



The effects of exercise protocols on postural control changes have been supported, but the influence of a common and specific type neuromuscular exercise such as plyometric on postural control is not clear. Therefore, the aim of this study was to examine the effects of plyometric type neuromuscular exercise on balance or postural control performance of young male volleyball players.
MethodTen professional young male volleyball players participated in this study and performed plyomeric exercises including 4×10 squat jump, broad jump, tuck jump with knee to chest, and depth jump from 45-cm box high 60 and 90s rest between sets and exercises, respectively. Before and immediately after completing the plyometric exercise, postural control was assessed by the Star Excursion Balance Test (SEBT) at 8 directions (anterior, A; anteromedial, AM; anterolateral, AL; medial, M; lateral, L; posterior, P; posteromedial, PM; and posterolateral, PL).
ResultsThe results indicated that plyometric exercise induced deficits in reach directions and greater changes occurred in the M, P and AL directions.
ConclusionsIt can be recommend that strength and conditioning professionals in the field of volleyball do not perform other type of landing exercise in plyometric training sessions because of postural control impaired and consequently the probability of lower extremity injuries will increase.
El efecto de protocolos de ejercicios, en cambios del control postural, son bien conocidos, pero la influencia de un sencillo y específico tipo de ejercicio neuromuscular, como los ejercicios pliométricos, en el control postural, no está clara. Por tanto, el objetivo de este estudio fue examinar los efectos de los ejercicios neuromusculares, de tipo pliométrico, en el equilibrio o en el control postural, de varones jóvenes jugadores de voleibol.
MétodoDiez varones jóvenes jugadores profesionales de voleibol participaron en este estudio y realizaron ejercicios pliométricos incluyendo 4×10 saltos con sentadilla, saltos de longitud, saltos con rodillas al pecho y saltos con rebote desde un cajón de 45cm de altura, con 60 y 90s de reposo entre series y ejercicios, respectivamente. Antes e inmediatamente después de completar los ejercicios pliométricos se midió el control postural mediante el Star Excursion Balance Test (SEBT) en 8 direcciones (anterior: A; anteromedial: AM; anterolateral: AL; medial: M; lateral: L; posterior: P; posteromedial: PM y posterolateral: PL).
ResultadosLos resultados indican que los ejercicios pliométricos indujeron déficits en las direcciones analizadas y que los mayores cambios se produjeron en las direcciones M, P y AL.
ConclusiónSe puede recomendar, a los profesionales del voleibol, en el campo del entrenamiento de la fuerza, que no realicen otros tipos de ejercicios de suelo en las sesiones de entrenamiento pliométrico, porque la disminución del control postural podría incrementar secundariamente la probabilidad de lesión del miembro inferior.
O efeito de protocolos de exercícios sobre as mudanças no controle postural ébem conhecido, mas a influência de um tipo de treinamento neuromuscular comum e específico como o pliométrico no controle postural não está claro. O objetivo deste estudo foi examinar os efeitos dos exercícios neuromusculares do tipo pliométrico no equilíbrio e controle postural de jovens jogadores de voleibol masculino.
MétodosDez jovens, jogadores profissionais de voleibol, participaram desse estudo e realizaram exercícios pliométricos que incluíram: 4×10 saltos partindo da posição de agachamento, saltos longitudinais, saltos com joelho encostando no peito e salto com rebote sob uma caixa de 40cm de altura, com descanso entre 60-90 segundos entre as séries e exercícios, respectivamente. Antes e imediatamente após completarem o exercício de pliometria, o controle postural foi medido com as 8 direções do Star Excursion Test (SEBT) (anterior: A; antero-medial; AM; antero-lateral: AL; medial: M; lateral: L; posterior: P; póstero-medial: PM e postero-lateral: PL).
ResultadosOs resultados indicam que os exercícios pliométricos induziram déficits no alcance das direções do SEBT e as maiores mudanças ocorrem nas direções M, P e AL.
ConclusãoPode ser recomendado que os profissionais que trabalham com força e condicionamento físico voltado ao voleibol não realizem outro tipo de exercício com carga nas sessões de pliometria, por causa da debilidade no controle postural que o treinamento pliométrico ocasiona e consequentemente na probabilidade de aumentar o risco de lesões nos membros inferiores.
Knee ligament injuries occur several times during training and competition in volleyball players. Among some ligaments in the knee, anterior cruciate ligament (ACL) plays a critical role to stability of the joint.1,2 ACL injuries account for 50% or more of all knee injuries, making this ligament especially important in any discussion of knee injuries. Most ACL injuries in volleyball players occur when a player lands awkwardly after jumping. Usually ACL tears are associated with a “pop” and immediate knee swelling. Previous authors reported that annual incidence of ACL injury is about 38000 cases in the United States.3
One possible explanation to increase ACL injury could be deficits in postural control. It has been well documented that poor postural control is associated with injury of the joint and therefore enhancing joint awareness and postural control could be a modality to decrease injuries.4
The common method of training for power-type athletes (i.e., volleyball players) is plyometric training. It has been reported that plyometric training is an effective training modality for improving joint awareness, balance and neuromuscular properties that used by strength and conditioning professional at pre- and in season of training schedule for athletes.5,6 Plyometric training is a form of training techniques which used by athletes in all types of sports to increase performance adaptations.7 Plyometrics consists of a rapid stretching of a muscle (eccentric action) immediately followed by a concentric or shortening action of the same muscle.7 The stored elastic energy within the muscle is used to produce more force than can be provided by a concentric action alone.7
Although, with review in literature, plyometric training could be an effective training method for enhancing balance and postural control in athletes,5,6 the acute effects of plyometric training on postural control are poorly understood. Deficits in postural control after several fatigue protocols (i.e., running and resistance exercise) has been supported by previous authors,8–14 but the influence of plyometric exercise on balance performance is not clear. To the authors’ knowledge, only Twist et al.15 examined the influence of 200 countermovement jump plyometric exercise on unilateral balance performance by using the Biodex Stabiliometer and found deficits at 24h post exercise. Since, plyometric training can be used in some sport teams (i.e., volleyball) and those athletes perform plyometric training for increasing muscle explosiveness, determining the acute effects of plyometric exercise on balance and postural control is vital.
Compared with previous study that used Biodex Stabiliometer to analyze balance changes after plyometric exercise,15 Gribble et al.16 reported that Star Excursion Balance Test (SEBT) should be considered a highly representative, noninstrumented dynamic balance test for physically active individual. The SEBT has been shown to be a reliable measure and has validity as a dynamic balance test to predict risk of lower extremity injury, to identify dynamic balance deficits in patients with a variety of lower extremity conditions, and to be responsive to training programmes in both healthy people and people with injuries to the lower extremity and this note have been confirmed by clinicians and researchers that employed the SEBT for the lower extremity functional test.
With regard to importance of plyometric training on athletes training schedule and highly representative of SEBT to determine the deficits in postural control, no study has focused on the analysis of a specific plyometric exercise programme on postural control performance in volleyball players. Therefore, the aim of this study was to examine the effects of plyometric type neuromuscular exercise on postural control (SEBT) in volleyball players. It was hypothesized that a session of plyometric exercise would impair postural control performance and would induce reduction of joint awareness in volleyball players.
MethodsParticipantsTen national level young male volleyball players (age 19±1.5 years, height 181.6±12.7cm, weight 69.5±10.8kg and training age 4.1±0.7 years) volunteered for the study. Athletes were free from lower extremity injury for at least 6 months prior to testing, have no history of hip, knee or ankle surgery and participated in a minimum of 2h volleyball training four times a week. All athletes signed an informed consent form and the study was approved by the University Research and Ethics Committee.
DesignAthletes reported to the laboratory at 4:00 PM. On entering the laboratory, height (cm), body mass (kg), and training age (year) were measured in each subject. Body mass was obtained to the nearest 0.1kg using an electronic scale (Tanita, BC-418MA, Tokyo, Japan). Height was measured to the nearest 0.1cm using a stadiometer (Seca 222, Terre Haute, IN). The athletes were familiarized with the testing and plyometric exercise protocols in this session. Each player was instructed and verbally encouraged to give a maximal effort during all plyometric exercises and testing. A standardized warm-up, consisting of jogging, dynamic stretching, and then a series of increasing intensity sprints, was performed before initiation of study. Before and after plyometric treatment, each volleyball player performed SEBT to determine postural control changes.
Postural control assessmentIn this study the Star Excursion Balance Test (SEBT) was used for the postural control assessment because Gribble et al.16 reported highly representative, noninstrumented dynamic balance test to assess postural control. The SEBT was performed as described by Robinson and Gribble.17 Participants stood in the middle of a grid laid on the floor with 8 lines extending at 45° angles from the centre of the grid, each of which is labelled according to the direction of excursion in relation to the standing leg: anterior (A), anteromedial (AM), medial (M), posteromedial (PM), posterior (P), posterolateral (PL), and lateral (L) anterolateral (AL). Participants undertook the testing barefoot, with foot position controlled by aligning the heel with the centre of the grid and great toe with the anteriorly projected line. Participants were asked to maintain a single-leg stance on the test leg whilst reaching the opposite leg to touch as far as possible along the chosen line with the most distal part of their foot. The foot was only allowed to touch lightly so as not to aid balance. The athlete then returned to bilateral stance. The point at which the subject touched was marked by the examiner and measured manually using a measuring tape. The same investigator measured all participants, and marks were erased after each trial.
For a trial to be successful the participants hands had to remain on their hips, the reach leg could not provide support upon touching down, the heel of the stance leg had to remain in its position in the centre of the grid and not lift from the ground and balance had to be maintained. Each athlete performed six trials in each direction for familiarization of testing and then performed three reaching trials with one leg before switching to the other leg with 30s recovery allowed between them. The best score in between three trials was chosen for further analysis. This approach allowed for the effect of repeated trials to be examined to determine whether a learning effect was present and decreases the fatigue induced by direction trials.
Normalizing SEBT dataAthlete's legs were measured from the anterior superior iliac spine to the distal tip of the medial malleolus using a standard tape measure while participants lay supine. Leg length was used to normalize excursion distances by dividing the distance reached by leg length then multiplying by 100.18
TreatmentVolleyball players performed squat jump, broad jump, tuck jump with knee to chest, and depth jump from 45-cm box high four sets with ten repetitions, respectively. There were 60 and 90s rest between sets and exercises, respectively. This type and repetition of plyometric intervention is common in volleyball players.7 The athletes were instructed to perform each jump with maximal effort and minimal contract on land. All exercises were supervised by strength and conditioning specialist and author.
Statistical analysisDescriptive statistics [mean±standard deviation (SD)] for the SEBT values were calculated. To determine the effect of plyometric intervention on postural control changes a two times (pre and post) for eight directions (A, AM, M, PM, P, PL, L, AL), ANOVA was applied. When a significant F value was achieved, Tukey post hoc procedures were performed to locate the pairwise differences between the means. The effect sizes (ESs) were calculated using Cohen's d. The level of significance was set at p≤0.05.
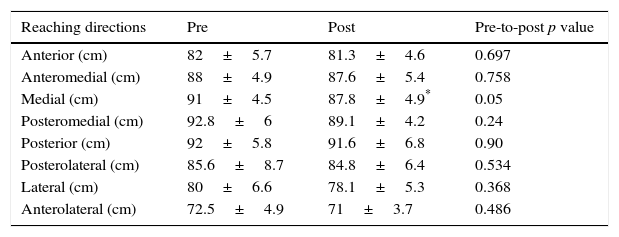
ResultsThe results of this study indicated that a session of plyomeric exercise induced significant decrease in reaching direction for the M (p=0.05); however changes in other reaching directions were no statistically significant (p>0.05) (Table 1). With comparing the % of changes in between directions, there were significant differences between them. The greater changes were observed in the M, P and AL directions and these differences were maintained compared with AM and PM, respectively (p≤0.05). Fig. 1 shows differences in % of change and ES in between reaching directions.
Pre to post changes in postural control performance. Values are mean±standard deviation.
| Reaching directions | Pre | Post | Pre-to-post p value |
|---|---|---|---|
| Anterior (cm) | 82±5.7 | 81.3±4.6 | 0.697 |
| Anteromedial (cm) | 88±4.9 | 87.6±5.4 | 0.758 |
| Medial (cm) | 91±4.5 | 87.8±4.9* | 0.05 |
| Posteromedial (cm) | 92.8±6 | 89.1±4.2 | 0.24 |
| Posterior (cm) | 92±5.8 | 91.6±6.8 | 0.90 |
| Posterolateral (cm) | 85.6±8.7 | 84.8±6.4 | 0.534 |
| Lateral (cm) | 80±6.6 | 78.1±5.3 | 0.368 |
| Anterolateral (cm) | 72.5±4.9 | 71±3.7 | 0.486 |
 and effect size in reaching directions for the volleyball players. A; anterior, AM; anteromedial, AL; anterolateral, M; medial, L; lateral, P; posterior, PM; posteromedial, PL; posterolateral. *Significant differences compared with AM direction (p≤0.05). †Significant differences compared with PM direction (p≤0.05).")
Plyometric effect (%) and effect size in reaching directions for the volleyball players. A; anterior, AM; anteromedial, AL; anterolateral, M; medial, L; lateral, P; posterior, PM; posteromedial, PL; posterolateral. *Significant differences compared with AM direction (p≤0.05). †Significant differences compared with PM direction (p≤0.05).
The aim of this study was to examine the influence of a session of plyometric type neuromuscular exercise on postural control changes which assessed by SEBT. The results indicated that plyometric intervention induced deficits in balance. The impairments in postural control were greater in M, P and AL directions in volleyball players. In accordance with these findings, some studies reported impairments of postural control after different exercises. For example, Crowell et al.8 investigated postural stability after exercise protocol including squat jumps, sprints, and treadmill running in male and female club-sport athletes. Differences between baseline and post exercise balance were observed, leading to the conclusion that any decrease in performance on the postural control might be attributed to the fatigue that had occurred in the lower extremity. Similarly, Wilkins et al.9 examined the effects of a 20min exercise, including a 5min moderate jog, 3min of sprints, 2min of push-ups, 2min of sit-ups, 3min of step-ups, 3min of sprints, and a 2-min run on balance performance in NCAA Division I collegiate athletes. Total errors increased from pretest to posttest in the exercise group. It appears that a contribution of both central (i.e., changes in force perception by the brain) and peripheral mechanisms (i.e., disruption to extrafusal and intramuscular fibres) might play a role in exacerbating balance performance. Several studies have alluded to the possibility that muscle spindles and Golgi tendon organs become desensitized as a result of fatiguing19 or eccentric exercise.20,21 Therefore, given the significance of these intramuscular receptors in controlling joint movement and position, it is plausible that the plyometric exercise could have potentially led to changes in afferent receptor activity, which resulted in reduction of balance performance.
It seems that the main reason for decreasing balance performance becomes plyometric-induced muscle fatigue. Due to the fact the muscular fatigue decreases the neural transmission velocity,22 maybe the ability in creating efficient compensatory contractions around the joint is reduced, resulting in a loss of the neuromuscular control and decreases in reaching directions. But no physiological and neural assessments were made and this is only a speculative statement. In the literature, the negative effects of fatigue protocols (i.e., cycle ergometer, aerobic and anaerobic exercise) on postural control deficits have been supported.8,9 Indeed, several studies have demonstrated that muscle fatigue can impair joint proprioception.10–13 It has been suggested that impaired proprioception can delay stabilizing muscle activation, leading to decrements in postural control.14
In this study, muscle fatigue could not be separated because of the plyometric exercises involved hip, knee and ankle muscles and the effects of each muscle groups on balance performance could not determine. However, there were available data about the local muscle fatigue and postural control deficits. Gribble and Hertel23 reported that fatigue at the knee caused greater postural sway than fatigue at the ankle during unipedal stance. Bellew and Fenter24 examined the effects of muscle fatigue at the ankle and knee on balance using three different clinical tests. Their results indicated that postural control, as measured using the lower-extremity reach test, decreased significantly only after knee fatigue, while postural control measured with the single-limb stance time test was significantly reduced only after ankle fatigue.
In the present study, it seems that knee fatigue occurred because the most jump and plyometrics which used in this protocol involved knee extensor muscles. The results have shown a deterioration in the reflection sensitivity after the fatigue, and they suggest that the modulation of the neural input to the muscle has at least partial reflective origin in the contracted muscles, and the decreasing muscular rigidity that followed the decreasing reflection sensitivity, and such lower rigidity may induce deficits in joint awareness and consequently decreases in reaching directions and postural control deficits.25 According to the results found in the present paper, the neuromuscular control is partially compromised with the fatigue onset, and this can be a predisposing factor to future injuries and it is better that strength and conditioning in the field of volleyball did not perform other type of landing exercise in plyometric training session and separate plyometric training with regular volleyball training to reduce probability of lower extremity injuries.
From a practical point of view, it must be considered that a session of plyometric exercise tends to decrease balance and postural control performance of volleyball players. The reduction in neuromuscular control (i.e., SEBT) was possibly attributed to a complex interaction of central and peripheral mechanisms, although this study was unable to distinguish the precise contribution of each and further studies are necessary for this subject. Overall, the findings have implications for coaches and athletes who should be conscious of the use of skill-based activities and for increased injury risk following plyometric training.
Conflicts of interestThe author has no conflicts of interest to declare.
