




Se conoce como sarcopenia al progresivo deterioro muscular que se produce con el paso de los años y que se caracteriza por una pérdida progresiva de fuerza y masa musculares, aumento de la grasa muscular y el deterioro progresivo de la capacidad funcional. Este proceso tiene importantes repercusiones en la calidad de vida de las personas mayores, ya que es causa frecuente de discapacidad, dependencia y aumento de la morbimortalidad. En la presente revisión bibliográfica del tema, analizamos los diferentes factores etiológicos y las estrategias de prevención y tratamiento de la sarcopenia, entre las que el ejercicio, y en particular el entrenamiento de fuerza, junto con una alimentación adecuada, desempeñan un papel primordial.
Sarcopenia is known as a progressive muscle wasting produced as years accumulate and characterized by a progressive loss of muscle mass and strength, increase of muscle fat and progressive decline of functional capacity. This process produces important and severe effects on quality of life in elderly people since sarcopenia is the most frequent cause of discapacity, dependency and increase or morbi-mortality. In the present review we analyze the different etiological factors and the prevention and treatment strategies against sarcopenia. One of the main strategies is the strength training that, added to an adequate nutrition, plays a primordial role in prevention and progression of sarcopenia.
Introduction
After reaching adulthood, humans and most mammals suffer a progressive decline of strength and muscle mass as time goes by. This is accompanied by a functional capacity loss and a raise of fat in muscle. Importantly, all these factors affect quality of life of the elderly causing frailty, dependency and the increase of morbi-mortality1-5. This progressive deterioration of muscle capacity is known as sarcopenia (From the Greek: sarco: muscle and penia: wasting, loss). In a classical way, an individual was considered as suffering sarcopenia when muscle parameters values were lower than two standard deviations from the values of a referenced young population. However, the current tendency includes in the definition of sarcopenia some other parameters related to strength, functional capacity of the subject and corporal fat amount6,7. This tendency distinguishes between an aging-dependent process (primary sarcopenia) and a pathological process (secondary sarcopenia)8-16. New concepts such as dinapenia or the age-associated loss of strength17 or new techniques such as proteomics18 or genomics19 must be considered in future studies of this pathology.
Etiology and particular characteristics of sarcopenia in the elderly
Several authors indicate that muscle mass reaches the maximum amount around the 30s and after that, it declines at a rate of 3-8% per decade. Decline rhythm accelerates from the 50s reaching 12-15% per decade9,11,20. Women show a higher decrease of muscle mass, especially after menopause. Regarding muscle quality, the capacity to produce strength per unit of muscle, different longitudinal studies have reported an important decrease during aging9,21-25. European population data about sarcopenia prevalence in people older than 65 years indicate a ratio moving from 9.5 to the 15.7%. These values rise as the population get older13. When compared with woman showing normal bone mineral density (0.8%), sarcopenia is more frequent in women suffering osteopeny (25%) and osteoporosis (50%)2. This relationship is probably due to related etiological mechanisms26. Furthermore, we can speculate that physical activity, able to maintain muscle mass, will help to maintain bone mass. This effect will be especially good in women since they show higher osteoporosis prevalence27.
The reduction of muscle mass in aged people does not affect in the same way to arms and legs. Muscle wasting is higher in lower limbs with independency of the sex of the person. However, when functional parameters, such as muscle quality, are taken into consideration, we can find sex-dependent differences. Men suffer a higher loss in upper limbs than women whereas no differences in the deterioration of muscle mass rate in lower limbs have been found. These differences could be due to the fact that women are more able to maintain a higher activity in arms due to domestic duties11,28. Reduction of muscle mass in lower limbs is, however, more important since it produces a severe functional decline in people's capacity29.
Aging-related sarcopenia seems to depend on the chronic inflammation process affecting most of the elderly30, aggravated by fat infiltration in the muscle11,31 and sarcopenic obesity. Sarcopenic obesity is characterized by the pathological increase of body fat accompanied by a decrease in muscle and bone mass. In these patients, excessive amount of calories in the diet produces a higher loss of muscle mass32. Obesity seems to contribute, even more than sarcopenia, to the lower functional capacity of these subjects6. Further, co-morbid diseases common to older individuals such as cancer, kidney disease, diabetes and peripheral artery disease can also accelerate the progression of sarcopenia in elderly people33.
Two mechanisms are involved in the decrease of the muscle mass in humans: reduction of the number of muscle fibres and reduction of the cross-sectional area of existing fibres. Aging does not affect in the same way to all the types of fibres. Type II fibres are the most affected. In consequence, important functional incapacity appears due to the decrease of production of rapid strength or to carry out power in muscle31,34. This is due to the lower resistance of this kind of fibres to the denervation11,35, deficiencies in gene expression of myosin type II35,36 and a lower resistance of these fibres to oxidative stress37. All these mechanisms could be related to testosterone deficit found in old people34.
Reduction of muscle fibre mass is also produced by intrinsic factors in myocytes. In aged people muscle mitochondria dysfunction accumulates. This deleterious effect is caused by accumulation of mtDNA damage that negatively affects the metabolic rate, protein synthesis and ATP production. Al these effects end in the death of the muscle fiber11,38. Moreover, regeneration and repair mechanisms of muscle fibre are also compromised in elderly people due to a lower activity of satellite cells31, chronic inflammation39, oxidative stress35,40, abnormal response of the microRNA41 and an inadequate regulation of the repair processes in damaged muscle fibres39.
Aged muscle is characterized by a delay in the peak of muscle contraction, an increase in the time of muscle relaxation, diminution in strength and reduction of the oxidative metabolic capacity35,42. These alterations are due to the accumulation of oxidative stress damaged proteins and DNA, especially mtDNA35,43, mitochondrial dysfunction, alteration of the transport of calcium35,40 and malfunction of contractile proteins37. Disappearance of muscle fibres forces to surviving fibres to compensate, or partially correct the compelled deficit to maintain the optimal capacity to generate strength44.
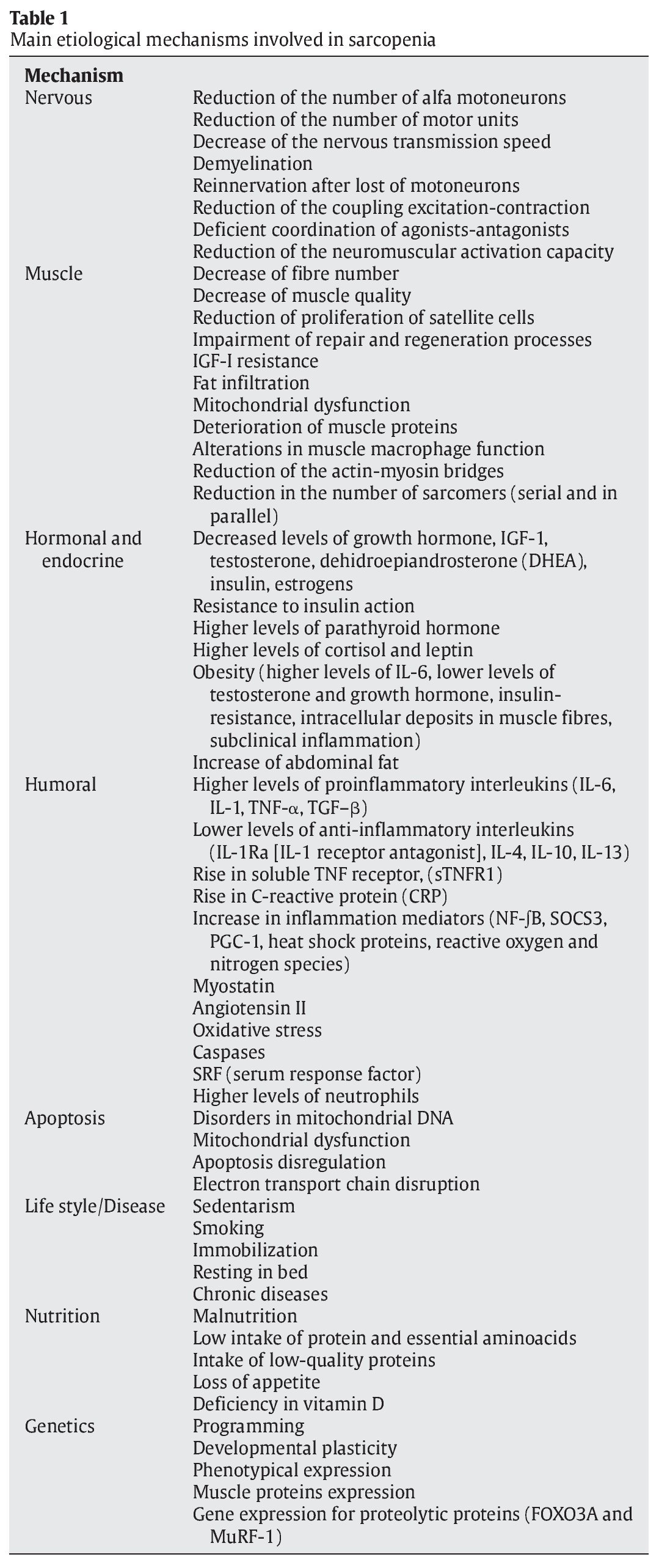
All these reasons permit us to affirm the multifactorial etiology of sarcopenia9-11,16,20,27,30-31,35,37-40,42,45-63. The different concerned mechanisms involved in muscle loss are indicated in table 1 and figure 1.
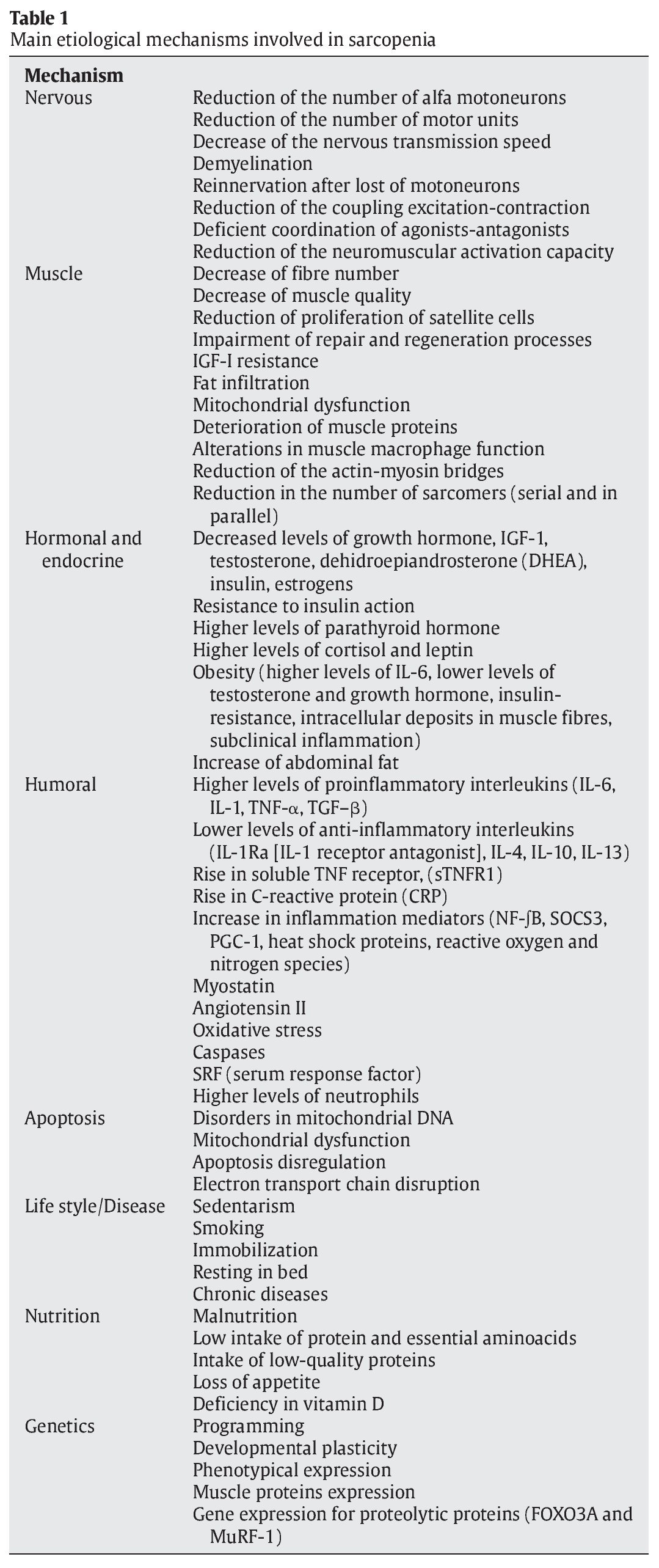
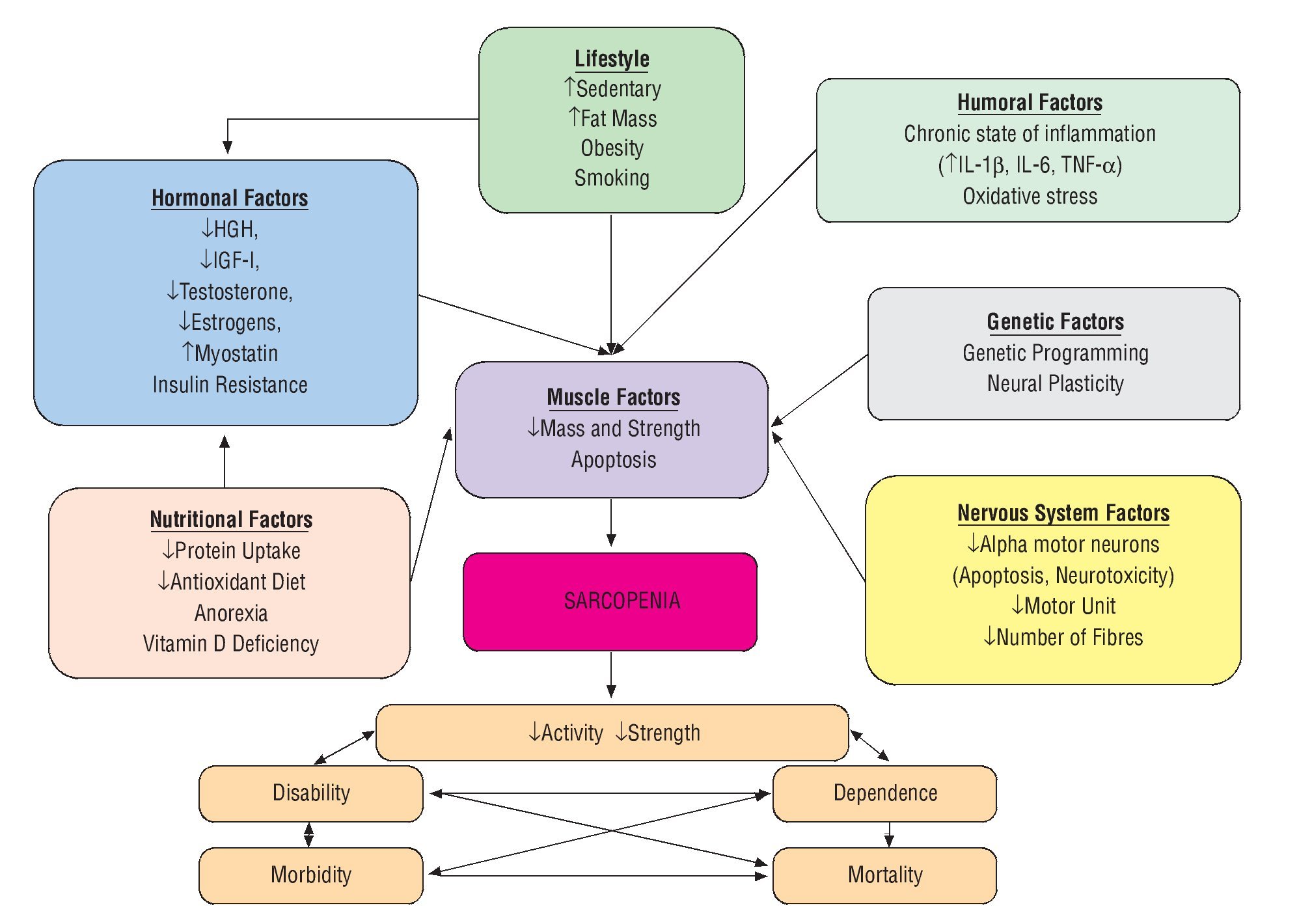
Fig. 1. Scheme of the different etiological sarcopenia mechanisms and their consequences.
Prevention and treatment of sarcopenia
Physical exercise, nutrition and pharmacological approaches have been proposed as mechanisms for and treatment of sarcopenia10-11,16,35,64-79. However, to date, no pharmacological procedures have demonstrated any efficiency in the prevention of sarcopenia in humans62. This pharmacological inefficacy must be due to the complexity of sarcopenia. For this reason, clinical trials of drug testing for treatment of sarcopenia must include significant improvement of physical performance, falls, fractures and functionality and quality of life80.
Preventive measures must be maintained during the whole life of the person. These measures consist in the practice of regular resistant and aerobic exercise and an equilibrated diet. These mechanisms require the increment of the uptake of high-quality proteins, showing fast absorption and high contents of leucine11,12,35,49,58,81, adequate uptake of antioxidants, caloric restriction and reduction of the deficit of vitamin D or inappropriate loss of weight10-11,54-56,62,82-85. Nutritional measures are of special interest because elderly people showing recurrent pathologies86 or in the case of sarcopenia-suffering obese old people85, reduce physical activity. In fact, in the obese sarcopenic elder, physical exercise, together with a moderated caloric restriction, seems to be the optimal method to reduce fat mass and avoid the muscle mass wasting85.
The metabolic effect produced by resistance exercise in old people must be accompanied by an adequate protein intake58. Since ancients show a decrease in the protein metabolism87, it is recommended that protein intake must be at least 1.0 to 1.3 g/kg body weight per day. This intake must be homogeneously distributed among all the meals during the day. Further, these proteins must show a high biological quality as higher content of branched-chain aminoacids (BCAA) such as leucine. Other nutritional measures such as antioxidant dietary supplementation, omega-3 acids or compensation of the vitamin D deficit have demonstrate to be efficient in the treatment of sarcopenia16,62,83,88,89. These nutritional measures are very important when muscle catabolism increases because inactivity periods86.
Regarding pharmacological procedures against sarcopenia, several pharmacological compounds have been used. However, their secondary effects and their moderated or null effect advise against their use in the treatment of muscle wasting. Some of these compounds such as angiotensin I to II-conversion inhibitors (ACE Inhibitors), simvastatin, androgenic receptor selective agonists, ibuprofen and paracetamol have demonstrated some efficacy in the treatment of sarcopenia. However, their definitive role in this pathology needs to be clarified11,12,20,35,77,78,90,91.
Role of physical exercise in prevention and treatment of sarcopenia
Resistance exercise
Resistance exercise o muscle potentiation has demonstrated a great efficacy in the treatment and prevention of sarcopenia. In fact, increases in muscle mass, strength and quality and also a better neuromuscular adaptation have been reported after the practice of exercise programs including different exercise protocols11,12,16,35,58,67,92-97. After analyzing the different recommendations of several associations such as the American College of Sport Medicine and the American Heart Association, and the results of the main studies performed about exercise, aging and sarcopenia, we suggest that the recommended exercise must contain resistance training including several exercises circuits with the 70-90% of the one repetition maximum (RM), with an exercise predominantly eccentric and performed, at least, every two non-consecutive days11,35,58,93,98,99. Since the abandon of the resistance training ends in a fast waste of muscle mass, we advise that a maintenance exercise must be performed including, at least, a week session with the above indicated exercises and intensities100-102. However, the clinical status of elderly people must be taken into consideration and obliges to individualize training programs35.
Furthermore, several other added beneficial effects of resistance exercise to the health of elderly people must be taken into consideration. In fact, the practice of physical exercise also exerts a positive effect in the preservation of cognitive function5.
Aerobic exercise
Aerobic exercise delays the strength loss and phenotypic changes produced during aging in muscle fibers35,84, even at moderated intensities101. However, the effects of aerobic exercise are modest and its definitive effect on sarcopenia is not completely clarified62. Then, it seems clear that the combination of both, resistance and aerobic exercises is more healthy for elderly people since it produces multiple benefits preventing and treating prevalent diseases at old ages5,31,59,62 or in particular situations such as sarcopenic obesity32,52,85.
Mechanisms of action of exercise on sarcopenia
There are multiple mechanisms by which resistance exercise prevents and ameliorates sarcopenia. We considered that it is worth to detail these mechanisms. Although these mechanisms are widely overlapped, we will analyze the effects of resistance exercise at muscle and neuro-motor levels (fig. 1).
At the muscle level
At the muscle level, resistance exercise neutralizes several of the mechanisms involved in the development of sarcopenia. This kind of exercise induces positive changes in the inflammation status, apoptosis of muscle fibre, regeneration of these fibres and the function and anatomy of muscle. Regarding the function of muscle, resistance exercise increase muscle quality through the increase in the number of sarcomera in parallel but also serial number103, by increase of the rigidity and the longitudinal elastic module (Young's module) of tendons27,104.
Subclinical inflammation is one important etiological factor in sarcopenia. Resistance exercise reduces the chronic status of inflammation in elderly people by decreasing the level of pro-inflammatory mediators produced by monocytes/macrophages, increasing the production of anti-inflammatory cytokines or reducing the inflammatory response to acute exercise. Furthermore, resistance exercise also reduces the expression of genes encoding proteolytic proteins and increases the expression of antioxidant enzymes30,39,50. Since the increase in fat mass and the reduction of the levels of sexual hormones is related to the increase of pro-inflammatory cytokines11, the reduction of the amount of fat mass and infiltrated muscle fat by the practice of resistance exercise is other of the mechanisms by which exercise would reduce the chronic inflammatory status in elderly population showing sarcopenic obesity.
Apoptosis is other of the mechanisms involved in the development of muscle fibre loss during sarcopenia in the elderly. A session of acute exercise induces the apoptosis machinery in some of the muscle fibres. Moreover, this apoptosis is also a stimulus for the reparation machinery in muscle. For this reason, acute exercise also stimulates the process of muscle regeneration. When it is practiced regularly, exercise induces important and beneficial adaptations in apoptotic pathways such as a lower activity in caspases, lower amounts of proapoptotic proteins, increase of the expression of anti-apoptotic genes and increase in the levels of anti-apoptotic markers26,54. Caloric restriction plays an important adjuvant role to the beneficial effects of exercise since it also contributes to the reduction of apoptosis in muscle fibers10,54.
Mitochondrial dysfunction found in aged people is due to the accumulation of oxidative damage in lipids, proteins and mitochondrial DNA. This dysfunction jeopardizes the production of energy in muscle fibres and reduces the physical capacity in old people35,42,43. The practice of both, resistance and aerobic exercise reduces these adverse effects of aging11,38,105-107.
Reparation and regeneration mechanisms degenerate as years accumulate27,31,39,41. One of the activation pathways in the regeneration of damaged muscle fibres depends on Insulin-like growth factor (IGF). The isoform I (IGF-I) promotes proliferation and differentiation of myoblasts and induces protein synthesis in muscle whereas the isoform II (IGF-II) promotes the differentiation of satellite cells. Then, IGF benefits muscle recovering by stimulating anabolism in muscle fibres and activating proliferation and differentiation of satellite cells27,31. In old people, muscle maintains the capacity to produce IGF-I, but shows resistance to its action. On the other hand, exercise increases the capacity to produce IGF-I, the synthesis of its receptors and the activity of the IGF-I-dependent pathways31,98,108-111. Eccentric exercises, that at the beginning induce a higher muscle damage in comparison with concentric contraction, increase levels of IGF-I mRNA in muscle98. Then, eccentric exercises will be especially indicated for the treatment of elderly people suffering sarcopenia. Other authors5 have related the increase in the sensibility to IGF-I and the decrease in the levels of homocystein produced by the practice of resistance exercise, with the prevention of cognitive decay induced by this type of exercise.
Since sarcopenia in the elder affects predominantly to type II fibres and training of muscle strength, through vibratory platforms, increase the number of these fibres, this kind of training would be recommended for the treatment and prevention of sarcopenia, specially because its security, efficacy and simplicity112-115. The physiological arguments of this methodology for training are based on the fact that the capacity of blunting of the vibratory stimulus depends on the viscoelastic properties of the individual. This means that this capacity depends on the stiffness produced by the structures of the organism and, in this case, this rigidity depends on the activation level of the receptors of the muscle use, the skin and joints or on the proportion of muscle type II fibres in the person. These factors are compromised in different degree in elderly people116,117. Other factors contributing to the increase of muscle stiffness are the incoordination agonist-antagonist118-121 and the increase in the rigidity of the tendons104. These data would reinforce the use of vibrating platforms with subjects suffering sarcopenia.
Neuromotor level
After the performance of strength training programs the increase found in muscle strength is higher than the increase in muscle mass. This fact highlights the importance of the neuromuscular adaptations induced by this type of exercise. These adaptations consist in better muscle innervations and improved muscle activation patterns11,17 by increases of muscle nervous stimuli from central nervous system, improvement of the synchronization122, changes in the commitment118 and increase in the maximum unloading rate in motor units35, decrease of the co-activation of antagonist muscles119-121, and increase in the expression of genes participating in the function and plasticity of synapse19.
Dynapenia, muscle weakness in the elderly, depends on alterations in muscle quantity, contractile quality and also neuronal activation. In this case, maintenance of the neuromuscular function through the practice of physical exercise seems to be essential for maintaining muscle strength and physical independence in old people123.
Molecular level
Since muscle wasting indicates a deregulation of the mechanisms involved in the maintenance of muscle fibres, a better understanding of the metabolic processes involved in the regulation of muscle mass is critical. This knowledge will permit us to design and develop more effective therapies to prevent this process124. Among the factors implicated in sarcopenia, the deregulation of muscle protein synthesis is one of the most frequently reported. Thus, the possible mechanisms to treat or prevent sarcopenia must include the regulation of the molecular factors that contribute to the balance between protein synthesis and breakdown125. One of the main signalling pathways controlling protein synthesis in skeletal muscle is depending on the kinase Akt/PKB. One of the main targets of Akt/PKB is the mammalian target of rapamycin (mTOR) kinase that has been recently shown as a key sensor of nutritional status and lifespan. In fact, animal studies have demonstrated that Akt/ mTOR-dependent pathway is downregulated in muscle during aging126. Furthermore, it has been demonstrated that this anabolic pathway show a delayed response to both, strength exercise and essential aminoacid treatment in aged in comparison with young people127. These effects can probably due to the oxidative modification of Akt by s-nitrosylation that contributes to a lower activity and then, regulation of downstream targets even with higher levels of Akt128. This delayed response is probably due to the insulin resistance that increases during aging since some experiments have demonstrated that supraphysiological doses of insulin can induce protein anabolism in muscle in aged people129. Since aerobic exercise have demonstrated its capacity to overcome insulin-resistance in muscle130, the combination of both, aerobic and strength exercise must increase the response of muscle and increase the activity of the Akt/mTOR dependent protein anabolism.
On the other hand, mitochondrial activity is other of the main factors involved in the maintenance of the activity of muscle fibres. Caloric restriction is one of the main therapies able to increase life-span and increase muscle capacity of the organisms tested during aging. This nutritional intervention prevents mitochondrial damage by improving the metabolic balance and avoiding oxidative stress131. Then, a balanced aerobic metabolism will prevent mitochondrial damage and probably will delay sarcopenia progression. Thus, prevention of mitochondrial damage could be one of the key mechanisms to delay or avoid sarcopenia. Recently, studies performed in mouse models for mitochondrial mutations have demonstrated that exercise prevents mitochondrial dysfunction and apoptosis in sarcopenia by increasing mitochondrial remodeling51,132,133, indicating the importance of functional mitochondria in muscle maintenance.
Biogenesis of mitochondria depends on multiple factors that converge in the activation of the peroxisome proliferator-activated receptor gamma coactivator-1 alpha (PGC-1-α)134. This factor is the centre of a system of gene induction that regulates the renovation of mitochondrial components and maintains mitochondria function. PGC-1-α itself is regulated by several factors including AMP-activated protein kinase (AMPK). AMPK is a key sensor of the metabolism and nutritional status of the cell135. Activity of AMPK is also negatively affected by aging contributing to the decrease of mitochondrial biogenesis and, then, sarcopenia. Furthermore, prevention of mitochondrial damage by increasing antioxidant activities has been recently shown to prevent age-associated mitochondrial function and improve insulin resistance136. This fact will permit to maintain a better oxidative metabolism at the same time that improves protein anabolism by increasing insulin sensibility. However, in old organisms, mitochondriogenesis induced by exercise seems to be limited137, although, some reports in humans indicate induction of this pathway at old ages138,139, probably by inducing the activity of sirtuins, key factors in longevity and mitochondrial metabolism134,140,141.
Finally, mitochondrial biogenesis must be balanced with the elimination of old and damaged mitochondria by mitophagy to maintain a balanced metabolism and avoid oxidative damage produced by higher release of reactive oxygen species (ROS). In this process, fork-head box (FOXO)-dependent mechanism must be taken into consideration. In muscle, FOXO3 regulates the expression of both, proteasome-dependent mechanisms of protein catabolism and auto-mitophagy. Both mechanisms are involved in muscle wasting142-144. On the other hand, activation of PGC-1-α expression in muscle inhibits FOXO-dependent protein degradation and prevents atrophy145,146. At the same time, exercise is able to increase both, protein synthesis machinery at the same time that induces proteasome-dependent activity indicating a mechanism of protein remodelling in muscle fibre147.
All these mechanisms are differently affected by the type of exercise performed, by quality of nutrients and amount of calories (fig. 2). Further, other hormonal effectors must be taken into consideration to understand the complex system involved in muscle physiology. It seems clear that intracellular signalling pathways are negatively affected by aging and that those mechanisms able to increase their activity during aging are important to avoid or, at least, delay sarcopenia.
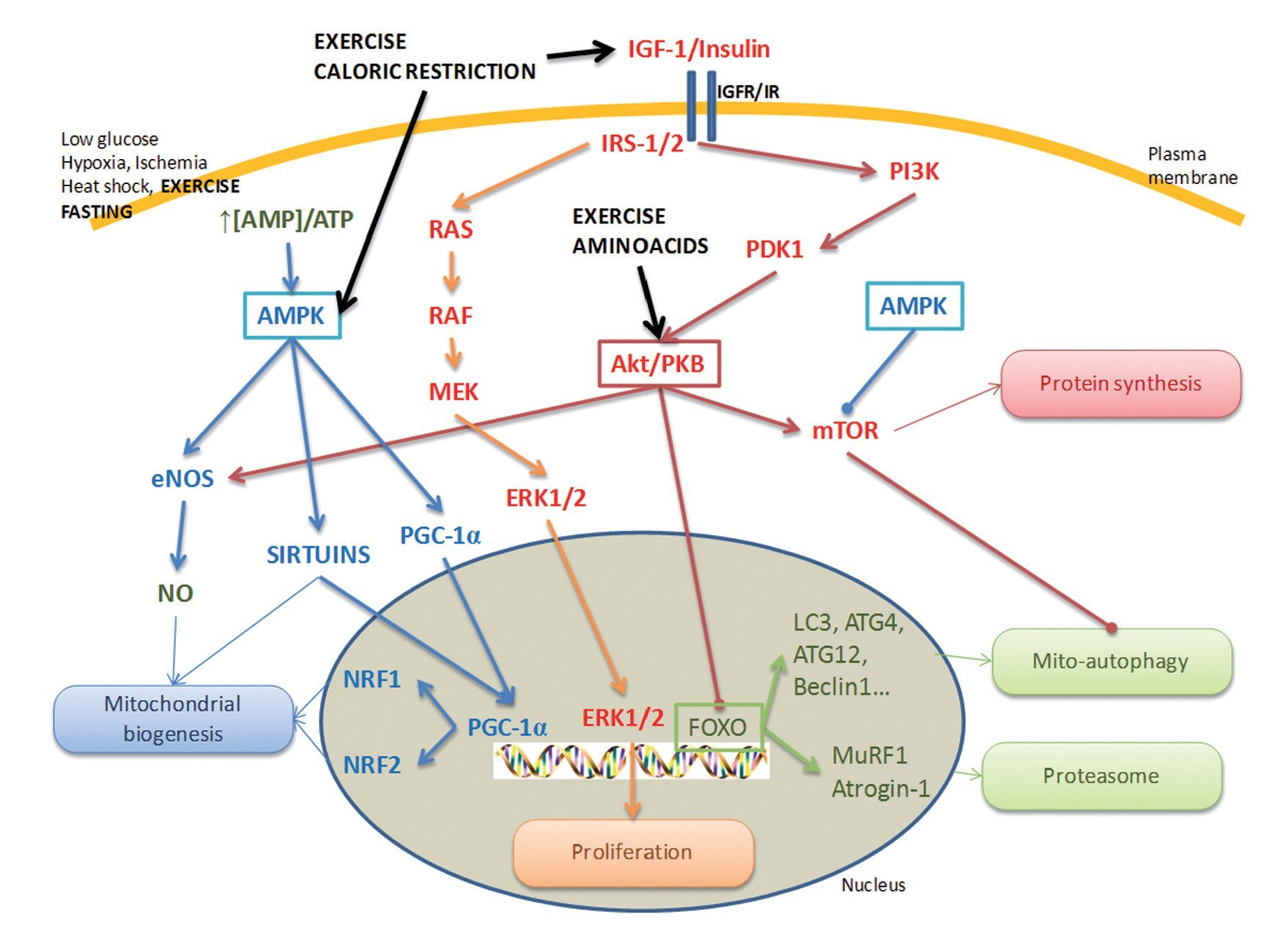
Fig. 2. Molecular mechanisms involved in sarcopenia. Basic representation of the molecular mechanisms involved in sarcopenia. Activity of AMPK, Akt/PKB and IGF-R-dependent mechanisms are reduced during aging. Practice of exercise, a low calorie diet and the intake of high quality aminoacids are able to induce the activity of the different components and stimulate protein synthesis and mitochondrial biogenesis. At the same time, Akt and AMPK also control mito-autophagy and proteasome activity. The knowledge of how these pathways are affected during aging and its effect on sarcopenia and the mechanism of action of exercise and diet on the activity of the main components of these pathways will permit us to develop therapeutical and pharmacological strategies to reduce sarcopenia during late ages.
Other mechanisms
Resistance mechanism improves the hormonal profile of old people specially affecting the levels of testosterone20,90,148, growth hormone11-13,26, estrogens78,92,149, IGF-I11,20,26,31,79,98,108-111 and insulin and improve the response to insulin20 preventing and improving by these means muscle capacity and, then, at least, reducing the progression of sarcopenia.
Conclusions
Resistance training, added to an adequate nutrition and aerobic exercise, is one of the main tools to prevent and treat sarcopenia in the elderly.
Correspondence:
J. de D. Beas-Jiménez.
Centro Andaluz de Medicina del Deporte. Consejería de Turismo, Comercio y Deporte de la Junta de Andalucía.
Glorieta Beatriz Manchón, s/n.
41092 Sevilla. Spain.
E-mail: juand.beas@juntadeandalucia.es
History of the article:
Received April 15, 2011
Accepted August 20, 2011
