




Objetivo: La infiltración con resina es una innovadora técnica microinvasiva, donde los tejidos duros son preservados, que ha sido usada para tratar estadios medios de caries. El objetivo de este estudio es evaluar con microscopio laser confocal la técnica indirecta de tinción en dientes con diferentes grados de fluorosis.
Métodos: Veinticuatro molares y premolares humanos con fluorosis fueron infiltrados y fotocurados. Los especímenes fueron preparados y las lesiones (FDmax), así como la profundidad de penetración fueron analizadas usando el método de fluorescencia dual en el microscopio láser confocal.
Resultados: El porcentaje de penetración fue significativamente mayor en dientes con fluorosis leve y muy leve, a diferencia de los especímenes con fluorosis moderada y grupo control en los que el porcentaje de penetración fue significativamente menor (p < 0,05, test de Bonferroni). Sin embargo, no hubo diferencias significativas entre el grupo mode-rado y control, ni entre los grupos leve y muy leve (p > 0,05, test de Bonferroni).
Conclusión: Se puede concluir que la penetración de la resina en dientes con fluorosis leve y muy leve es mayor que en los dientes con lesiones moderadas.
Objective: Resin infiltration is an innovative microinvasive measure, whereby hard tissues are preserved, that has been used to treat medium stages of caries.
The aim of this study is to evaluate with Confocal laser scanning microscopy the indirect staining technique of resin infiltration in teeth with different degrees of fluorosis.
Methods: Twenty-four fluorosed human molars and premolars were infiltrated and light cured. Specimens were prepared and lesions, as well as penetration depth were analyzed using dual fluorescence method in confocal laser microscopy.
Results: Percentage penetration, was significantly higher in teeth with mild and very mild fluorotic lesions, unlike moderate and control group which was significantly lower (p < 0.05, Bonferroni test). However, there are no statistically significant differences between control and moderate groups neither between very mild and mild groups (p > 0.05, Bonferroni test).
Conclusion: It can be concluded that resin penetration in mild and very mild fluorotic lesions is higher than in moderate lesions.
Introducción
Fluorotic enamel is characterized by an outer hypermineralized, acid-resistant layer and retention of more porous in the areas of subsurface hypomineralization. The pores are occupied by water as well as enamel secretory proteins which are retained due to the effect of the excessive fluoride level on ameloblasts1-3.
During amelogenesis, ameloblasts secrete a protein matrix composed by more than 90% of amelogenin, a specific ameloblast protein, which must be degraded by proteases to start mineralization. Proteases have their greatest proteolytic activity at a high concentration of Ca++. Fluoride is highly electronegative, and reacts with free Ca++ ions inhibiting the proteolytic activity and leaving areas with protein matrix remnant, without minerals, resulting in hypocalcified enamel pores2,4.
There are two main classifications for dental fluorosis5 (Fluoride in drinking water). Dean's index that ranks dental fluorosis in four levels of severity, according its clinical appearance6, and Thylstrup and Fejerskov index that classify dental fluorosis regarding its clinical appearance in relation to histologic changes7. Dean index is the most used to assess the prevalence and severity in many U.S. communities8.
Dental fluorosis remains highly prevalent condition. A report shows a prevalence of enamel fluorosis in USA of 23%, mainly in its mild and very mild degrees9. This is consistent with studies in Chile10 where the prevalence of fluorosis reached 31.2%, corresponding to the following classifications: 14.4% to questionable, 12.9% to very mild and 2,4% to mild.
Although fluorosis has a high prevalence, its severity is low, that is the reason why EPA (US Environmental Protection Agency) considers it to be a cosmetic effect and not a public health problem11.
Depending on its severity, there are several treatment options for enamel fluorosis, such as micro-abrasion, bleaching, composite restorations, veneers and crowns12.
On the other hand, there has been recent advances in adhesive dentistry, with the development of micro-invasive technique of caries infiltration, an innovative approach to treat medium stages of caries that fills the gap between preventive and invasive measures, whereby hard tissues are preserved. To evaluate this by confocal laser microscopy, there has been use the indirect staining techniquethat involves the application of 15% HCl to allow the infiltration of a low viscosity, light curing resin, blocking the diffusion pathways for cariogenic acids and reduces lesion progression13. Infiltrated lesions lose their whitish appearance and look similar to sound enamel; this might be an alternative to microabrasion and restorative treatment, in particular for white spot lesions of esthetically relevant14, as fluorosis.
Hence, the aim of this study is to evaluate with Confocal laser scanning microscopy the depth of resin infiltration in teeth with different degrees of fluorosis in which the use of this micro-invasive treatment could be a significant contribution to the solution of a cosmetic problem that is highly prevalent and increasing. We hypothesized that moderate lesions has a lower penetration compared with milder lesions.
Materials and methods
Teeth selection
Twenty-four fluorosed human molars and premolars [Dean Index: very mild, mild and moderate (Dean, 1942)], extracted for orthodontic reasons, from the cities of Viña del Mar and Valparaiso, Chile (0.6 ppm F), were selected for this study. The teeth were collected after the consent of patients. Then they were allocated to 3 groups (moderate, mild and very mild) regarding its degree of fluorosis, using Dean Index. Control was the etched and infiltrated sound enamel surrounding the fluorotic lesion. Teeth were stored in a 0.9% NaCl solution at 4°C for 30 days before the experimental procedure. Diagnosis and classification (8 teeth per group) was made by consensus of three researchers (VQ, RP and SG. Kappa Interexaminer = 0.83).
Specimen Preparation
Each tooth was mounted in an acrylic cube to facilitate its handling. The teeth were processed according to the indirect staining technique described by Paris et al. Fluorotic lesion surfaces were etched with 15% hydrochloric acid gel for (Icon, DMG Hamburg), for 2 minutes. To label all accessible porosities with the red fluorophore, specimens were stored in an ethanolic solution of 0.1% RITC [red fluorophorerhodamine B isothiocyanate (RITC 0.1%); Sigma Aldrich, Steinheim, Hamburg, Germany] for 12 h. Subsequently, teeth were dried using compressed air for 10 s and infiltrant resin (ICON, DMG, Hamburg, Germany) was applied onto the fluorotic surface. After 3 min, excessive material was wiped away using a cotton pellet and the material was light cured for 60 s. To bleach all red fluorophore that has not been enclosed by the infiltrant resin, specimens were stored in 10% hydrogen peroxide solution for 12 h at 37°C. Finally, teeth were washed with water for 60 s.
The teeth were cut perpendicular to the surface across the lesions with a Precision Saw (IsoMet 1000, Buehler, Lake Bluff IL, USA) in order to obtain sheets of 1 mm thick. Then, the specimens were carefully polishing (Abrasive Paper 500, 600 and 1200 grit; ISESA), and 100 um thin sections were prepared and fixed on object holders. To visualize porous structures (e.g., not infiltrated lesion parts), specimens were immersed in a 50% ethanolic solution of 100 uM sodium fluorescein (NaFl; Sigma Aldrich) for 3 min. Subsequently, specimens were washed in deionized water for 10 s. We chose the most representative sample for each tooth, thus 24 samples were analyzed.
Confocal Laser Scanning Microscopy
Specimens were observed using a confocal laser scanning microscope CLSM, (Arquimed, Olympus Fluorview, FV1000, Japan). We used 10x and 60x objectives with dual fluorescence mode, where RITC and NaFl fluorescence can be detected simultaneously (RICT: Ex 543nm, NaFl: Ex 488nm). Two dimensional images (xy-scan) were obtained.
Image Analysis
To achieve reproducible measurement of fluorotic lesion depths and resin penetration depths, ten markers per image were set, the deepest points of the lesions. Lesion depths were assessed by two observers independently using the Olympus Fluorviewer program (Fluorviewer 3.0., Olympus, Japan). Observers were calibrated previously and measurements were repeated by the observers after one week.
Resin penetration depth (PD), and the remaining porosities not infiltrated (FD) were measured by the 10 selected points and the mean depth number for penetration and lesion depth was obtained. Using the mean depth number of Rhodamine and Fluorescein we calculated the percentage of penetration of the resin in all fluorotic lesions.
Statistical Analysis
Statistical analysis was performed using SPSS software (SPSS for Windows 11.5.1; SPSS Inc., Chicago, IL, USA). Percentage penetration was calculated as PD (Penetration Depth)/ FDmax (Fluorosis Depth) x 100. Differences in lesion and penetration depths, as well as percentage penetration, were analyzed using Bonferroni test. The level of significance was set at 5% for all tests.
Results
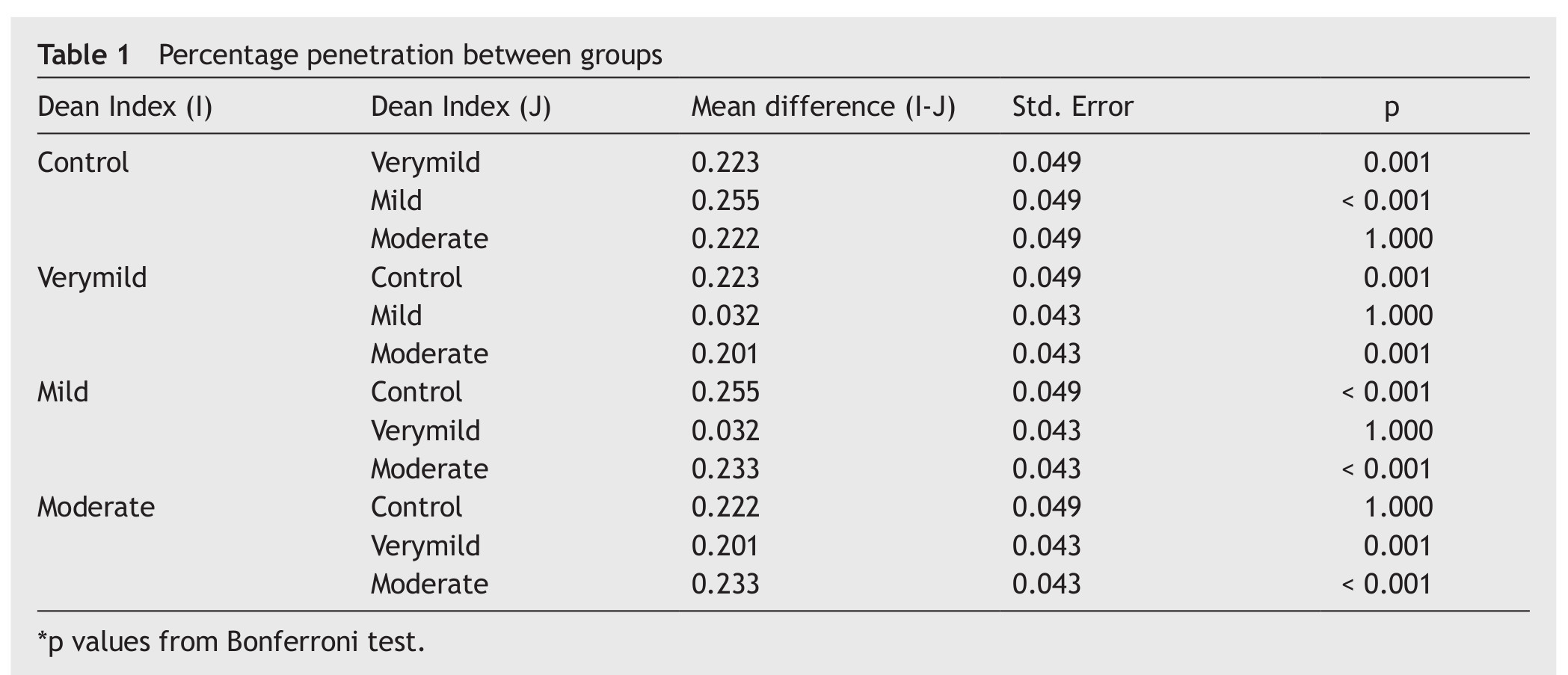
Analysis of images taken with CLSM, using dual fluorescence mode, allows measurements of the infiltrant penetration and the remaining pore structures. The infiltrant is represented by the red colordue to staining with rhodamine, whereas remaining porous structures as non infiltrated parts of the enamel defect (fluorotic lesion) appeared green because of the fluorescein dye. Nonporous structures like sound enamel without etch, showed no fluorescence and were displayed dark (fig. 1).
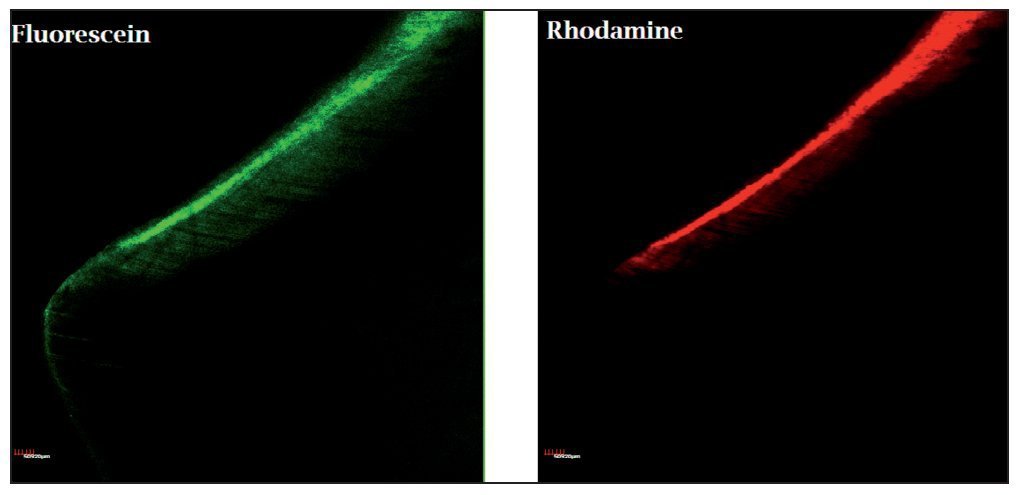
Figure 1. CLSM Image of infiltrated fluorotic lesion. Porosites in enamel are displayed green, whereas infiltrated lesion parts appear red. Solid material as sound enamel shows no fluorescence and are displayed black. Selective visualisation mode.
Images show a superficial penetration depth on moderate fluorotic lesion and control, meanwhile on mild and very mild fluorotic lesions penetration depth was higher (fig. 2).

Figure 2. Representative images of penetration depth of: a) control, b) moderate, c) mild, d) very mild fluorotic lesions. 10x objective in dual fluorescence mode.
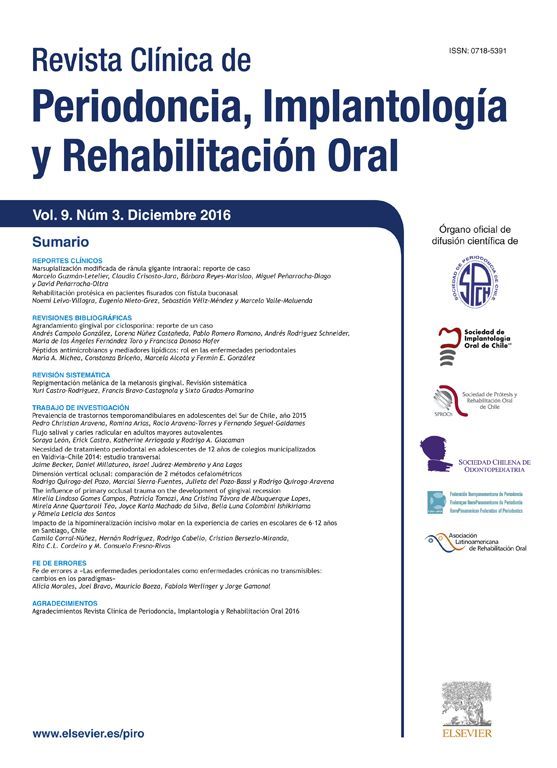
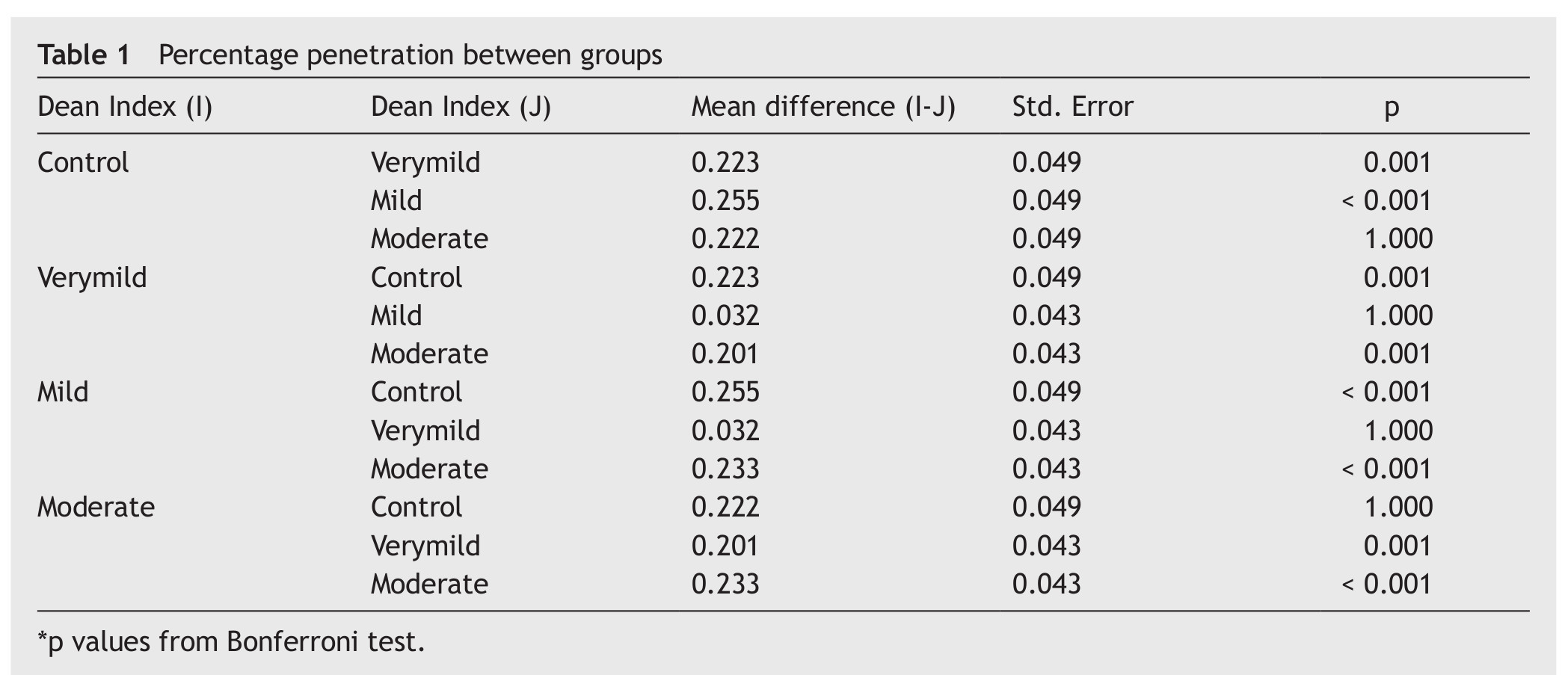
The higher values of resin penetration were 204.314 μm in very mild group and 141.648 μm in mild group. On the other hand, resin penetrated 9.894 μm in moderate group, and 3.870 μm in control group, which is much lower than the first two groups. The median value of percentage penetration in very mild and mild group was 74% and 79% respectively. In the moderate group was 54% and 55% for the control group. Comparing the difference in percentage penetration between groups, is significantly higher in teeth with mild and very mild fluorotic lesions, unlike moderate and control group which was significantly lower (fig. 3) (p < 0.05, Bonferroni). However, there are no statistically significant differences between control and moderate groups; and between very mild and mild groups (p > 0.05, Bonferroni) (table 1).
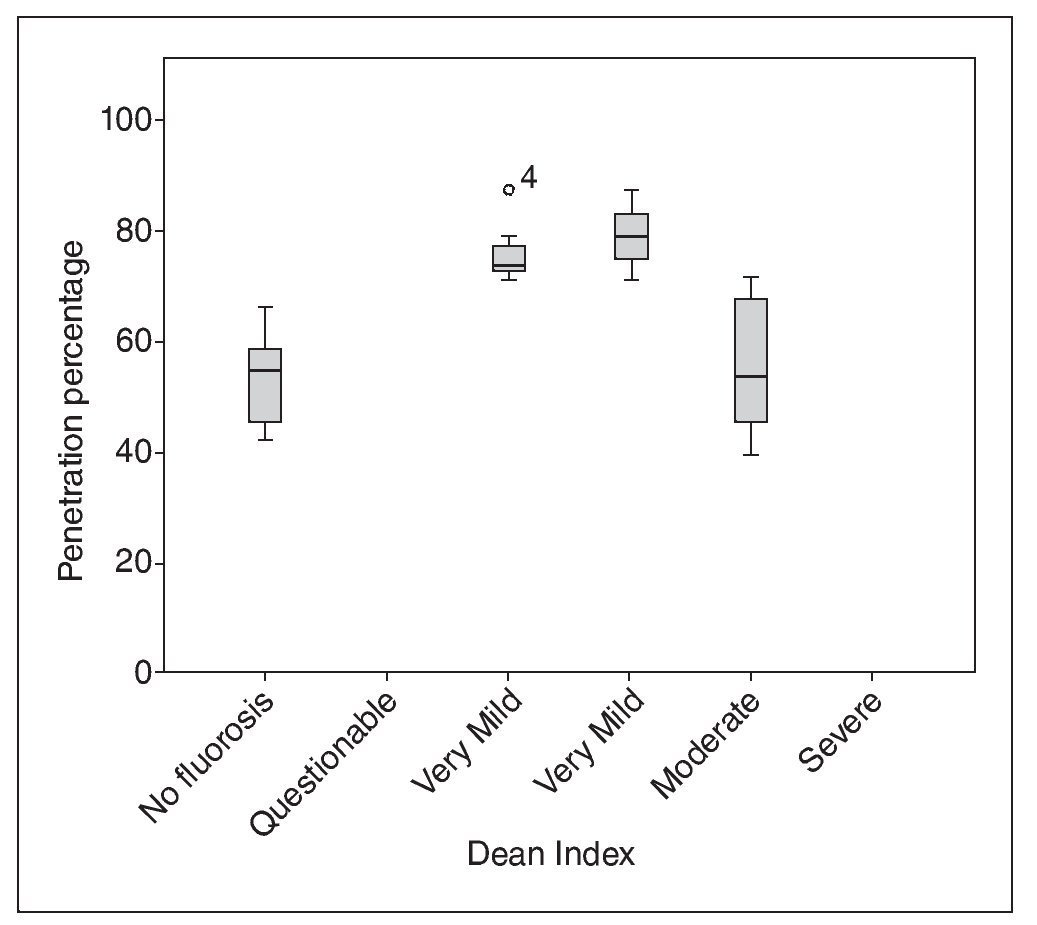
Figure 3. Box plots of the percentage penetration in the three groups of fluorotic lesions (Dean: moderate-mild-very mild) and control (no fluorosis) evaluated.
Discussion
This in vitro study shows that the infiltrant resin used is capable to penetrate several micrometers into all the fluorotic lesions evaluated regardless lesion severity. The study hypothesis was confirmed, since significant difference in percentage penetration was found between moderate lesions (and control) and the milder forms of fluorosis. Furthermore, deepest penetration could be observed only in milder lesions, meanwhile on moderate lesions, penetration depths were lower. This means that there were factors that prevented a further penetration of the resin on moderate lesions and that have allowed greater infiltration on milder lesions.
Resin penetration into enamel caries lesions has been investigated using many different observation techniques. Fluorescence confocal microscopy is a useful tool to analyze the infiltration of enamel caries lesions with low-viscosity resins in vitro15 showing an almost complete penetration into natural lesions16.
The use of multiple fluorescence stains allows selective visualization of different material or even molecules and therefore, is frequently applied in confocal microscopy15. Rhodamine and fluorescein derivates allow selective visualization due to well-separated excitation and emission wavelengths17. Therefore, these are the most commonly used fluorophores in dental research15.
Direct staining technique, that was the conventionally technique used to visualize infiltrant penetration into natural enamel caries lesions, which comprises dye labeling of the resin, has been shown to be limited by chromatographic separation of the resin-dye-mixture during penetration. Also, staining of resin prior to penetration in the enamel can lead to erroneous interpretations of the images, so that; the fluorophore was not present in all infiltrated lesion parts leading to an underestimation of penetration depth15. Therefore, the indirect staining technique was used in this study because of its more valid and reliable results to this type of visualization.
Enamel fluorosis is featured histopathologically as a subsurface hypomineralized lesion covered by a hypermineralized outer enamel surface4, behaving as a noncavitated enamel caries lesion. Both present clinically as a white spot, interfering with the aesthetics18.
Al-Sugair and Akpata 1999 study19 shows that fluorapatite in the hypermineralized surface layer of fluorosed teeth is more resistant to acid dissolution than the hydroxyapatite in non-fluorosed teeth. Despite this, in clinical practice, etching time of fluorosed teeth with the milder forms should be same as for non-fluorosed teeth. But, the etching time of moderate fluorosed teeth should, at least, be doubled. Therefore, etching time on fluorosed teeth, with different degrees of severity, could be a factor involved in the lower penetration on moderate lesions and the higher infiltration on mild and very mild lesions.
Moreover, fluorosed enamel retains a high proportion of immature matrix proteins due to an incomplete removal during development. Fluoride affects Ca-dependent protease activities responsible for the degradation of enamel proteins. With increasing severity, the subsurface enamel all along the tooth becomes increasingly porous, and the lesion extends toward the inner enamel2.
It has been studied that in vivo remnants of proteins within caries lesions might hamper penetration of infiltrants16 and it is likely to happen something similar in fluorotic lesions, especially on moderate ones because of its extension and amount of proteins retained inside the lesion body owing to the lack of degradation and subsequent mineralization.
After conditioning of the lesion surface using hydrochloric acid gel, a resin infiltrant is applied on the lesion. The infiltrant used in this study, is a light-curable resin that is optimized for rapid penetration into the capillary structures of the lesion body14. These materials show a very low viscosity, low contact angles to enamel, and high surface tensions20. Studies of resin infiltration in caries lesions allow a better appearance, because the infiltrant is capable of penetrating deep into the lesion21.
Hydrochloric acid in similar concentrations as used in the present study is widely accepted in aesthetic dentistry to remove superficial discolorations by enamel microabrasion22. Previous research showed that 18% HCl and pumice removed 7 to 22 μm and 36 to 62 μm of surface enamel on 5 s and 25 s applications respectively23. The infiltration technique demands the application of 15% hydrochloric acid, to promote erosion of the surface layer (less than 30 μm of demineralized enamel)24. Fluorosed teeth have the highest concentration of fluoride in the outer 200 μm of enamel25, and this makes them highly resistant to acid etching19.
In a recent study ICON®-DMG was applied to mask white spot lesions and evaluated the color change; they demonstrated that resin has a refractive index of 1.475, which is closer to the refractive index of enamel (1.65). Thus, the difference in refractive indices between porosities and enamel is reduced and lesions regain translucency, appearing similar to the surrounding enamel. So they concluded that resin infiltration was proven to be an effective treatment for masking white spot lesions18. This leads to further researches regarding to correlate the results of this study with aesthetics parameters.
It can be concluded that resin penetration in mild and very mild fluorotic lesions is higher than in moderate lesions.
Conflict of interest
The authors declare that there are no conflicts of interest.
Acknowledgments
We would like to express our special thanks of gratitude to Dr. Diego de Nordenflycht (UNAB), Dr. Felipe Barros (CECS), and Genaro Alvial (Institute of Anatomy, Histology and Pathology, Faculty of Medicine, Universidad Austral de Chile). Samples of ICON were kindly provided by Dierk Lubbers from DMG GmbH, Germany. Part of this work was presented at IADR Chile meeting. This paper is based on a thesis submitted by two of the authors (RP, VQ) to the Universidad Austral de Chile in part fulfillment of the requirements for a BDS degree.
Recibido el 8 de mayo de 2013
y aceptado el 25 de septiembre de 2013
* Corresponding author.
E-mail:romina.perez.a@gmail.com (R. Pérez).