




Objetivo. Investigar los efectos agudos de la crioterapia en la expresión de la enzima creatina fosfoquinasa (CPK), lactato deshidrogenasa (LDH), percepción del dolor y fuerza muscular en los miembros superiores de competidores de jiu-jitsu.
Método. Diez luchadores altamente entrenados fueron sometidos a dos sesiones de competición simulada (4 × 7-minutos y 15 minutos de intervalo). Después del primer día, cinco atletas fueron elegidos para la inmersión en piscina con hielo (5 ± 1 °C) durante 19 minutos, los demás fueron asignados al grupo control.
Resultados. Para LDH se observó efecto de la condición (F1,18 = 7,91, P = 0,012; η2 = 0,31) con valores más bajos (P = 0,012) en la crioterapia en comparación con el control (crioterapia = 533,2 ± 55,4 y 671,2 ± 61,0, respectivamente para inicial y final; control = 528,5 ± 63,7 y 759,8 ± 85,7 UI/l; respectivamente para inicial y final). El delta del CPK fue significativamente distinto entre las condiciones (crioterapia = 138,0 ± 95,1 UI/l; t = -1,72; P = 0,119; control = 231,3 ± 135,8 UI/l; tamaño del efecto = 0,75). Para el dolor percibido también hubo efecto de la condición (F1,18 = 12,35, P = 0,003; η2 = 0,41) con valores más bajos (P = 0,003) en la crioterapia (2,4 ± 1,4 frente a 4,4 ± 1,8). La temperatura corporal posrecuperación fue más baja en grupo crioterapia (P = 0,005) que la obtenida después en el control (34,5 ± 1,9oC frente a 37,6 ± 1,3oC). Se encontró correlación significativa entre la percepción del dolor y las concentraciones de CPK (r = 0,314) y LDH (r = 0,546). Las concentraciones de CPK y LDH se correlacionaron negativamente con la fuerza dinámica (r = - 0,525).
Conclusión. La recuperación usando la inmersión después de la competición resulta de un menor daño muscular e hipoalgesia.
Objetive. The acute effects of cryotherapy on creatine phosphokinase (CPK) and lactate dehydrogenase (LDH) expression, perceived pain and upper limb muscle strength in jiu-jitsu competitors were investigated.
Method. Ten highly trained athletes underwent two simulated competition sessions composed by four 7-minute combats with a 15-minute interval between them. Athletes were randomly allocated to receive either cold water immersion (5 ± 1 °C for 19 minutes) or no intervention (control) after competition simulation in a crossover counterbalanced fashion.
Results. For LDH, there was an effect of condition (F1,18= 7.91, P = 0.012; η2 = 0.31), with lower values being found in cryotherapy as compared to control (criotherapy = 533.2 ± 55.4 and 671.2 ± 61.0 for pre- competition and post-recuperation, respectively; control = 528.5 ± 63.7 e 759.8 ± 85.7 UI/l for pre- competition and post-recuperation, respectively). Delta CPK differed significantly between conditions (criotherapy = 138.0 ± 95.1 UI/l; control = 231.3 ± 135.8 UI/l t = -1,72; P = 0,119; effect size = 0.75). For perceived pain there was also an effect of condition (F1,18 = 12.35, P = 0.003; η2 = 0.41), with lower values being found following cryotherapy (2.4 ± 1.4 versus 4.4 ± 1.8, P = 0.003). Pre-competition skin temperature was lower than that measured after recovery (34.5 ± 1.9 oC. versus 37.6 ± 1.3 oC, P = 0.0005). There were significant correlations between perceived pain and CPK (r = 0.314) and LDH (r = 0.546). The concentrations of CPK and LDH were negatively correlated with dynamic strength (r = - 0.525).
Conclusion. Recovery via cold water immersion after simulated competition resulted in less muscle damage and hypoalgesia compared to the control.
INTRODUCTION
The muscle damage caused by exercise is an important tool for measuring the intensity of training, and it also affects the recovery period. The creatine phosphokinase (CPK) and lactate dehydrogenase (LDH) enzymes, muscle soreness and performance measures, such as strength and power, are widely used as indirect markers of muscle damage after exercise1-3. Recovery time depends on the type of training, duration, intensity and familiarity of the athlete with the exercise being performed. High-intensity exercises are associated with high catabolism of substrates, hyperthermia, muscle damage, oxidative stress and central nervous system fatigue4. High-intensity intermittent effort reportedly has high mechanic and metabolic costs4, while eccentric exercise requires only elevated mechanical overload5. Recovery strategies must consider the approach and characteristics of stress associated with the applied exercise.
Recently, cryotherapy has been tested extensively in studies involving recovery after exercise in athletes, particularly in the form of cold water immersion2,6-7. Several physiological mechanisms that have been proposed to explain the effects of cryotherapy are related to the induction of vasoconstriction6, which can limit vascular permeability and, thus, the inflammatory process, thereby reducing muscle pain2,8. A meta-analysis conducted by Leeder el al.8 demonstrated that cryotherapy contributes to the recovery of muscle power, reduces the efflux of CPK and alleviates pain symptoms pain 24, 48, 72 and 96 h after exercising.
Recently, Santos et al.7 demonstrated that cryotherapy benefited jiujitsu athletes undergoing specific training sessions, as the cold water immersion attenuated the concentrations of the CPK and LDH enzymes, decreased perceived pain and reduced isometric strength endurance in tests performed under specific intervention conditions (i.e., cryotherapy versus control). Thus, athletes involved in competitive grappling combat sports, such as jiu-jitsu, in which there is a predominance of high-intensity efforts interspersed with brief periods of low and moderate intensity and a large number of competitions on sequential weekends, could benefit from cold water immersion as a recovery strategy, allowing a faster return to training. The fast recovery time is desirable for high performance athletes as they return to the training cycle immediately after the competitions9. Therefore, the aim of this study was to investigate the acute effects of cryotherapy on the blood concentration of CPK and LDH the enzymes, perceived pain, and endurance strength of the upper limbs of jiu-jitsu competitors after a simulated competition. The hypothesis of this study was that the ice intervention would minimize muscle damage, decrease perceived pain levels and led to better preservation of isometric resistance and dynamic strength.
METHOD
The present study used a crossover design with two simulated competitions spaced two days apart. There were four 7-min fights with 15-min intervals. All subjects were previously familiarized with the procedures being employed. This study was approved by local human research ethics committee (protocol CAAE-0330.0.107.000-12).
Sample
Ten highly trained males (age 23.3 ± 4.1 years; body weight, 70.0 ± 3.3 kg; height, 175.3 ± 2.0 cm; body fat, 14.1 ± 2.9 %; jiu-jitsu competition experience 5.4 ± 2.0 years) who were members of a team that competes in international contests volunteered to take part in the present study. The athletes were selected using the following criteria: a) at least three years of training experience, and b) participation in at least three competitions in the year preceding this study. Prior to participation, all athletes were informed about the procedures to be followed, potential risks and benefits; each participant provided signed informed consent. All athletes were in the final stage (30 days) of preparing for a state jiu-jitsu championship, trained 5-6 days each week in 90-minute sessions and did not undergo rapid body mass reductions during the week preceding the data collection.
Pretest procedures
Before the experimental phase, anthropometric measurements were conducted. Body mass was measured with a scale calibrated with a maximum capacity of 200-kg and 100-g precision (Soehnle®, São Paulo, SP, Brazil). Height was measured using a stadiometer coupled to the scale (accurate to 1 cm). Body composition was estimated indirectly by equations that used skinfold thickness (caliper Lange, MA, USA). Body density was estimated with the Thorland et al.10 equation for university wrestlers, and body fat (% BF) was estimated by the Brozek et al. equation11. The International Society for the Advancement of Kinanthropometry (ISAK)12 manual was used as a reference for the anthropometric measurements, which were performed by a single trained investigator and performed in the 24-hours preceding the experimental phase.
Data collection
The fighters were advised to avoid training or any strenuous physical activity 48 h before the experiment. On the first day, five athletes were randomly chosen to perform cryotherapy after competing, and the others remained lying down. The treatments were reversed in the second competition simulation. Immediately after the last fight, the athletes were immersed in cold water (5 ± 1°C) for 19 min (four 4-min immersion cycles with 1-min intervals). During this period, the fighters in the control remained lying down at passive rest at room temperature (26°C).
Muscle damage markers
The serum levels of CPK and LDH were used as muscle damage indicators. For this process, blood samples were drawn before the first fight (15 min), and immediately after recovery (cryotherapy or rest). We collected 2 ml of venous blood from the arm and deposited it in tubes containing gel coagulant (Vacuette®, Greiner Bio-one, Campinas, SP, Brazil). The blood remained at rest for 30-min at room temperature for coagulation. Then, the blood was centrifuged at 2500 rpm for 8 min to separate the serum. The biochemical determinations were performed using an automated analyzer (Vitros® 5.1, Ortho-Clinical Dianostics, Johnson & Johnson Company, Rochester, NY, USA) using dry chemistry methodology. The LDH was measured using the multi-point kinetic technique (reading range: 101-825 IU/l). CPK was determined by the rate of multiple points (reading range: 41-1154 IU/l). Blood collection was performed by a research assistant trained for this function.
Upper limb strength
Before the competition and after recovery, all fighters completed the kimono grip strength endurance test, as proposed by Franchini et al.13. The test consists of a static strength exercise and another dynamic test. Initially, the fighters held a kimono wrapped around a horizontal bar and remained with their elbow flexed for as long as possible. After a 15-min break, the dynamic test began. During this test, the athletes performed the maximum number of repetitions from a fully extended to a fully flexed elbow position, with the same grip position used in the previous test. Both tests were performed to fatigue. This tests showed good reproducibility (dynamic test, intraclass correlation coefficient = 0.99, limits of agreement = -2.9 to 2.3 repetitions; isometric, intraclass correlation coefficient = 0.97, limits of agreement = -6.9 to 2.4 s)14.
Perceived pain
Athletes indicated the perception of pain using the visual analogue scale of pain, which is characterized by a 10-cm horizontal scale in which 0 = no pain, 1 to 3 = low intensity pain, 4 to 6 = moderate pain, 7 to 9 = severe pain and 10 = unbearable pain intensity. This measurement was performed before the first fight, after the last fight, after recovery and after the kimono grip strength endurance test, according to the methodology described by Carvalho and Kovacs15.
Body temperature
As a complementary measure, the axillary epithelium temperature was measured three times: before (10 min) the simulated competition, immediately after and during recovery. A digital thermometer was used (G-Tech®, RI, USA) with amplitude measured between 32.0 and 43.9°C (0.2°C accuracy). For all measurements, the thermometer was attached to the right side of the body. Figure 1 shows a flow chart with the measured variables and their periods.
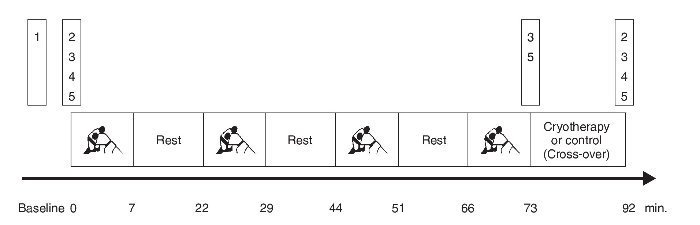
Fig. 1. Schematic representation of the data collection procedures. The numbers in the bars refer to the procedures used before, during and after the competition sessions. 1: anthropometry; 2: Judogi Handgrip Test; 3: body temperature; 4: blood collection; 5: scale of perceived pain.
Simulated competition
The simulated competition followed the rules of the International Brazilian Jiu-jitsu organization, except for submissions and the contest time. No fight was stopped before the preset time, even if there were submissions (e.g., arm lock or choke). This procedure was adopted to ensure the maximum physical effort and to maintain the same fighting times for all competitors in both conditions. Each fight lasted 7 min, in alignment with purple belt competitions. It is hoped that this procedure ensured greater validity for the practical application of the results obtained here. Moreover, the sample was composed of athletes with the following skill levels: two blue belt, four purple belt, two brown belt and two black belt. Therefore, fight time aligned with that of the greatest percentage of the sample. The fighters were divided into two fight contest groups: a) blue and purple, and b) brown and black. This competition format aimed to ensure that the participants faced opponents with equivalent technical levels, thus minimizing the bias associated with the level of effort.
Statistical analysis
Data normality was tested using the Kolmogorov-Smirnov test and Bartlett's homoscedasticity criterion. We adopted a two-way (treatment x time) analysis of variance (ANOVA) with repeated measures. For validation of the repeated measures, we used Mauchly's sphericity test, and the Greenhouse-Geisser correction was applied, as necessary. If a significant difference was observed in the ANOVA, the Bonferroni correction was used post-hoc. Cohen's d16 was used to estimate the magnitude of the effects of treatments across conditions. To compare the effects of CPK and LDH cryotherapy under controlled conditions, we calculated the deltas of these variables, which were compared with Student's t test for dependent samples. The magnitude of treatment effects calculated for CPK and LDH deltas was determined using the mean of the control minus the mean of the cryotherapy condition divided by the standard deviation of the two combined conditions (i.e., effect size = [mean control condition - average cryotherapy condition]/standard deviation of the two conditions combined). Pearson's correlation was used to verify the relationship between the adopted variables. All analyses were conducted by SPSS (version 16.0), and P < 0.05 indicated the level of significance.
RESULTS
Table 1 shows the values of CPK and LDH pre-competition and post-recovery under the two experimental conditions.

For CPK, there was an effect of time of measurement (F1,18 = 11.75, P = 0.003; η2 = 0.40), with lower values at pre compared to post-competition (P = 0.003). However, a significant difference was observed when the delta CPK was compared between conditions (t = -2.43, P = 0.038, effect size = 0.79), with lower values observed for cryotherapy (48.5 ± 146.5 IU/l) compared to the control condition (166.8 ± 134.1 IU/l). LDH was affected by condition (F1,18 = 7.91, P = 0.012, η2 = 0.31) and time (F1,18 = 49.60, P < 0.001, η2 = 0.73). Regarding the effect of condition, the values were lower (P = 0.012) for the cryotherapy condition versus the control. However, the delta concentration of LDH did not differ significantly between the conditions (t = -1.72, P = 0.119, effect size = 0.75). Additionally, the values measured before the competition were lower (P < 0.001) than the values measured after the competition.
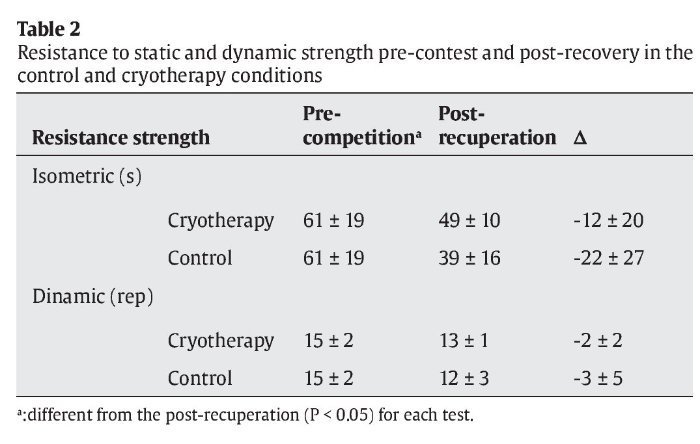
Table 2 shows the results for isometric and dynamic strength endurance performance.
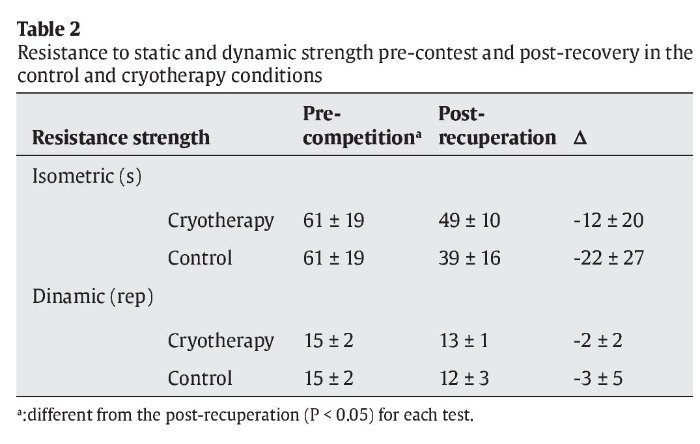
Only moment of measurement affected (F1,18 = 10.33, P = 0.005, η2 = 0.37) the isometric strength endurance performance, with higher values (P = 0.005) measured in pre-moment compared to post-moment. A similar result was observed for the dynamic strength endurance performance (i.e., there was no effect of moment; F1,18 = 9.46, P = 0.007, η2 = 0.35), with a greater number of repetitions (P = 0.007) at pre-moment compared to post-moment.
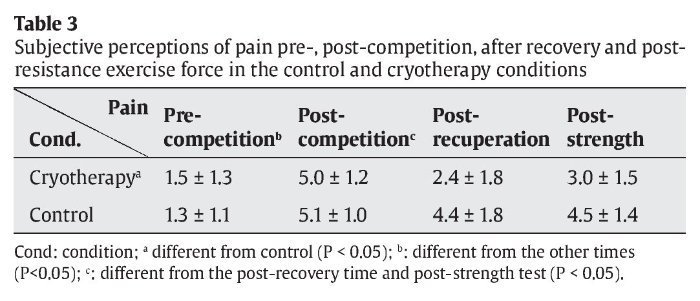
Table 3 shows the estimated perceived pain values.
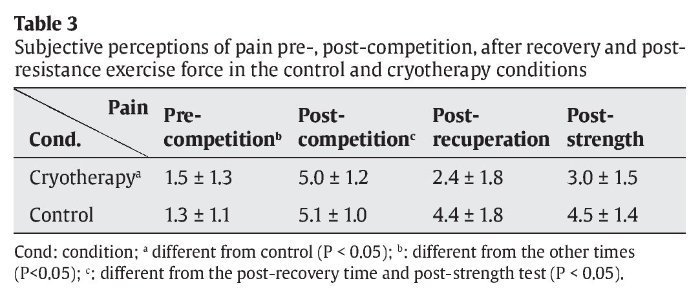
Perceived pain was affected by condition (F1,18 = 12.35, P = 0.003, η2 = 0.41) and moment (F3,54 = 19.46, P < 0.001, η2 = 0.52). The cryotherapy values were lower than those in the control condition (P = 0.003). Regarding the effect of the moment of measurement, the pre-competition values were lower than the values measured after the competition (P < 0.001), post-recovery (P = 0.001) and after the strength tests (P < 0.001). Additionally, the post-competition values were higher than those values measured after the recovery (P = 0.005) and post-strength tests (P = 0.028).
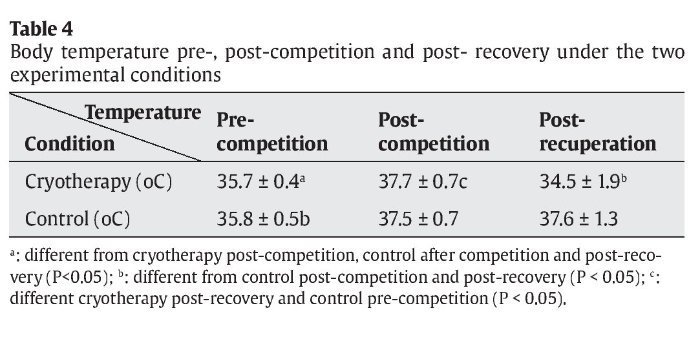
Table 4 shows the epithelium body temperature measurements at different moments.
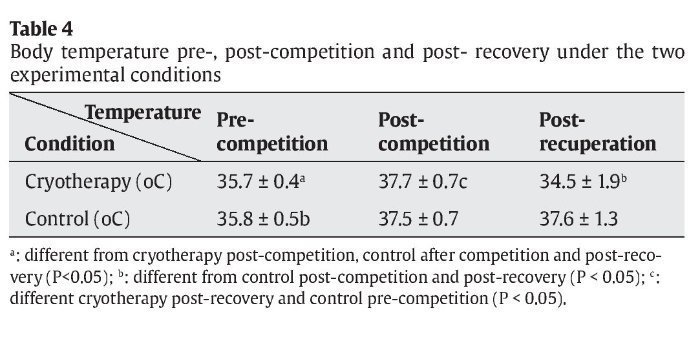
For temperature there were significant condition (F1,18 = 18.35, P < 0.001; η2 = 0.51), moment (F2,36 = 15.87, P < 0.001; η2 = 0.47) and interaction effects (F2,36 = 13.44, P < 0.001; η2 =.43). The pre-competition temperature in the cryotherapy condition was lower than that obtained after the competition in the same condition (P = 0.003), after the competition (P = 0.009), and after recovery (P = 0.005) in the control condition. The post-competition temperature in the cryotherapy condition was higher than that after recovery in the same condition (P < 0.001), but higher than that of the control condition during the pre-competition period (P = 0.008). In the control condition, the temperature during the post-recovery moment (P < 0.001) was lower than that of the cryotherapy condition after the competition (P < 0.001). Finally, during the pre-competition period, the temperature in the control condition was lower than that obtained after competition (P = 0.022) and after recovery (P = 0.012) in the same condition.
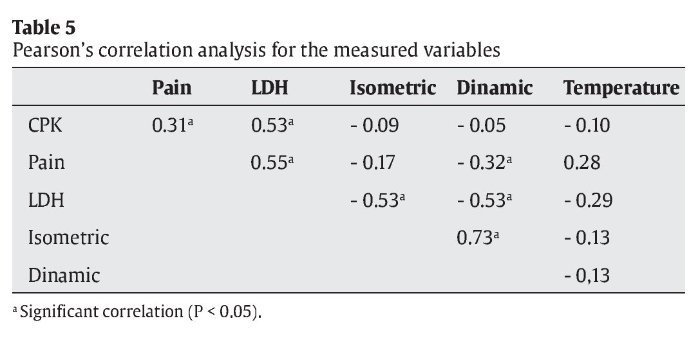
Table 5 presents the correlations between the different variables investigated.
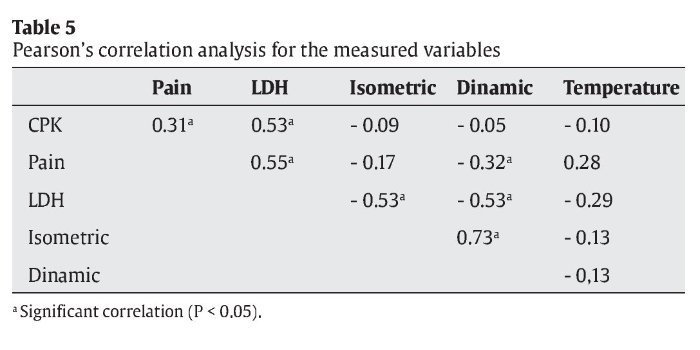
There was a moderate significant correlation between perceived pain and the concentrations of CPK and LDH and between the two enzymes (i.e., CPK and LDH). The LDH concentrations showed a moderate inverse correlation with performance in the endurance test evaluating static and dynamic strength. Additionally, there was a high correlation between the performances of both tests.
DISCUSSION
Recent studies have investigated strategies to assist the recovery of athletes after training sessions, games and competitions17-18. However, there have been no studies investigating cold water immersion after competition in combat sports. Recently, Santos et al7. found that cryotherapy reduced muscle damage in jiu-jitsu after 90 min of training. The results of current study indicated that jiu-jitsu competition resulted in increased concentrations of CPK and LDH, reduced performance on isometric and dynamic grip strength endurance tests, and increased perceived pain. Intervention with cryotherapy was effective in altering the temperature after the recovery period compared to the control. Lower levels of LDH were found in the cryotherapy condition compared to the control, although the delta increase of this enzyme did not differ between the conditions. However, the cryotherapy intervention resulted in a lower increase of CPK concentration and a lower perceived pain value compared to the control condition. However, even with the positive effects shown above, the performances on isometric and dynamic grip strength endurance tests did not differ between conditions. Shorter recovery course is desirable for competitors because they must often return to the training cycle immediately after the competitions19.
The increase observed in the markers of muscle damage is explained by the intensity of effort expended during fights jiu-jitsu20. Cryotherapy attenuated the release of LDH into the blood, which indicates lower impairment in the integrity of the skeletal muscle compared to passive rest (control). These findings were also found after a soccer match21. However, it is important to note that in our study, the delta of the concentration of LDH did not differ between the conditions.
Consistent with the results shown here, Banfi et al.22 observed a lower serum CPK in elite rugby players after cryotherapy compared to the active and passive recoveries. Similar results were observed in exposure to cold (-110°C for 2 min)23. In contrast, Hausswirth et al.2 observed that CPK levels did not differ from control after eccentric exercise. Note that the different methodological procedures, time of exposure to ice, water temperature and submerged part of the body all hinder comparisons between studies. Jakeman et al.24 investigated 18 physically active female volunteers who performed 10 sets of 10 repetitions of jumps with counter-movements; immediately after exercise, the women placed their lower limbs in cryotherapy 10°C. The authors observed an effect of time but no interaction between time and the treatment markers of muscle damage.
The time between the end of the competition and the dynamic grip strength endurance test was 34 min (19-min interval dedicated to the recovery and 15-min after the isometric test). However, this interval was not sufficient to restore the dynamic grip strength endurance. This result is contrary to that obtained in highly-trained judo athletes, in which it was observed that 15 min was enough for full recovery even after high-intensity intermittent stimuli.25-26. Thus, considering that both isometric and dynamic strength endurance are relevant to performance in jiu-jitsu competitions, where the final match is preceded by four fights, it is possible to infer the need for longer than 19-min and 34-min interval between the last and the final fight for the restoration of isometric and dynamic grip strength endurance, respectively, to allow for better physical performance of athletes. Future studies could be conducted to determine the minimum time required for recovery of these variables. In turn, Leeder et al.8 demonstrated that cryotherapy had no effect on the restoration of maximum strength but helped to maintain the levels of muscle power, although the authors did not present the possible mechanisms involved.
As observed in previous studies, the perception of pain was lower in cases of recovery using cryotherapy8,17. A similar result was observed by Poiton et al.27 in a study in which the application of ice packs (0.5oC for 20-min) decreased perceived pain after exercise. According to Gregson et al.6, a possible mechanism that explains this fact would be decreased osmotic pressure of the exudate (metabolites resulting from inflammation), which in turn result in lower neural signal signaling and pain stimuli propagation. Associated with this effect, the vasoconstriction tends to decrease the overflow of liquid, which in turn reduces muscle inflammation6. Strength endurance tests performed in the present study were meant to exhaustion and the discomfort is great in the final moments of the exercise. Thus, it was expected that a lower perception of pain would assist in the performance of isometric strength endurance test, which did not occur. After recovery, the cryotherapy condition has decreased the skin temperature close to 3°C in skin temperature when compared to the control condition. Having a body temperature of approximately 34°C peripheral vasoconstriction occurs28, which may have contributed to a decreased perception of pain.
In fact, cryotherapy results in lower rhabdomyolysis29, which is associated with greater perceived pain30. The results showed in this study indicated an association between the serum levels of CPK and LDH and perceived pain. Importantly, the enzyme levels that are indicative of muscle damage have been directly correlated with delayed onset muscle soreness8,31-32, but not immediately after exercise. However, cryotherapy also appears to influence acute pain. Ascensão et al.18 observed lower perceptions of acute pain (30-min after cryotherapy) and late onset (24 and 48-hours). Although there was an inverse correlation between serum LDH and the result of isometric and dyamic grip strength endurance tests, no studies were found that measured the strength of the association between these variables. However, when muscle strength and LDH were measured simultaneously, there were smaller force levels (-12 %) when the serum LDH levels were elevated (+163 % compared to baseline)33.
Although little attention has been given to combat sports, this study emphasizes the short-term metabolic benefits of cryotherapy after simulated competition jiu-jitsu. These findings are consistent with previous studies that have observed decreased muscle soreness after immersion with intermittent sprints34-35. Ingram et al.30 showed that after 80 min of exercise that simulated team sports, cryotherapy preserved more maximal voluntary contractions compared to a placebo or contrast therapy. This study indicates the need for further research regarding the application of cryotherapy in combat sports, and future studies should follow the late effects of immersion, because the concentrations of CPK and LDH exhibit peaks between 48 and 72 hours post-exercise36; other methods, such as massage therapy37, may also be used to improve the recovery of athletes.
It is concluded that the immersion after competition results in lower body temperature, hypoalgesia, lower serum LDH, and lower CPK elevation when compared to the control situation, although the performance in tasks involving isometric or dynamic grip strength endurance were not affected. This knowledge can be used by coaches who have athletes involved in competitive cycles with a high number of competitions.
Conflict of interest
The authors declare that they have no conflict of interest.
History of the article:
Received February 12, 2013
Accepted January 15, 2014
Correspondence:
C. J. Brito.
NEDES - Núcleo de Estudos em Desempenho Esportivo e Saúde.
Departamento de Educação Física. Universidade Federal de Sergipe.
Campus José Aloísio Campos - São Cristovão -Sergipe - Brasil CEP: 49100-000
E-mail: cirojbrito@gmail.com
