





To investigate the effects of cryotherapy on markers of muscle damage, as well as the perception of muscle soreness caused by eccentric exercise after downhill running.
MethodsTen participants (age=26±5year, height=173±8cm and body mass=70±4kg) performed two running trials on a treadmill tilted –6.6%, separated by one-week period. Cryotherapy (∼15°C for 30 minutes) was conducted after one of the trials of exercise. Blood samples were analyzed for markers of muscle damage (creatine kinase – CK; lactate dehydrogenase – LDH; calcium – [Ca2+]). Perception of muscle soreness was quantified using an analogical scale of pain. Data were collected before, 24 and 48h after the trials with and without the use of cryotherapy.
ResultsCryotherapy significantly reduced muscle soreness and was able to reestablish homeostasis in CK, LDH and [Ca2+].
ConclusionUse of cryotherapy after exercise with eccentric contractions was effective to reestablish the level of biochemical markers of muscle damage and reduce muscle soreness and pain perception in subjects submitted to downhill running.
Investigar los efectos de la crioterapia en los marcadores de daño muscular, así como la percepción de mialgia causada por ejercicio excéntrico tras carrera en bajada.
MétodoDiez participantes (edad=26,0±5,0 años, altura=173,0±8,0cm y masa corporal=70,5±4,0kg) realizaron dos ensayos de carrera en tapiz rodante con una inclinación de –6.6%, separados por un periodo de una semana. Se llevó a cabo una sesión de crioterapia (∼15°C,) tras cada uno de los ensayos. Se analizaron muestras de sangre para determinar los marcadores de daño muscular (creatín kinasa–CK; deshidrogenasa láctica–DHL; calcio - [Ca2+]). La percepción de dolor muscular fue cuantificada usando una escala analógica de dolor. Los datos se tomaron antes, 24h y 48h después de los ensayos con y sin el uso de crioterapia.
ResultadosLa crioterapia disminuyó significantemente el dolor muscular y fue capaz de reestablecer la homeostasis en CK, DHL y [Ca2+].
Conclusión: El uso de crioterapia tras ejercicio con contracciones excéntricas fue efectivo para reestablecer el nivel de los marcadores bioquímicos de daño muscular y reducir la mialgia y la percepción de dolor en sujetos sometidos a carrera en bajada.
O dano muscular é frequentemente observado em indivíduos envolvidos em atividades físicas que envolvam contrações excêntricas. Nestas situações, a crioterapia é utilizada para reduzir o dano muscular e a sensação de dor. No entanto, poucos estudos investigaram o efeito da imersão em agua gelada em marcadores de dano muscular, bem como a percepção de dor após exercício excêntrico.
MétodoDez homens (26,0±5,0 anos de idade, 173,0±8,0cm de estatura, 70,5±4,0kg de massa corporal). Os voluntários completaram dois corridas (teste e controle) separadas por sete dias, em um percurso declinado (–6,6%) em esteira. Em uma das tentativas realizou-se imersão em água gelada (∼15°C, 30 minutos). O dano muscular foi estimado mediante os níveis sanguíneos de (creatina quinase–CK; lactato desidrogenase–LDH e cálcio–[Ca2+]). A percepção de dor muscular foi estimada usando uma escala analógica. Todas as medidas foram realizadas antes, 24 e 48 horas pós-exercício.
ResultadosA imersão em agua gelada diminuiu significativamente a dor muscular e auxiliou no reestabelecimento da homeostase da CH, LDH e Ca2+.
ConclusãoA imersão em agua gelada após exercício excêntrico foi efetiva em reestabelecer os níveis bioquímicos de marcadores musculares e diminuiu a percepcao de dor.
The physiological mechanism of the delayed onset muscle soreness (DOMS) after exercise is not well elucidated.1 The DOMS is more frequent and of greater magnitude after exercises with a predominance of eccentric contractions.1 Among the reasons for this association between DOMS and eccentric exercise is the fact that eccentric actions promote greater tension to the contractile apparatus with greater accumulation of metabolites and structural damage in tissues.1–3 The structural damage to the sarcolemma and Z lines of sarcomeres are often measured by markers such as creatine kinase (CK) and lactate dehydrogenase (LDH).4
DOMS is largely observed among sportsmen, and it may have deleterious effects on human performance.5 The performance degradation associated with DOMS results of mechanisms such as the loss of homeostasis of calcium (Ca2+)6 and local elevation of inflammatory substances like histamine, kinins and prostaglandins.7 These inflammatory substances stimulate pain receptors types III and IV.5,7,8 Thus, the effect of DOMS on performance rely on an increased sensitivity to touch changing characteristics of skin sensitivity, increased muscle stiffness and reduced range of motion.3,9
Several strategies have been used in order to speed up recovery after exercise reducing the period and magnitude of DOMS; some examples are laser therapy,10 massage,11 contrast (heat and cold immersion) and immersion cryotherapy;12 this last one is the most popular due to the low cost and easy use by sportsmen. The vasoconstriction of blood vessels, capillaries, and lymphatics supported by cryotherapy13 reduces the spread of fluid in the interstitial spaces, thereby minimizing inflammation, pain, edema, and muscular spasms.14–16
Although cryotherapy is applied to reduce the DOMS, changes in inflammatory markers show divergent outcomes.12,17 Ingram et al.,12 Bailey et al., 17 Eston and Peters15 reported no change in the concentration of CK after cryotherapy, while Rise et al. observed reduction in the concentration of CK, myoglobin and C-reactive protein after immersion in cold water. Part of the incongruence concerning these studies results from the variety of methods used, such as different water temperatures, immersion time, intensity and type of exercise performed.19
The influence of cryotherapy on DOMS is evaluated in real sports context,18 simulations,12,17,20,21 isokinetic dynamometry evaluations,15 after a series of maximum eccentric contractions,11,19,22 vertical jumps from a higher level24 and plyometrics.25
Regarding the use of running protocols, Hausswirth et al.20 compared the effects of the application of whole-body cryotherapy, infrared and passive recovery in a well-trained runners group on different grounds (flat, uphill and downhill). These authors concluded that whole-body cryotherapy promotes faster recovery in comparison to other methods. However, it is known that trained people in modalities that require predominant eccentric contractions are more resistant to the damage caused by these types of contractions,26 which leads us to question if the application of post-eccentric exercise cryotherapy could significantly affect damage markers and pain perception in physically active people. Nevertheless, few studies27 have sought a significant evaluation related to the effects of application of cryotherapy on markers of muscle damage and muscle soreness after downhill running in people considered to be physically active. As a result of the increasing number of street racing fans and the diversity of ground characteristics, studies with this perspective are necessary since the runners are exposed to situations of greater demand for eccentric contractions. Thus, the objective of this study was to investigate the effects of application of cryotherapy on markers of muscle damage, as well as the perception of muscle soreness caused predominantly by eccentric exercise after downhill running.
MethodSubjectsThis study included 10 male volunteer subjects, healthy and sedentary (26±5 years of age, 173±8cm height and 70±4kg body weight). This set of subjects is similar to the ones that underwent cryotherapy in other studies (Eston and Peters15n=8, Ascensão et al.18n=10, and Santos et al.28n=9). Subjects who have participated on this study were informed about the goals and methods of the study and subsequently signed a consent form in accordance with the local ethics committee. Subjects who reported musculoskeletal problems were excluded.
ProceduresThe subjects underwent two bouts of exercise with a predominance of eccentric action (PEA) with one week interval between bouts. In the end of one session, randomly, a treatment with cryotherapy was applied. The perception of pain and markers of muscle damage were measured immediately before, 24 and 48h after the PEA. The subjects were instructed to avoid intense exercise and maintain normal diet during the previous days to the testing. All tests were performed in the afternoon, with a room temperature of 24°C.
The PEA was performed on a treadmill, with a negative slope of 6.6%, similar to the one used by Malm et al.29 The protocol started with a five-minute warm up walk (with no slope) at 5km/h. After warming up, the treadmill was declined and subjects ran for 25min at 8km/h. After the PEA, the subjects walked for five min at 5km/h with no slope in order to calm down.
The application of cryotherapy was immediately performed after the end of one of the two sessions of PEA. Cryotherapy was applied through the immersion of the lower limbs into cold water (15±1°C)25 for 30min. During this period, the subjects remained standing and had both legs submerged up to the iliac crest height. A thermometer was used to check the temperature, which was regulated by the addition of ice throughout the session.
The perception of DOMS was assessed by a visual analog scale of pain from 0 to 10 points,18 in which zero indicates no pain and ten indicates severe pain. Initially the subjects indicated the general feeling of pain, and then reported the perception by muscle groups of the lower limbs, which are ankle dorsal and plantar flexors and knee flexors and extensors.
Samples of 10ml of venous blood were collected, centrifuged and analyzed by spectrophotometry before exercise, 24 and 48h after the application of cryotherapy. Blood tests allowed the analysis of the enzymes lactate dehydrogenase (LDH) and creatine kinase (CK) using commercial kits (Labtest Diagnóstica, Lagoa Santa, MG, Brazil). These enzymes are among those indicated for monitoring muscle injuries.4
Analysis of dataThe data were tested using Shapiro–Wilk for normality, followed by Mauchly's test of sphericity. In order to check the effect of cryotherapy and time after treatment, as well as their interactions, a linear mixed model of 2 factors (with and without cryotherapy; 0h, 24h or 48h) was used with Bonferroni adjustment for multiple comparisons. When there was cryotherapy effect, the comparisons were made employing Student's t test for paired samples; when there was effect on the different durations of the treatment, comparisons were made using the analysis of variance for repeated measurements – ANOVA. The significance level of 0.05 was used for all analysis using a commercial statistical package (SPSS version 13.0).
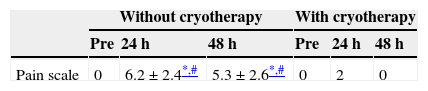
ResultsThe subjects reported no DOMS before starting the PEA protocols. The culmination of the induction protocol to DOMS without the subsequent application of cryotherapy caused DOMS in 70% of the subjects. The application of cryotherapy significantly reduced (p<0.05) values of DOMS compared to the situation without cryotherapy; no differences were observed concerning the previous situation (Table 1). In the situation without cryotherapy, DOMS increased significantly after 24 and 48h compared to the previous situation; the highest values occurred 24h after the PEA.
Reports of DOMS in different muscle groups showed a prevalence of the knee extensors of 71.4% opposite to the 57.1% of the knee flexors; and a predominance of the ankle dorsal flexors of 57.1%, opposite to the 28.5% of the ankle plantar flexors. The general DOMS reports indicated only the knee extensor muscles.
Regarding markers of muscle damage, the plasma concentration of CK in both situations was higher after 24h, but it was only a significant change in the situation without cryotherapy (Fig. 1). Plasma concentrations of LDH during the recovery period, regardless of the treatment, did not change significantly (Fig. 2). The concentrations of blood calcium [Ca2+] were significantly higher in the situation without cryotherapy when compared 0h and 48h (Fig. 3).
 in the pre-PEA (preconditions to the exercise with predominance of eccentric action, 0h), 24h and 48h after PEA conditions. * Indicates significant differences (p<0.05) for pre-PEA (0h) and 48h.")
 in the pre-PEA (preconditions to the exercise with predominance of eccentric action, 0h), 24 and 48h after exercise. There were no statistically significant differences.")
![Concentration of calcium [Ca2+] in the pre-PEA (preconditions to the exercise with predominance of eccentric action, 0h), 24h and 48h after exercise. * Indicates significant differences (p<0.05) compared to pre-PEA (0h).](https://static.elsevier.es/multimedia/18887546/0000000800000002/v2_201505010150/S1888754615000453/v2_201505010150/en/main.assets/gr3.jpeg?xkr=ue/ImdikoIMrsJoerZ+w997EogCnBdOOD93cPFbanNfAaByTQ/N8ihiO5/gXSp+QSmXRvECtoYOhQ5DvFt9tdI5SYv7oldxOVE+X58pKGvl752iHAa5cwlOp2I351QKtPRXfcj90+CFkbcKQ+mk9zIr8pfFrKXSMjMBCsnJHaxLt4CkOaKLdbtXheiM/5LqiekU+rB8rd3wSbR9PczaJcqR3ofYKV9rUuTTIU1VzEt6eaeBFLGR5YAGGrgvgXCcCObxINpfVa9uVrbf8tAP9k1OOofUh0BMdtrVaclqwT/g= "Concentration of calcium [Ca2+] in the pre-PEA (preconditions to the exercise with predominance of eccentric action, 0h), 24h and 48h after exercise. * Indicates significant differences (p<0.05) compared to pre-PEA (0h).")
This study has investigated the effects of cryotherapy on markers of damage and muscle soreness caused by exercise predominantly eccentric in downhill running. The results showed that the treatment with ice immediately after the PEA is able to reduce and minimize DOMS effects caused by muscle damage and that some mechanisms associated with inflammation appear to be the major determinants of DOMS in sedentary subjects.
The inflammatory process caused by damage to the muscle tissue increases the concentration of pro-inflammatory chemical mediators that stimulate pain receptors.5,7 Although the mechanisms are not yet fully elucidated, it is widely accepted that cryotherapy has an analgesic effect. The ice seems to decrease the ability of sensory transmission and thus reduces acetylcholine release influencing the pain threshold.19 Yet, according to these authors, another possible benefit of cryotherapy would be the change in hydrostatic pressure on the body, which could be associated with a reduction in edema and pain in the muscle.
When cryotherapy is used, the values found after 24 and 48h PEA did not differ from the preconditions. This demonstrates that the application of cryotherapy maintains homeostasis in CK levels after PEA. It is speculated that cryotherapy may reduce membrane permeability and thus reduce the flow of CK into the interstitium.15
However, the results found in the literature are not conclusive regarding the effects of cryotherapy on CK. The differences among the studies that concern the effectiveness of cryotherapy on DOMS depend on the type of exercise and immersion time. Ascensão et al.18 observed that, after a soccer match, players treated with cryotherapy (10°C) for 10min decreased the concentrations of CK after 24 and 48h compared to the control situation (35°C). Ingram et al.12 using the same temperature but with 2×5min immersions separated by 2.5min, reported no significant differences in the concentrations of CK in a group of 11 athletes. Goodall and Howatson24 induce DOMS through jumps on downhill and used cryotherapy (10°C) right after the exercise, 24 and 48h later. The results indicated higher concentration of CK after intervention with cryotherapy. According to some researchers, CK shows great variability among individuals, entailing considerable heterogeneity between subjects.30,31
After PEA downhill running, LDH showed no significant changes caused by cryotherapy. Although LDH is used to assess muscle damage,4 few studies have evaluated the effects of cryotherapy on its behavior. The effects of acute intervention (first hour) and subacute (24–168h) use of cryotherapy were analyzed and reported that LDH was not affected significantly by the application of cryotherapy, and that major changes were noticeable only 96h after the harmful stimulus.22 Vaile et al.23 who analyzed different hydrotherapy strategies for the recovery of muscle injuries, also reported no differences in the concentrations of LDH, even after 72h. In the present study the concentrations of LDH were checked 48h after the PEA, so we would expect that significant increases were not noticeable and/or cryotherapy does not cause many effects on this marker. This suggests that some blood markers can be used for evaluations of cryotherapy in acute post-exercise recovery, while others seem to be more sensitive to medium and long term changes.
Cryotherapy was effective in reducing the levels of calcium ion 48h after the PEA. This can be explained by the function of cryotherapy in reducing the plasma membrane permeability.15 The damage caused by PEA results in an increasing intracellular calcium concentration. It would be associated with the stimulation of the autogenic phase, increasing the action of proteases and phospholipases, with subsequent myofibrillar degradation – especially desmine and cell, thus triggering an inflammatory process.5 This increased pressure also causes tissue edema, which activate pain receptors thereby increasing the feeling of discomfort associated with DOMS.19 The ratio of intra- and extracellular calcium with the mechanism of skeletal muscle apoptosis can lead to reduction in muscle power, and the more releasing of inflammatory markers and DOMS, the more muscle undergoes apoptosis – thus reducing the number of myocytes chronically.32
Our main conclusion is that cryotherapy after exercise is a pertinent strategy to reduce DOMS and also markers of muscle damage for street racers who perform their training on slopes. Among the limitations of this study we can mention the small number of subjects, and the fact that improvements in the perception of pain reported by the subjects after treatment cannot be compared to a placebo situation.
Our results suggest that the use of cryotherapy by immersion for 30min at 15°C immediately after the practice of PEA reduces the DOMS of the lower limbs, while maintaining the homeostasis of some markers of muscle damage, such as CK and serum calcium.
Conflict of interestsThe authors agree that there is no conflict of interests about this study.
