




Introduction
Nutrition plays an important role in the achievement of optimal performance in sports and is especially critical in resistance sports. The resistance sport of alpinism combines high physical exercise with hypoxia-induced anorexia, especially at altitudes above 6,000 metres. Studies have shown that the organism can oxidize fats and carbohydrates in a normal manner up to 5,000 metres, therefore any weight loss below this altitude can be attributed to inadequate calorie intake1-3. Weight loss above 5,000 metres appears inevitable due to the loss of appetite and nausea produced by altitude sickness and the metabolic changes required to obtain energy.
It has generally been accepted that the human diet should contain 55-65% carbohydrates, 12-20% proteins and 20-30% fats4, although the WHO recently increased the recommended proportion of carbohydrates to 75%5. However, some authors have supported increasing the protein intake at the expense of fats at high altitudes, with each component comprising 15-20% of the diet. They propose a daily intake of at least 7 g of carbohydrates per kg of weight (3.2 g per pound) plus 1.5-2.0 g of protein, with remaining calories consumed as fats6. Special caution should be taken with traditional fat-rich diets, which can lead to chronic muscle fatigue; they provide an inadequate amount of readily available carbohydrates, and diets rich in fatty acids require more oxygen during metabolism, slowing acclimatization. In a hypobaric chamber study7, in which altitude hypoxia was simulated by the gradual decompression of the chamber, subjects consumed ad libitum from a range of appetizing dishes but lost weight in proportion to the simulated altitude versus controls offered the same food under normal pressure conditions. Therefore, hypobaric hypoxia appears to be sufficient to produce weight loss, probably due to anorexia and poor intestinal absorption. These effects are increased in real expeditions8,9.
Oxygen saturation values of around 70% are essential for good absorption in the small intestine and avoidance of weight loss10-11. Roberts et al12 suggested that acclimatized individuals may have lower fat metabolism activity at high altitudes, influencing carbohydrate availability. On the other hand, McClelland et al13 concluded that the relative carbohydrate contribution does not change after altitude acclimatization and that the metabolic utilization of fuel is mainly influenced by the relative intensity of exercise, as at sea level.
There is little evidence that chronic or acute exposure to altitude increases the demand for any specific micronutrient, although there have been reports that iron and vitamin E supplements may be beneficial14. Studies of the effects of cold, energy expenditure, ultraviolet ray exposure and atmospheric composition indicate that supplementation with certain vitamins has a highly desirable antioxidant function in the high mountains15-18. At high altitudes, the prolonged consumption of vitamins with antioxidant properties can prevent the slowing of blood flow and the reduction in physical function associated with free-radical induced damage19,20. Dietary treatments that preserve or enhance the fluidity or deformability of the red blood cell membrane improve the transfer of oxygen to tissues, and action to improve oxygen delivery to tissues under hypoxia conditions is generally advantageous for the functioning of the organism. Exposure to hypoxia and peroxidation of unsaturated fatty acids of the red blood cell membrane reduce its deformability and its capacity to adapt to capillaries. Improved membrane fluidity (increased deformation capacity) can be achieved by two dietary mechanisms, for instance, diet supplementation with polyunsaturated fatty acids or antioxidants (for instance, vitamin E), in order to protect polyunsaturated fatty acids in membranes from peroxidation by free radicals.
Iron supplements can also be beneficial in this situation. According to observations of the response of erythropoiesis and haemoglobin synthesis at high altitudes, a normal iron intake appears adequate for males, whereas women may benefit from iron supplementation. The intake of oral iron supplements (ferrous sulphate, 200-300 mg/day) has been proposed during 2-3 weeks before a climb and during 2-4 weeks while at altitude, with the caveat that an increase in free radicals may be produced21-23.
In November and December 2002, seven climbers from Andalusia (Southern Spain) attempted the ascent of Jannu ("sleeping giant" in Nepalese), a Himalayan mountain of 7,710 meters in the Kangchenjonga region of Nepal.
The objective of the present study was to evaluate the diet of a group of high-mountain climbers at 4,500 metres, analyzing the types and amounts of nutrients.
Methods
Subjects
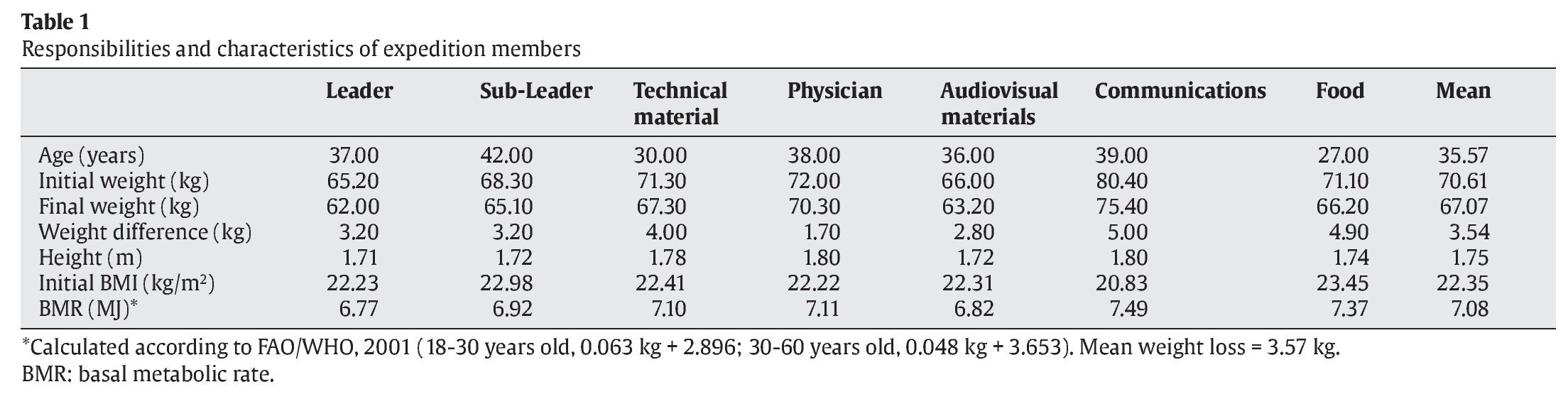
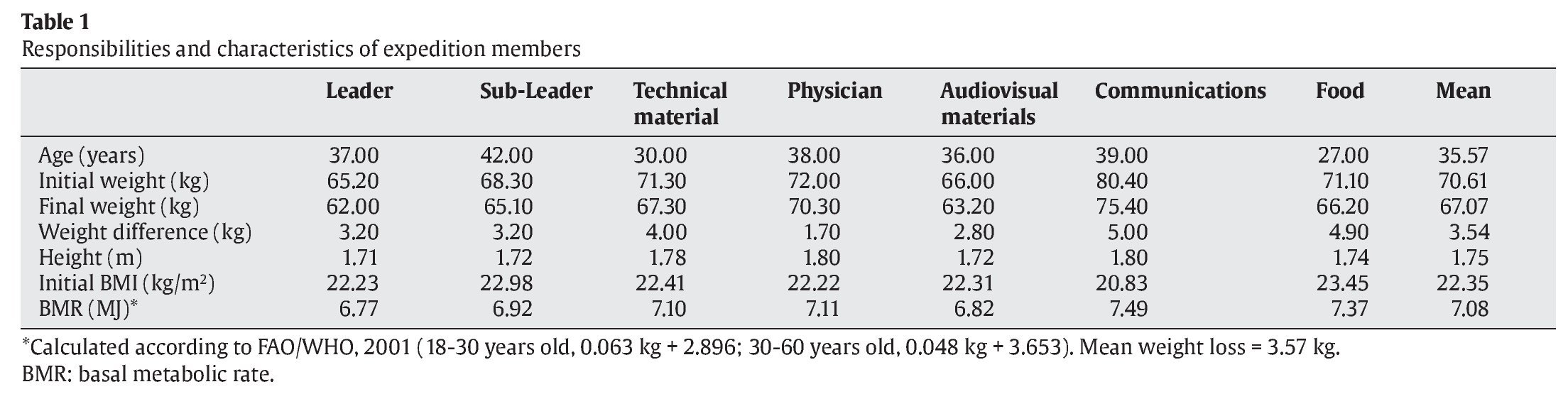
A study was undertaken of the diet followed by seven male climbers on the "Andalusia K2 2003" expedition; they were aged from 27 to 42 years and all had considerable mountaineering experience. Before acceptance as expedition member, each was informed both verbally and in writing of the full extent of the proposed research, and written informed consent was then obtained from each subject. All were in excellent physical condition prior to departure. Table 1 lists the responsibilities of expedition members and their anthropometrical parameters, calculated according to FAO/WHO24.
Procedure
The expedition comprised two phases: firstly ascent of Jannu in October, November, and December 2002; and secondly ascent of K2 (at 8,611 meters, the second highest mountain in the world) in June, July, and August 2003. The expedition was organized by the Andalusian Mountaineering Federation and subsidized by the Department of Tourism and Sports of the Andalusian Regional Government. The investigation was approved by the ethics committee of the University of Granada and all subject data were coded to maintain confidentiality.
Food and supplements
A register was pre-prepared for recording all data related to nutrition throughout the expedition. We recorded and analysed all of the food consumed at base camp during a 17-day period. Food items were brought from Katmandu and prepared by two Sherpa cooks.
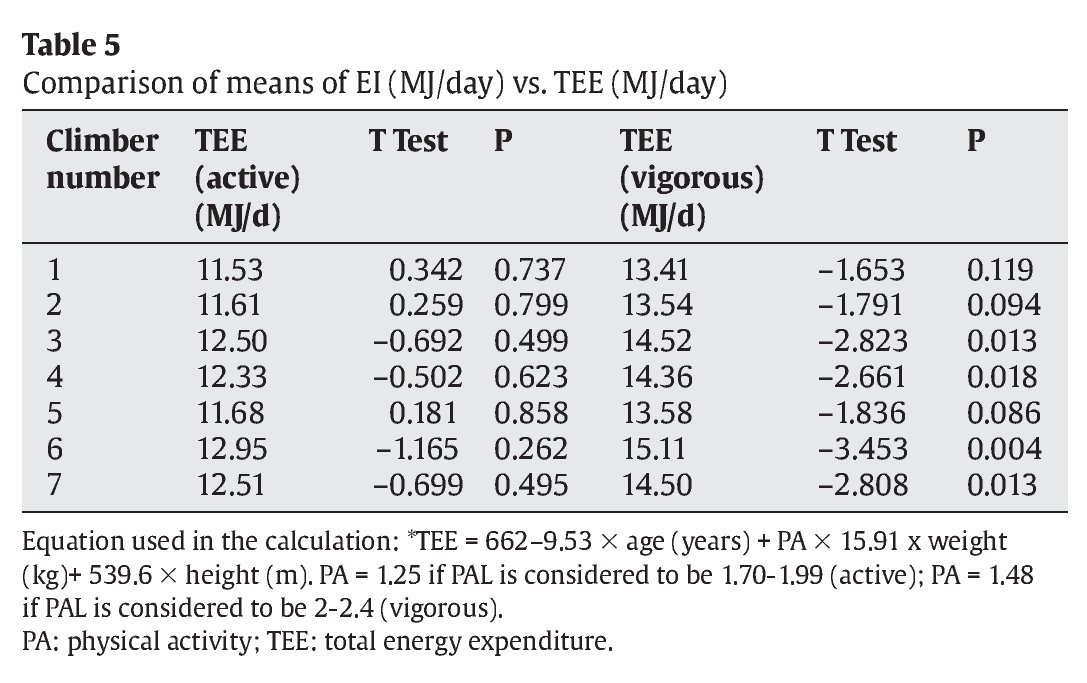
Four daily meals were prepared: breakfast, mid-morning snack, lunch, and evening meal. Varied menus were provided during the 17-day study period, prepared from both fresh and preserved foods. The amounts were calculated from the weight of the food items, measured by the climber responsible for food. They were weighed by means of a kitchen scale of 2 kg capacity with 20 g increments (Hanson UK Ltd. ref. 205 H, 700320363 Rev. 6.11). The same climber maintained the register, in which all foods purchased were noted and the food consumed on each day was recorded. The diet was analyzed by using the Dietsource software package25. When necessary, information on the composition of local foods (for instance, yak meat) was added to the database of this program, derived from the Food Composition Table for use in East Asia26. The energy intake (EI) was estimated from the daily menus. All mountaineers ate exactly the same meals and always ate all of the food offered, therefore the daily EI can be assumed to be identical for all study subjects. The estimated-EI value was related to the total energy expenditure (TEE) according to equations proposed by FAO/WHO24 (TEE = 662 - 9.53 x age (years) + PA x 15.91 x weight (kg)+ 539.6 x height (m), taking account of the basal metabolic rate (BMR) and physical activity level (PAL) of the group27. TEE values were calculated considering active PAL values (1.70-1.99) or, on climbing days, vigorous PAL values (2.00-2.40) PAL values.
Statistical analysis
Mean, minimum and maximum levels of nutrients in the menus were calculated, and the Student's t-test was used to compare nutritional data gathered during the 17 days of the expedition (estimated-EI) with nutrient intake recommendations (2005 Dietary Reference Intakes [DRI] data) for this population28. The normal distribution of nutrient values was checked and confirmed by using Kolmogorov-Smirnov and Shapiro-Wilke tests29,30. P < 0.05 was considered statistically significant. SPSS version 15.0 software was used for all data analyses.
Results
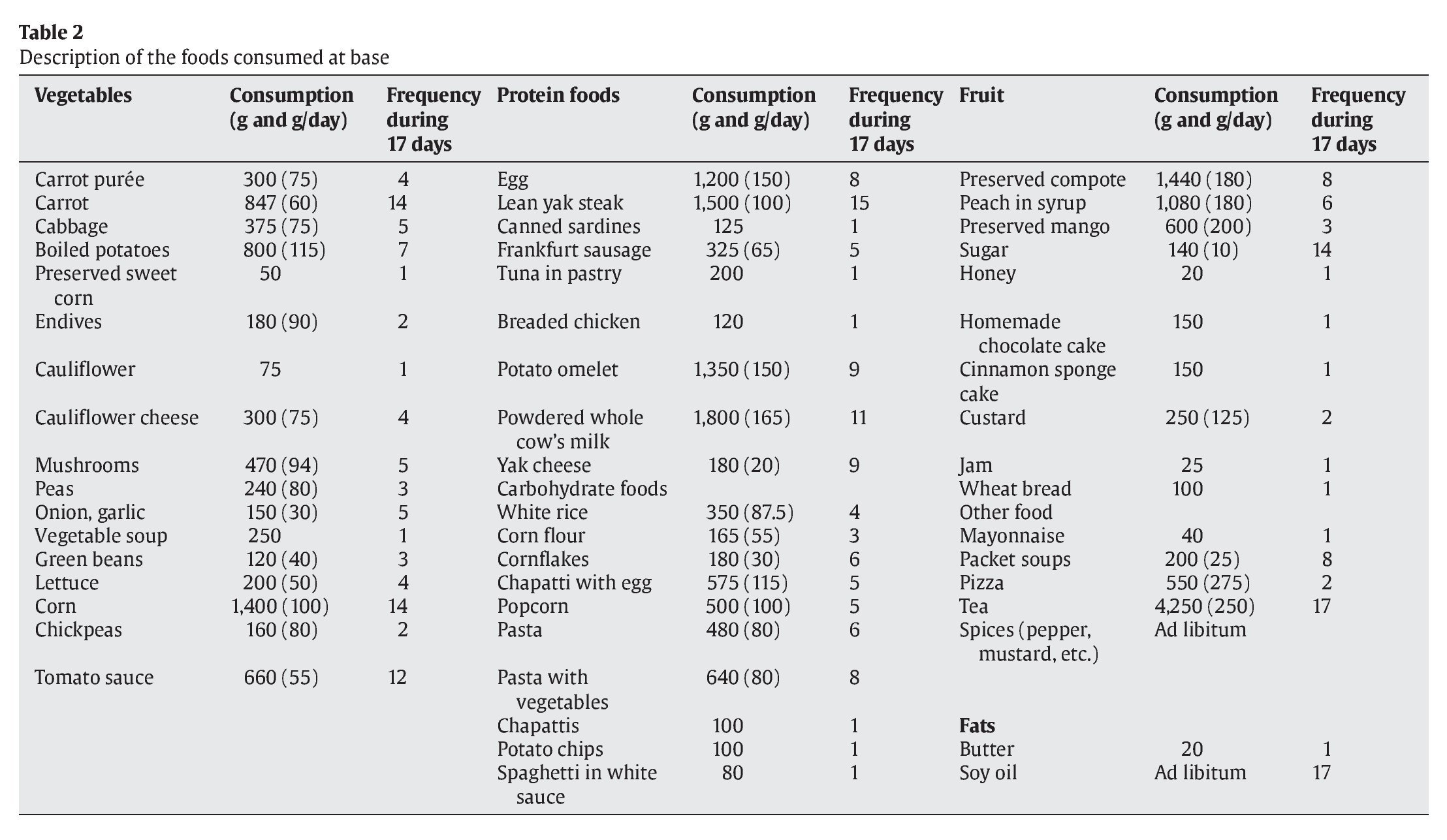
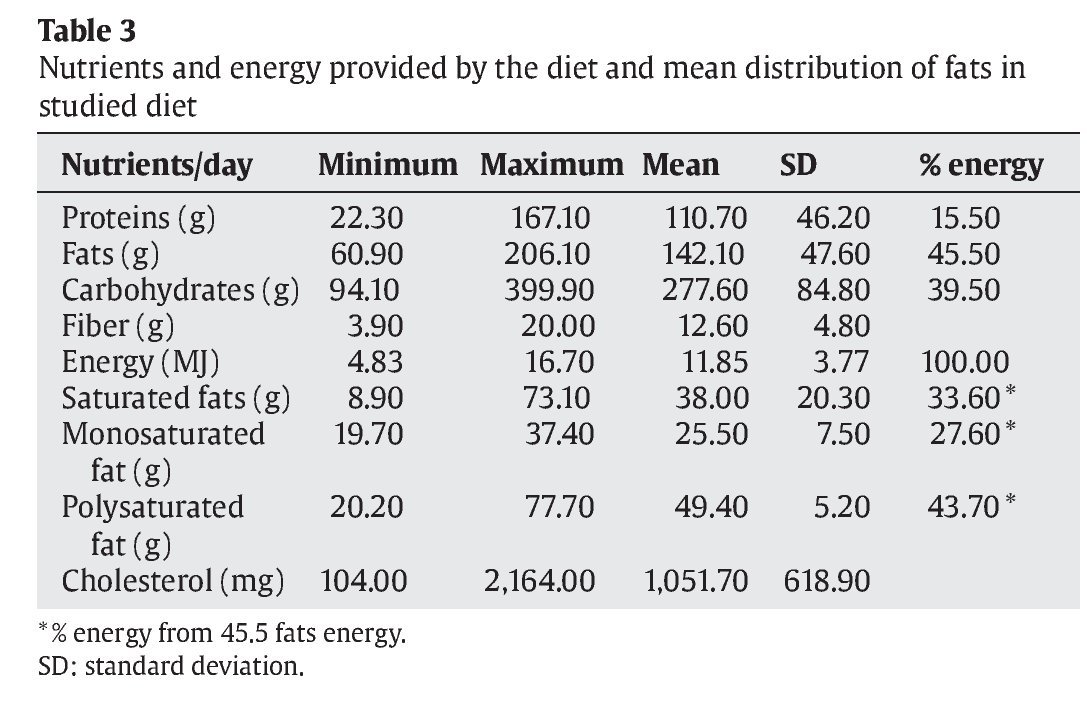
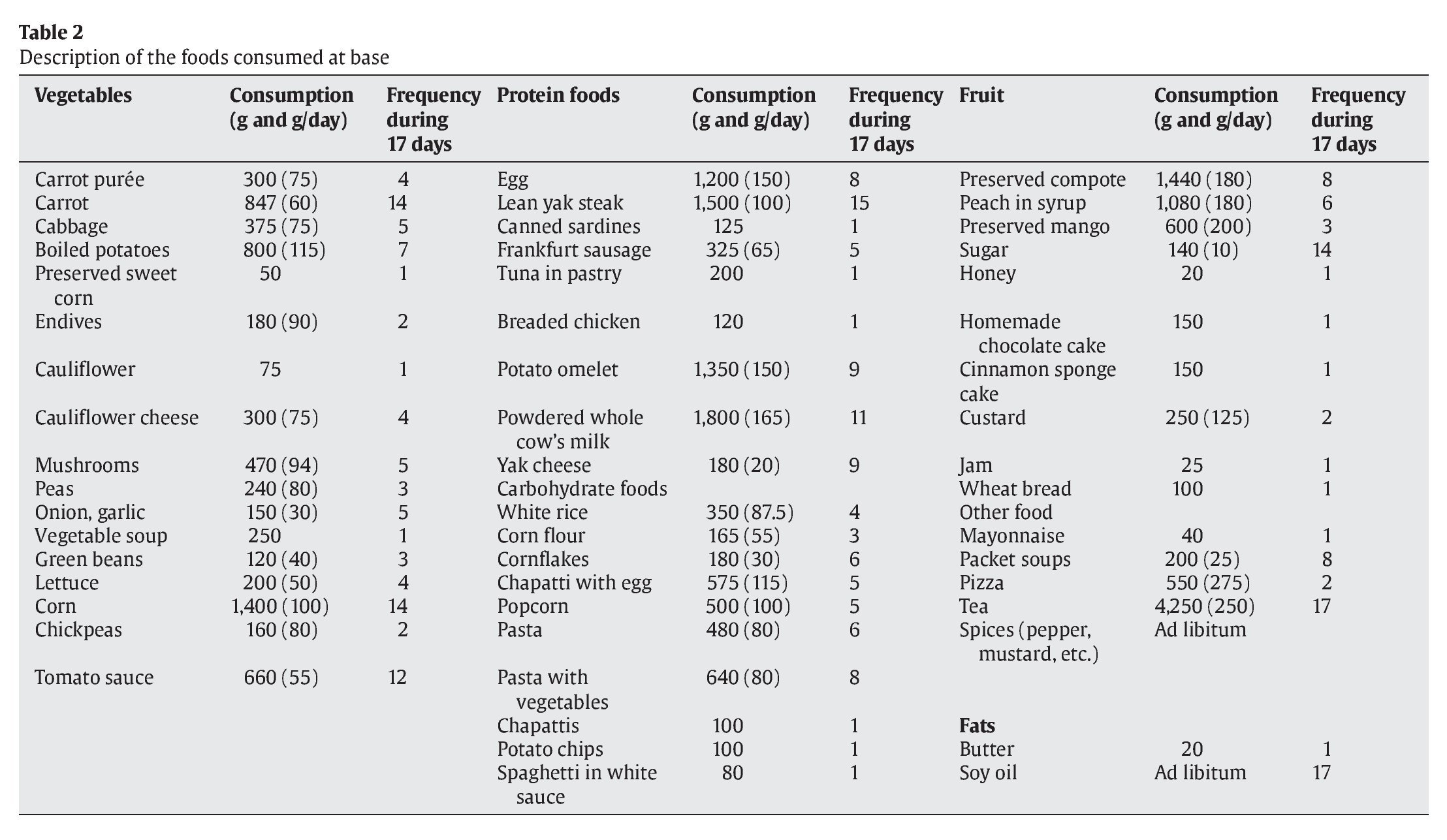
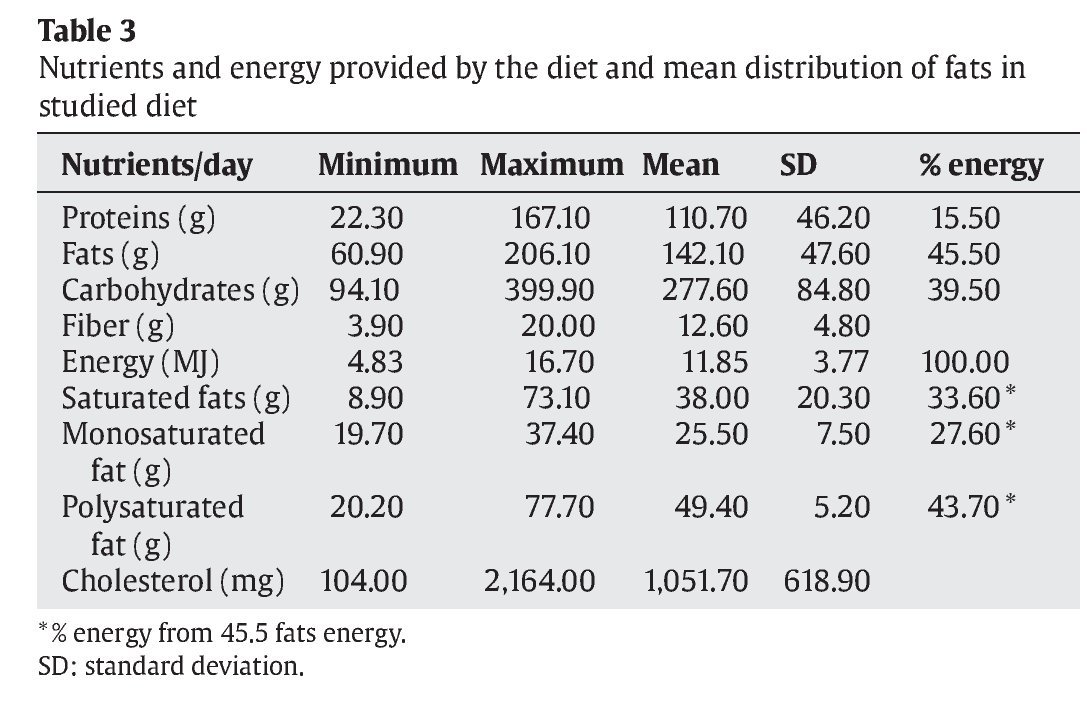
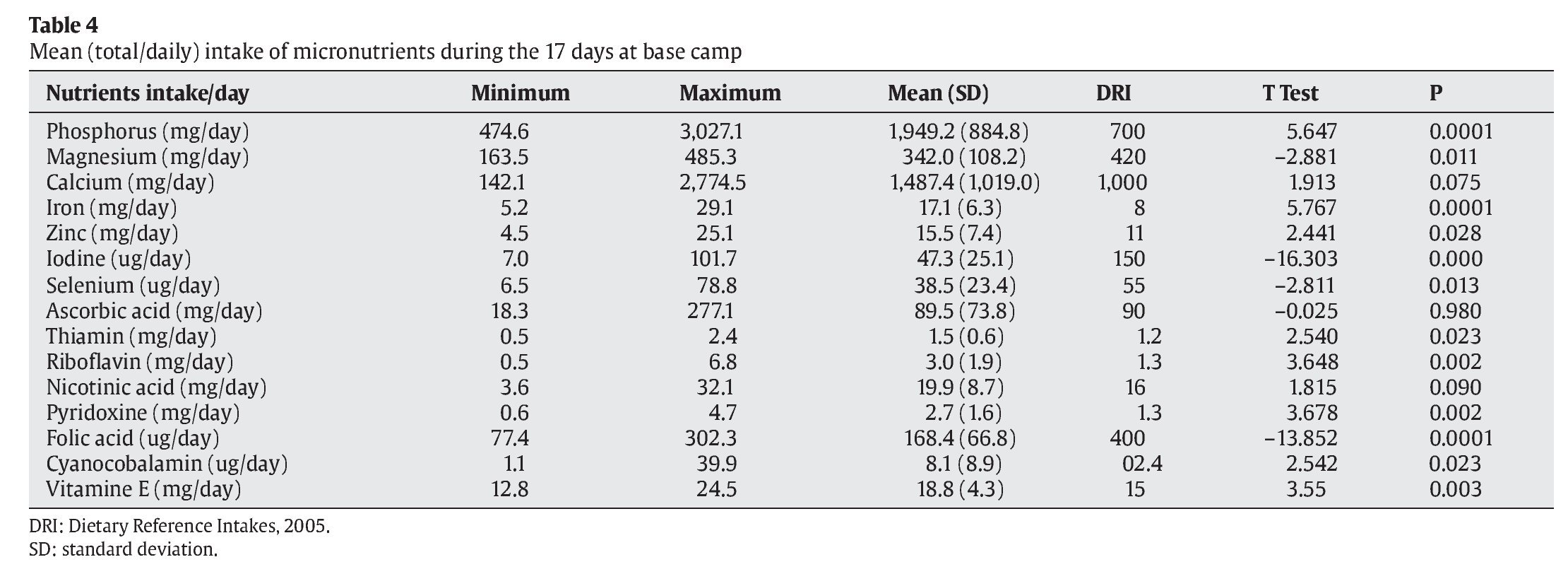
Table 2 lists food groups in the diet, amounts per person and frequency of their consumption. Tables 3 and 4 show results of the nutritional analysis of the meals consumed at the base camp during the 17-day study and the comparison (Student's t-test for one sample) with DRI values. Minimal estimated-EI (calculated from mean portions consumed by the group) and hence minimal estimated-EI/BMR ratios were observed on days 1 and 11 of the base camp stay. The mean estimated-EI/BMR (SD) of the group was 1.67 (0.53), ranging from 0.64 to 2.47. Table 5 shows the comparison between the TEE values calculated for each climber (according to weight, age and physical activity) and their estimated-EI values (see table 5 footnotes). When active PAL values were considered, no differences between mean estimated-EI and TEE values were found, but when vigorous PAL values were assumed, significant differences (P < 0.05) were found for five of the climbers.
Climbers were weighed at the start and end of the entire 2-month expedition, finding weight losses ranging from 2 to 5 kg (table 1).
Discussion
On a high-mountain climb, 15.90-25.10 MJ (3,800-6,000 kcal) are expended daily according to the type of physical activity involved11. It is evidently important to consume the amount of calories required by the organism. Climbers lose at least 3% of their body weight after eight days at 4,300 meters and 15% after three months at 5,300-8,000 meters31. This loss can produce a reduction in mental and physical functioning. Some studies have suggested that the intake of carbohydrates at altitude improves blood oxygenation and provides a more efficient energy source compared with fats or protein2. The macronutrient and energy levels observed in the present climbers differed widely from the usual recommendations for climbs above 6,000 meters. Nevertheless, no significant differences were found between the mean estimated-EI values estimated from the diet (11.85 MJ/day [2,832.5 kcal/day]) and the TEE values calculated for each climber according to 2001 FAO/WHO recommendations24 for adults with moderate activity. When the TEE was calculated for adults engaged in vigorous activity (PAL = 2.00-2.40), however, a significant difference with the estimated-EI value was found for five climbers. It should be borne in mind that this level of activity cannot be maintained during long time periods.
Among the 17 acclimatization days studied, estimated-EI/BMR values of > 2.00 were recorded on the only 7 days when they were climbing, an intake of at least 8.37 MJ/day (2,000 kcal/day) is recommended during long-duration activities to avoid iron or calcium deficits, depletion of glycogen deposits and dehydration31. Since these climbers were at 4,500 m and the aim of their base camp stay was to replenish energy deposits, their mean intake of 11.85 MJ/day (2,833 kcal/day) provided an inadequate supply of energy and micronutrients. These observations are similar to those reported by most studies, either in hypobaric chamber or in situ3.
The production of energy per litre of oxygen is higher when carbohydrates are the energy source, regardless of the oxygen pressure of inhaled air. Carbohydrates are also a more efficient energy source for working under conditions of reduced oxygen pressure32. The 39.5% carbohydrate intake of the present study group was very low, since around 55-65% is usually recommended to avoid muscle exhaustion from excessive depletion of glycogen reserves and to maintain adequate glycaemia against excessive protein catabolism. In short, a carbohydrate-rich diet favours acclimatization and the capacity for recovery4,31.
The climbers had a daily intake of 1.5-2.5 g of proteins per kg of bodyweight, very similar to the recommendations of most authors consulted (1.5-2.0 g/kg/day)33,34 and representing 12-15% of the total energy consumed35. Nevertheless, some authors have proposed a higher intake of 2.5-3 g/kg/day36. An adequate intake of proteins and glucose liquids is essential to prevent excessive weight loss under conditions of very high catabolism. Furthermore, prolonged exercise has a similar immunosuppressive effect to that of diets deficient in proteins and specific micronutrients37. Although no amino acid supplements were used in this expedition, some authors have proposed that valine, leucine and isoleucine supplementation prevents loss of muscle mass during acute hypobaric hypoxia38. In fact, the intake of these amino acids by the present climbers was similar to levels recommended for the general population. Supplementation with probiotics and glutamine appears to play a major role in immunofunction39. With regard to the origin of the protein, some studies have indicated that vegetable proteins produce a small reduction in free fatty acids40, which could be beneficial in diets that are very rich in fats.
In contrast to their carbohydrate content, the fat levels of the present diet were excessively elevated (45%). According to the American Dietetic Association and the American College of Sports Medicine31, fats should constitute at least 15% but not more than 20-25% of a diet. As mentioned above, fats are not the most efficient energy source under hypoxia conditions. The overconsumption of fats is a frequent observation, both among the general population and in different sports settings, for instance, swimming41.
Diets that are very rich in polyunsaturated fatty acids, especially linoleic acid, appear to reduce the absorption and utilization of iron, zinc and magnesium, reducing sports performance42. Nevertheless, some authors concluded that the role of linoleic acid remains unclear39. It should be taken into account that the present climbers underwent a drastic change in their diet. They all live in a Mediterranean region where fat consumption is largely in the form of olive oil, rich in monounsaturated fats (oleic acid), whereas the fats they consumed during the expedition were usually in the form of soy oil, rich in linoleic acid. Soy oil contains 45-60% linoleic acid, whereas olive oil contains 61-82% oleic acid, which presents greater resistance to auto-oxidation processes and the formation of free radicals43,44. If the climbers had used olive oil used instead of soy oil, their diet would have contained a much higher proportion of monounsaturated versus polyunsaturated fats.
The well-documented importance of iron, calcium, magnesium and vitamins D and C is even greater in situations of high oxidative stress, such as those produced in high mountains and by adaptation to high altitudes45,46. The increased excretion of iron, copper and manganese in intense and prolonged exercise was reported to produce a negative mineral balance42,47, although Fogelholm39 claimed neither the mineral nor vitamin balance is usually a problem for athletes, with the exception of iron and calcium in females. The supply of iron appears to have been adequate in the present study group (mean intake of 17.1 mg/day). Several authors have recommended that iron supplements may be taken up to two to three weeks before an expedition, maximizing iron levels, but once in the mountain they should only be supplied by the daily food intake, thereby avoiding the release of free radicals produced by iron supplements in hypoxia situations48,49. Excessive micronutrient supplementation (mainly vitamin C, B-group vitamins, and iron) during climbs has been contraindicated, since it does not improve sports performance and may have undesirable effects50. Nevertheless, vitamin C and general vitamin supplementation appears to be appropriate after exercise51,52.
The diet under study showed some interesting qualitative differences with the usual traditional Mediterranean diet53 of the climbers. It included novel foods such as yak products (meat, butter and cheese) and soy oil instead of olive oil, as mentioned above, and there was an absence or relative scarcity of fish, fruit, and vegetables (table 2).
The nutrient composition of the diet of these mountain climbers was not ideal. It was rich in saturated fats of animal origin and polyunsaturated fats from soy oil and was relatively poor in proteins and especially in carbohydrates, similar to the traditional diets of climbers. This type of nutrition does not favour acclimatization, because metabolism of the excessive fats requires greater supplies of oxygen at the expense of other tissues. An inadequate carbohydrate intake compromises effective muscle and liver recovery, produces a hyperglycaemia that increases protein catabolism, and accelerates weight loss54. The diet had a very low content of antioxidant vitamins, reducing the climbers' defences against free radicals and increasing the risk of damage to cell membranes. In conclusion, the diet of these climbers was not appropriate under these conditions. The lessons drawn from this study will serve to improve the nutritional intake of this team of alpinists during future expeditions.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Acknowledgements
The authors wish to thank Richard Davies for his assistance with the English version. This study was supported by the Junta de Andalucía, Spain (Research Group AGR-255 "Nutrition, Diet and Risk Assessment") and a postdoctoral grant from the University of Granada, Spain.
Correspondence:
F. Olea-Serrano.
Nutrition and Food Science Department. University of Granada.
Campus de Cartuja s/n
18071 Granada. Spain.
E-mail:folea@ugr.es
History of the article:
Received April 5, 2010
Accepted July 2, 2010
