increases this probability of inadequate emotional, behavioral and cognitive regulation, increasing the risk of CD14,24. Deficits in executive functions, therefore, could explain the charac teristics of individuals with CD, such as impulsivity, reckless conduct, breaking rules, aggression, disinhibition, extraversion, poor moral development and sensation seeking1,7,25 as well as its high comorbidity with attention deficit disorder with hyperactivity, due to difficulties with impulsivity that characterize the latter disorder23. Therefore, the study of cognitive and executive functions among school-age children could provide more insight into the etiology of CD. However, most studies that have examined these functions have been conducted with institutionalized adolescents diagnosed with CD, so it is not possible to confirm whether such deficits are present from childhood, and among non-institutionalized boys and girls with CD.
Based on the above, the purpose of this research was to evaluate cognitive and executive functions of a sample of school-age children with CD who are not institutionalized, compared, at a general level and by sex, to a sample of children without the disorder with similar demographic charac teristics. We used the Child Neuropsychological Assess ment Battery (Evaluación Neuropsicológica Infantil [ENI]26), through which the following cognitive functions were assessed: constructional skills, perceptual skills (tactile, visual and auditory) verbal memory (encoding), visual memory (encoding), delayed verbal memory, delayed visual memory, language (repetition, expression and understanding), metalinguistic skills, spatial skills, visual and auditory attention and conceptual skills, and the following executive functions: verbal fluency, graphic fluency, cognitive flexibility and planning and organization.
Materials and methodsParticipantsIt included a sample of 49 boys (62.8%) and 29 girls (37.2%), for a total of 78 participants, ranging in age from 6 to 12 (mean, 9.4±2.04) years, of which 39 met the diagnostic criteria for CD, according to Children's Interview for Psychiatric Syndromes-Spanish version (ChiPS27), while the remaining 39 did not have the disorder under the same criteria. Participants were selected from three educational institutions in Bogotá with students that differed in the socioeconomic status, making way for a sample of 30 participants from low-low socioeconomic status (38.5%), 30 low socioeconomic status and low-middle (38.5%) and 18 middle and middle high (23%). No participants had a score indicating possible intellectual deficits (e.g., a composite IQ below 70), according to the Kaufman's Brief Intelligence Test (K-BIT28), or other mental disorders, serious physical illness or major neuro-logical symptoms, according to information provided by their parents in ENI's clinical history questionnaire26.
Participants with CD (30 boys and 9 girls) had a mean age of 9.54±1.99 years and were selected according to their availability in the three educational institutions, prior identification of the professional of each institution, while participants without CD (19 boys and 20 girls) had a mean age of 9.26±2.11 years, with students from 6–12 years of age selected from these institutions who did not exhibit behavioral problems. The two subsamples did not differ in age (F[1, 78]=0.369; P=.545), grade (F[1, 78]=0.451; P=.504) or socioeconomic status (U[n=78]=760.5; P=1).
InstrumentsChildren's Interview for Psychiatric Syndromes-Spanish version (ChiPS27). It is a highly structured interview, based strictly on the diagnostic criteria of the Fourth Edition of the Diagnostic and Statistical Manual of Mental Disorders29. It is given to people between 6 and 18 years of age, allowing the diagnosis of 20 psychiatric disorders. In this study we used only the CD scale, composed of 15 reagents. The instrument showed a sensitivity of 87% and a specificity of 76%27.
Kaufman's Brief Intelligence Test-Spanish version (K-BIT28). It is a test of “screening”, which measures verbal and nonverbal intelligence in individuals from 4 to 90 years of age, by means of two subtests: Vocabulary (verbal intelligence) and Matrices (nonverbal intelligence). The Vocabulary subtest assesses the development of language and verbal conceptualization level, while the matrices subtest measures nonverbal skills and the ability to solve problems. The application of this test is individual character with dichotomous items (0–1) and it requires 15 to 30 minutes to complete. To obtain the composite IQ scores are added in each subtest. The reliability coefficient reported by authors was .98 for the Vocabulary subtest, .97 for the Matrices subtest and .98 for IQ Composite and the test-retest analysis showed correlations ranging from .86 and. 95, presenting statistically significant correlations with similar tests28.
Child Neuropsychological Assessment (Evaluación Neuro-psico lógica Infantil [ENI]26). It allows for the evaluation of the following cognitive functions of schoolchildren aged 5 to 16 years: constructional skills, verbal and visual memory (encoding and delayed recall), perceptual skills, language, metalinguistic skills, spatial skills, attention (visual and auditory) and conceptual skills and the following executive functions: verbal fluency, graphic fluency, cognitive flexibility and planning and organization. It also presents a medical history questionnaire to be filled out by the parents and two annexes to assess handedness and the presence of soft neurological signs. The normative values by sex and age were obtained with a sample of 788 children aged 5 to 16 years of age, 540 Mexican children and 248 Colombians. The inter-rater reliability ranged between .86 and .99 and concurrent validity was assessed with the Wechsler Intelligence Scale for Children-Revised (WISC-R30) which found significant correlations between scales of ENI and its corresponding WISC-R.
Constructional skills are measured from the subdomains: construction with sticks and graphic skills, for which tests are used with chopsticks construction, a human figure, a copy of figures and a copy of the complex figure. The memory consists of two subdomains: encoding and delayed recall. Word lists are used to evaluate the coding tests, recall of a story and list of figures, while the delayed recall tests are used to recover the complex figure evocation of auditory and visual stimuli: spontaneous recovery of the list words, recovery of key auditory verbal recognition, a written story recovery, recovery of the complex figure, spontaneous recovery of the list of figures, and key recovery for visual recognition26,31.
Perceptual abilities are comprised of the subdomains of tactile perception, visual perception and auditory perception. The tactile sense is assessed through testing the right hand and left hand while visual perception is measured by testing overlapping images, blur, close visual proximity, speech recognition and integration of objects. Finally, auditory perception is evaluated by tests of musical notes, environmental sounds and phonemic awareness26,31.
The language domain consists of subdomains: repetition, expression and understanding. The tests designed to measure repetition are: repetition of syllables, words, words and sentences, while for the evaluation of expression: a picture naming test, narrative coherence and the length of the expression are used. The subdomain of understanding is assessed by designating imaging tests, following instructions and understanding of speech. Metalinguistic skills are measured through testing synthetic phonics, counting sounds, spelling and word count. The domain of spatial skills, in turn, is measured by comprehension tests: right-left, left-right expression, drawings of different angles, orientation of lines and location coordinates, while the domain of attention, composed by the visual and auditory subdomains, is evaluated by testing patterns of cancellation, cancellation of letters, digit retention in progression and regression. The domain of conceptual skills is assessed through tests of similarities, matrices and arithmetic problems26,31.
The executive functions, in turn, are composed of domains26,31:
- •
Verbal fluency, which consists of two tests of semantic fluency (fruits and animals) and a phonemic fluency test.
- •
Graphic fluency, consisting of semantic and non-semantic fluency tests.
- •
Cognitive flexibility, through an abbreviated version of the Wisconsin Sorting Card Test, where scores were obtained for the following indicators: correct answers, perseverative responses, number of categories and inability to maintain the organization.
- •
Planning and organization, through the “Pyramid of Mexico” test (similar to the Tower of Hanoi), yielding scores for the following indicators: correct designs and design with the fewest possible moves, number of and number of moves.
We used a case-control design32; the cases were participants who met the diagnostic criteria for CD and controls who did not meet these criteria. In the interest of research, we selected children between 6 and 12 years of age in the three educational institutions mentioned. To select children with CD, we previously asked the professional of each institution to develop a list of students to present the diagnostic criteria of the APA1, confirming the diagnosis through ChiPS27. Participants without CD were selected randomly from the rest of students without behavior problems and the same age range, selecting the same number of participants in the CD group, about half of each sex, confirming the absence of CD through the same instrument.
The parents of these children were asked their consent for their children to participate in this research, being provided with information regarding the objectives and the general procedure of the study, the confidentiality of data, independence of the investigation with respect to the school, the voluntary nature of participation and the respect for the decision to quit the research participation any time, possible discomfort for the duration of the tests applied and the ability to provide the results obtained through these tests. No monetary rewards were given to these parents. A semi-structured interview was made with each parent through the ENI's clinical history questionnaire26, in order to rule out other mental disorders, serious physical illness or major neurological disorders. Subsequently, each participant was individually briefed, the general conditions of the tests were explained, and administered in two to four sessions in order to avoid the effect of fatigue, verifying that each child was in good physical condition and encouraged to answer the tests. The tests were administered by qualified specialists in neuropsychological assessment and diagnosis, in the following order: ChiPS27, K-BIT28, and ENI26.
The two subsamples were compared, at a general level and by gender, as the average percentile scores in each of the domains and subdomains of cognitive and executive functions of the ENI26, where the one-way ANOVA was used, accepting a significance level less than .05 (bilateral). Also the two groups in the IQ test compound with the same statistics were compared.
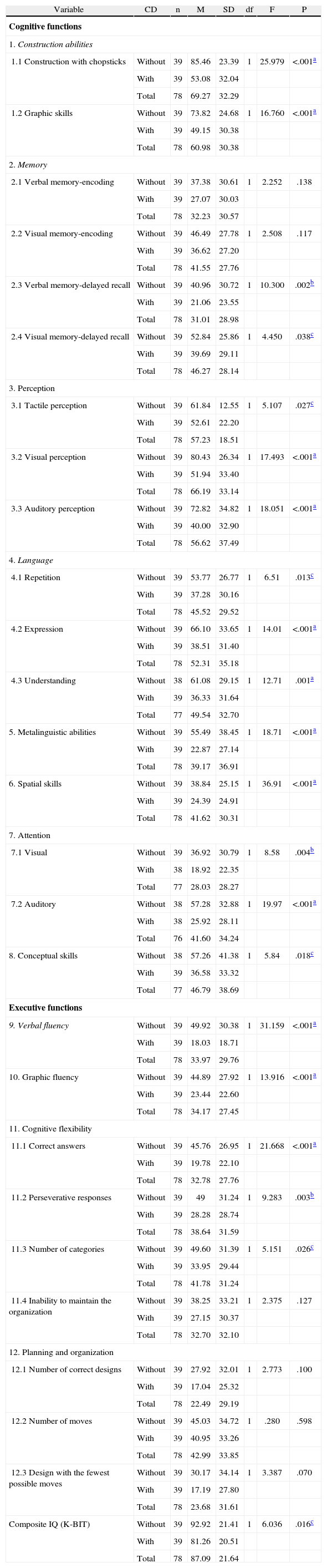
ResultsTable 1 presents the comparisons between cases and controls. Mean scores were statistically lower among cases compared with controls in almost all domains and subdomains of ENI26: constructional skills (building of toothpicks and graphic skills), perceptual skills (tactile, visual and auditory), delayed recall (verbal and visual), language (repetition, expression and understanding), metalinguistic skills, spatial skills, attention (visual and hearing), conceptual skills, verbal fluency, graphic fluency and the following indicators of cognitive flexibility: correct answers, perseverative responses and number of categories. The same occurred in relation to the average of composite IQ of both groups. No statistically significant differences were observed in the subdomains of memory-encoding (verbal and visual), an inability to maintain the organization (an indicator of cognitive flexibility) and indicators for planning and organization.
Group differences in mean percentile scores in executive and cognitive functions (one-way ANOVA).
| Variable | CD | n | M | SD | df | F | P |
| Cognitive functions | |||||||
| 1. Construction abilities | |||||||
| 1.1 Construction with chopsticks | Without | 39 | 85.46 | 23.39 | 1 | 25.979 | <.001a |
| With | 39 | 53.08 | 32.04 | ||||
| Total | 78 | 69.27 | 32.29 | ||||
| 1.2 Graphic skills | Without | 39 | 73.82 | 24.68 | 1 | 16.760 | <.001a |
| With | 39 | 49.15 | 30.38 | ||||
| Total | 78 | 60.98 | 30.38 | ||||
| 2. Memory | |||||||
| 2.1 Verbal memory-encoding | Without | 39 | 37.38 | 30.61 | 1 | 2.252 | .138 |
| With | 39 | 27.07 | 30.03 | ||||
| Total | 78 | 32.23 | 30.57 | ||||
| 2.2 Visual memory-encoding | Without | 39 | 46.49 | 27.78 | 1 | 2.508 | .117 |
| With | 39 | 36.62 | 27.20 | ||||
| Total | 78 | 41.55 | 27.76 | ||||
| 2.3 Verbal memory-delayed recall | Without | 39 | 40.96 | 30.72 | 1 | 10.300 | .002b |
| With | 39 | 21.06 | 23.55 | ||||
| Total | 78 | 31.01 | 28.98 | ||||
| 2.4 Visual memory-delayed recall | Without | 39 | 52.84 | 25.86 | 1 | 4.450 | .038c |
| With | 39 | 39.69 | 29.11 | ||||
| Total | 78 | 46.27 | 28.14 | ||||
| 3. Perception | |||||||
| 3.1 Tactile perception | Without | 39 | 61.84 | 12.55 | 1 | 5.107 | .027c |
| With | 39 | 52.61 | 22.20 | ||||
| Total | 78 | 57.23 | 18.51 | ||||
| 3.2 Visual perception | Without | 39 | 80.43 | 26.34 | 1 | 17.493 | <.001a |
| With | 39 | 51.94 | 33.40 | ||||
| Total | 78 | 66.19 | 33.14 | ||||
| 3.3 Auditory perception | Without | 39 | 72.82 | 34.82 | 1 | 18.051 | <.001a |
| With | 39 | 40.00 | 32.90 | ||||
| Total | 78 | 56.62 | 37.49 | ||||
| 4. Language | |||||||
| 4.1 Repetition | Without | 39 | 53.77 | 26.77 | 1 | 6.51 | .013c |
| With | 39 | 37.28 | 30.16 | ||||
| Total | 78 | 45.52 | 29.52 | ||||
| 4.2 Expression | Without | 39 | 66.10 | 33.65 | 1 | 14.01 | <.001a |
| With | 39 | 38.51 | 31.40 | ||||
| Total | 78 | 52.31 | 35.18 | ||||
| 4.3 Understanding | Without | 38 | 61.08 | 29.15 | 1 | 12.71 | .001a |
| With | 39 | 36.33 | 31.64 | ||||
| Total | 77 | 49.54 | 32.70 | ||||
| 5. Metalinguistic abilities | Without | 39 | 55.49 | 38.45 | 1 | 18.71 | <.001a |
| With | 39 | 22.87 | 27.14 | ||||
| Total | 78 | 39.17 | 36.91 | ||||
| 6. Spatial skills | Without | 39 | 38.84 | 25.15 | 1 | 36.91 | <.001a |
| With | 39 | 24.39 | 24.91 | ||||
| Total | 78 | 41.62 | 30.31 | ||||
| 7. Attention | |||||||
| 7.1 Visual | Without | 39 | 36.92 | 30.79 | 1 | 8.58 | .004b |
| With | 38 | 18.92 | 22.35 | ||||
| Total | 77 | 28.03 | 28.27 | ||||
| 7.2 Auditory | Without | 38 | 57.28 | 32.88 | 1 | 19.97 | <.001a |
| With | 38 | 25.92 | 28.11 | ||||
| Total | 76 | 41.60 | 34.24 | ||||
| 8. Conceptual skills | Without | 38 | 57.26 | 41.38 | 1 | 5.84 | .018c |
| With | 39 | 36.58 | 33.32 | ||||
| Total | 77 | 46.79 | 38.69 | ||||
| Executive functions | |||||||
| 9. Verbal fluency | Without | 39 | 49.92 | 30.38 | 1 | 31.159 | <.001a |
| With | 39 | 18.03 | 18.71 | ||||
| Total | 78 | 33.97 | 29.76 | ||||
| 10. Graphic fluency | Without | 39 | 44.89 | 27.92 | 1 | 13.916 | <.001a |
| With | 39 | 23.44 | 22.60 | ||||
| Total | 78 | 34.17 | 27.45 | ||||
| 11. Cognitive flexibility | |||||||
| 11.1 Correct answers | Without | 39 | 45.76 | 26.95 | 1 | 21.668 | <.001a |
| With | 39 | 19.78 | 22.10 | ||||
| Total | 78 | 32.78 | 27.76 | ||||
| 11.2 Perseverative responses | Without | 39 | 49 | 31.24 | 1 | 9.283 | .003b |
| With | 39 | 28.28 | 28.74 | ||||
| Total | 78 | 38.64 | 31.59 | ||||
| 11.3 Number of categories | Without | 39 | 49.60 | 31.39 | 1 | 5.151 | .026c |
| With | 39 | 33.95 | 29.44 | ||||
| Total | 78 | 41.78 | 31.24 | ||||
| 11.4 Inability to maintain the organization | Without | 39 | 38.25 | 33.21 | 1 | 2.375 | .127 |
| With | 39 | 27.15 | 30.37 | ||||
| Total | 78 | 32.70 | 32.10 | ||||
| 12. Planning and organization | |||||||
| 12.1 Number of correct designs | Without | 39 | 27.92 | 32.01 | 1 | 2.773 | .100 |
| With | 39 | 17.04 | 25.32 | ||||
| Total | 78 | 22.49 | 29.19 | ||||
| 12.2 Number of moves | Without | 39 | 45.03 | 34.72 | 1 | .280 | .598 |
| With | 39 | 40.95 | 33.26 | ||||
| Total | 78 | 42.99 | 33.85 | ||||
| 12.3 Design with the fewest possible moves | Without | 39 | 30.17 | 34.14 | 1 | 3.387 | .070 |
| With | 39 | 17.19 | 27.80 | ||||
| Total | 78 | 23.68 | 31.61 | ||||
| Composite IQ (K-BIT) | Without | 39 | 92.92 | 21.41 | 1 | 6.036 | .016c |
| With | 39 | 81.26 | 20.51 | ||||
| Total | 78 | 87.09 | 21.64 | ||||
Percentile ranks (Matute et al., 2007): above average, ≤84; average, 26–75; low, 5–16, and extremely low, ≤2.
CD participants showed an average of below-average scores (≤25), according to the scales provided by Matute et al26, in the following domains and subdomains: verbal memory delayed, metalinguistic skills, spatial skills, visual attention, verbal fluency, graphic fluency, correct answers, correct designs, and design with the fewest possible moves (table 1). Among men, we found the same differences that were evident across the board, except in repetition, where the average male (who met diagnostic criteria) did not differ statistically with respect to those of men who did not fulfill these diagnostic criteria (with CD, 38.23±29.58; without CD, 52.42±26.70): F[1, 49]=2,880; P=.096.
Thus, males with CD showed significantly lower scores on the following cognitive and executive functions, than males who did not fulfil these diagnostic criteria: a) construction with chopsticks (with CD, 54.40±31.28; without CD, 83.05±24.90): F[1, 49]=11,348; P=.002; b) graphic skills (with CD, 54.43±28.50; without CD, 72.10±26.86): F[1, 49]=4672; P=.036; c) tactile perception (with CD, 53.13±21.94; without CD, 65.10±6.84): F[1, 49]=5290; P=.026; d) visual perception (with CD, 53.16±34.93; without CD, 83.10±20.70): F[1, 49]=11 370; P=.002; e) auditory perception (with CD, 36.17±32.83; without CD, 68.47±39.11): F[1, 49]=9544; P=.003; f) delayed verbal memory (with CD, 20.68±21.69; without CD, 40.74±29.72): F[1, 49]=7443; P=.009; g) delayed visual memory (with CD, 34.47±28.24; without CD, 50.42±24.90): F[1, 49]=4056; P=.05; h) expression (with CD, 33.67±29.98; without CD, 66.89±30.08): F[1, 49]=14 243; P<.001; i) understanding (with CD, 35.17±32.13; without CD, 67.94±26.97): F[1, 49] =13 133; P=.001; j) metalinguistic abilities (with CD, 18.26±24.07; without CD, 52.84±35.44): F[1, 49]=16 575; P<.001; k) spatial skills (with CD, 22.18±25.13; without CD, 54.63±27.41): F[1, 49]=18 069; P<.001; l) visual attention (with CD, 20.86±24.65; without CD, 41.10±33.42): F[1, 49]=5828; P=.020; m) auditory attention (with CD, 29.93±30.51; without CD, 59.72±34.87): F[1, 49]=9486; P=.004; n) conceptual skills (with CD, 31.76±32.83; without CD, 56.33±43.31): F[1, 49]=4945; P=.031; o) verbal fluency (with CD, 20.16±19.36; without CD, 52.68±32.63): F[1, 49]=19 243; P<.001; p) graphic fluency (with CD, 24.80±23.41; without CD, 44.47±30.13): F[1, 49]=6562; P=.014; q) correct answers (with CD, 17.61±20.91; without CD, 43.41±25.60): F[1, 49]=14 859; P<.001; r) perseverative responses (with CD, 25.34±27.68; without CD, 42.68±30.12): F[1, 49]=4265; P=.044, and s) number of categories (with CD, 30.54±29.80; without CD, 50.00±32.37): F[1, 49]=4637; P=.036. Males with CD also had an average of composite IQ lower than males without CD (with CD, 79.73±19.97; without CD, 93.79±25.41): F[1, 59]=4657; P=.036.
Among women, meanwhile, it was evident that those who met the diagnostic criteria for CD had an average score lower in the following areas, compared with girls who did not meet diagnostic criteria for CD: a) construction with chopsticks (with CD, 48.67±36.07; without CD, 87.75±22.26): F[1, 29]=12 902; P=.001; b) graphic skills (with CD, 27.22±28.30; without CD, 75.45±23.01): F[1, 29]=23 660; P<.001; c) visual perception (with CD, 47.88±29.23; without CD, 77.90±11.31): F[1, 29]=5982; P=.021; d) spatial skills (with CD, 31.77±24.04; without CD, 62.85±22.78): F[1, 29]=11168; P=.002; e) visual attention (with CD, 12.66±11.20; without CD, 32.95±28.35): F[1, 29]=4235; P=.049; f) auditory attention (with CD, 13.00±12.27; without CD, 55.10±31.73): F[1, 29]=14 602; P=.001; h) verbal fluency (with CD, 10.88±15.17; without CD, 47.30±28.67): F[1, 29] =12 717; P=.001; i) graphic fluency (with CD, 18.88±20.22; without CD, 45.30±26.44): F[1, 29]=7061; P=.013; j) correct designs (with CD: 3.45±8.61; without CD, 26.60±32.36): F[1, 29]=4381; P=.046, and k) design with the fewest possible moves (with CD: 2.01±3.96; without CD, 32.55±36.07): F[1, 29]=6287; P=.018. Girls with CD did not have an average of composite IQ significantly different than the average of girls without CD (with CD, 86.33±22.71; without CD, 92.10±17.42): F[1, 29]=.563; P=.459.
DiscussionThe objective of this research was to evaluate cognitive and executive functions of a sample of school-age children with CD (not institutionalized), compared at a general level and by sex with a sample of children without the disorder with similar socio-demographic characteristics. The results showed that participants with CD had significantly lower scores on most cognitive and executive functions evaluated, confirming the relationship found between CD and neuropsychological deficits and the increased incidence of these deficits in childhood-onset CD7,14. Similarly, participants with CD had lower composite IQ scores than participants without CD, which confirms that individuals with CD could have below average IQ scores1,7.
The results show in particular that school males with CD had lower cognitive flexibility, an ability needed to change the focus and change the response in terms of environmental requirements and that unaffected children show good performance during their years in school24,33. The fact that children with CD showed a higher number of perseverative responses, indicative of low cognitive flexibility, demonstrates a lower sensitivity to errors and therefore, according to Rubia34, reduced sensitivity to punishment, a feature consistently found in studies showing a lower emotional reactivity in children and adolescents with CD17,35–37. CD girls, meanwhile, showed lower scores on two of the three indicators of planning and organization, indicating deficits in the functions necessary to the mental representation of a problem and planned cognitive and behavioral organization aimed at its resolution functions that are expected to be sufficiently developed in the school years24,33.
The results obtained with tests measuring executive functions corroborate, in general, the presence of some type of executive dysfunction which predispose them to the development of CD7,9,23,38, since these functions are necessary for emotional, cognitive and behavioral regulation14,23,39.
The low scores on verbal fluency among both boys and girls who meet the diagnostic criteria for CD and CD children with language and metalinguistic skills, on the other hand, are consistent with results obtained by other studies that found lower scores in verbal IQ, verbal fluency and verbal memory and processing15,16,18 and corroborate the importance of verbal information processing for emotional, cognitive and behavioural regulation, development of self-control and problem-solving skills, and learning of social and pro-social skills in which children with CD have difficulties12,14.
The lowest scores on visual attention, measured by tests of cancellation of drawings and letters and auditory attention, as measured by digit retention in progression and regression tests, support the existence of deficits in executive functions of the sample, since the control of attention is considered an executive function and digit regression is considered a working memory test, another executive-type function considered33,40. These findings, in turn, are consistent with the results of Toupin et al41, who found a significantly higher number of symptoms of attention deficit disorder with hyperactivity (ADHD) among children and adolescents with CD. The results of the meta-analysis by Willcutt et al40 show that in this sense, children and adolescents with ADHD may experience lower scores on vigilance and working memory, two functions measured through tests of attention in which children with CD in this study showed lower scores.
The results obtained in spatial skills in both boys and girls with CD and delayed verbal and visual memory, in the case of children with CD are also consistent with previous findings showing lower scores on spatial and memory functions among children with CD14. Although girls with CD did not have lower scores on verbal and visual memory like the boys, they did show lower average scores on the digit retention in regression, a task which, as already indicated, is related to working memory.
The results also show deficits in constructional skills, visual, tactile and auditory perception, conceptual skills and graphic fluency, indicating the possibility of a lower generalized cognitive development in many schools with CD, which is consistent with the lower CI obtained by children with CD, compared with children without CD, but not girls with this disorder. These deficits may not only predispose to the development of CD, because of its importance in the development of other areas such as social and moral42, but that might be related with lower academic performance and academic failure, common features in children with CD6,7. The lower scores on visual and auditory perception, in particular, are consistent with those already reflected lower scores on visual and auditory attention and point out that those school children with CD may have difficulties in primary and secondary processing of these two types of information.
The results also indicate several common features among school boys and girls with CD, at the level of constructional skills, visual perception, spatial skills, visual and auditory attention and verbal fluency and graphics, but also differences in the sense that girls affected by CD did not have lower scores on language and metalinguistic skills, tactile and auditory perception, verbal and delayed visual memory, conceptual skills and cognitive flexibility. In addition, these girls exhibited lower scores in planning and organization, unlike children with CD, who in this study showed no statistically significant differences in these functions, compared with children without CD. The results of this study also indicate that men with CD often have a composite IQ lower than women with this disorder.
These sex differences suggest that male and female school children with CD demonstrate common neuropsychological characteristics, as outlined in the literature, such as low verbal fluency deficits in memory and spatial skills, but differ according to the results obtained, in which males have more pronounced deficits in cognitive flexibility and on the verbal level, while women have more deficits in planning and organizing, but not as pronounced on the linguistic level. The fact that men with lower CD scores in a larger number of subdomains compared with girls with CD, on the other hand, shows that males with CD would be more likely to exhibit these neuropsychological deficits than schoolgirls with this disorder. It is possible that these differences are situated in, according to Eme14, a biological predisposition of ales, which explains, in turn, the increased prevalence of CD among them6–8.
Finally, it is important to note that although this research has its strengths in the use of a comparison group, using a validated neuropsychological battery with a Colombian sample and the control of several potential sources of error such as IQ, socioeconomic status and the presence of other mental disorders or serious physical illnesses, reveals two important limitations that should be remedied in future research. First, this study only examined “cold” executive functions, such as planning, self-regulation, mental flexibility and control of attention, but not “hot” function types, i.e. those related to motivational and affective processes and incentives33,34, and therefore would generate other research that may yield a more complete profile of executive functions in school children with CD. Second, this study involved the participation of a relatively small sample of male and female students with CD, so it is necessary to confirm the results obtained with larger samples, particularly of girls with CD.
Conflicts of interestsAuthors have no conflict of interest to declare.

