



It is estimated that, by mid-21st century, one in five people will be above 65 and, thus, it will be the state’s responsibility to find formulas to improve its citizens’ quality of life. Physical exercise has frequently been presented as a useful means to induce bone mass gaining1-3 and, therefore, to prevent osteoporosis4-6. Osteoporosis and osteopenia are two of the greatest health problems that modern society faces, especially in a moment in which population is significantly increasing its life expectancy.
The continuous remodeling processes (formation and resorption) of bone structures are affected by many factors, among which, age, diet, metabolic disorders, hormonal imbalances, lactation, menopause or exercise are included as the most relevant7-11.
Tensions resulting from mechanical loads, as generated by physical exercise, are an important regulator of remodeling in some parts of the skeleton. The introduction of new technologies, applied to physical condition improvement in sportsmen, has lead to the development of new methodologies that, years later, have been transferred to other population sectors (sedentary, sick people or special populations). One of the most recent and popular innovations is the use of neuromuscular activation by means of vibrating mechanical stimuli12,13.
Whole body stimulation (Whole Body Vibration [WBV]) is, from all the different applications this technology (vibration systems applied to traditional weights machines, upper limb vibration, lower limb vibration or whole body vibration) allows, the one that has reached greatest popularity in recent years and the one generating the greatest body of knowledge. This technology generates controlled vibrations that, originating on the person’s foot sole, are transmitted to the caudal body area activating, in the neuromuscular system, what is known as Tonic Vibration Reflex (TVR)14-19. TVR’s response intensity depends on four factors: localization of the vibration application (on muscle or tendon), muscle’s initial length (the more stretched, the greater the response will be), CNS’s excitability state and/or vibrating stimulus parameters20.
The impact produced by the stimulus on the musculature depends on factors such as vibration frequency (Hz), displacement amplitude (mm), movement magnitude (m.s-1), direction (linear and/or rotational), exposure duration (min or sec), number of exposures, recovery time between each exposure (sec or min) and number of sessions21.
Recently, it has been proposed that this type of activity may result in a convenient and simple alternative to be used by a population suffering from problems in bone structure mineralization or that present with risk of fracture; in fact, WBV use is especially interesting when subjects have part of their motor autonomy compromised22-27. Some of the functional responses that would be affected by vibration would be related to calcium metabolism and to the hormonal response that regulates it. Parathormone (PTH), 1,25 dihydroxy-vitamin D (1,25(OH)2D3) and calcitonin are some of the compounds related to the osseous formation and resorption processes, offering us an idea on how bone construction mechanisms behave during the application of these exercises25.
PTH contributes to several physiological processes such as: maintaining calcium concentration in extracellular fluids within physiological limits28, controlling intracellular Ca2+ homeostasis29, regulating 1,25 (OH)2D3 formation by the liver30 or, by means of this other hormone, incrementing Ca2+ resorption and decrease phosphate excretion. Such facts make this hormone a key factor in the control of osseous construction. The process entails that when extracellular Ca2+ levels decrease (< 8 mg/dl) PTH release by the parathyroid cells is increased31.
While in the long run the hormone’s function is to favor osseous resorption mobilizing both calcium and phosphate, when there are high levels of calcemia (> 9.5 to 10 mg/dl), PTH’s function might be the opposite favoring bone construction32-35. The anabolic mechanism is linked to osteoblast-produced plasminogen36, with PTH reducing the activity of this protein’s inhibitor and favoring plasmin production, which, in turn, favors the synthesis of local growth factors (Insulin like Growth Factor [IGF-II] and possibly Transforming Growth Factor-β [TGFβ]). Such growth factors favor the release and proliferation of osteoblasts, responsible of initiating osseous production.
There is a relatively abundant literature on the acute response of PTH to physical exercise37-44, though none of the studies was performed using elderly subjects. From the studies, it is derived that both intensity and duration of exercise are determining factors to achieve an intense response of PTH to exercise, postulating the existence of a load threshold from which the aforementioned response is provoked43,45. On the contrary, the studies analyzing the short- and long-term responses of PTH to training loads are less numerous; however, in such case, the population was composed of elderly people. Among these, Zerath et al46 find a statistically significant increase in PTH levels after training without observing any changes in osteocalcin.
We hypothesize that a short term WBV training provokes an endocrine response in elderly subjects that results favorable to the osseous construction processes. Thus, the objective of the present study was to analyze, in elderly women, the response of PTH to mechanical vibration stimuli and to assess its effect on basal calcium and phosphate concentrations after a low- and very low- intensity short-term training.
MethodsSubjects Sixteen elderly females (age: 69.64 ± 4 years; height: 156.24 ± 4.42 cm; body mass index: 28.29 ±1.97 kg?m -1) participated in the study. The inclusion criteria were related to: age, health condition, and physical condition; it was decided to choose people with a medium level of physical activity, which was determined by means of a typical simplified questionnaire. In order to be included, subjects could not be taking any medication that could affect calcium metabolism, or hormonal reposition. Therefore, exclusion criteria were related to not meeting any of the abovementioned inclusion criteria and/or having missed more than one training sessions. None of the subjects had any previous experience in vibration platforms training. Subjects were asked to maintain their regular diet during the whole study period; this feature was controlled by means of alimentary records. All the participants gave written consent according to the Helsinki Declaration guidelines for research on humans. The sample was randomly divided into two groups: Experimental Group (EG), n = 8; and Control Group (CG), n = 8 (fig. 1). Sample size was estimated as described by Cohen 47 for ANOVA by using the PTH variable and data from pilot studies.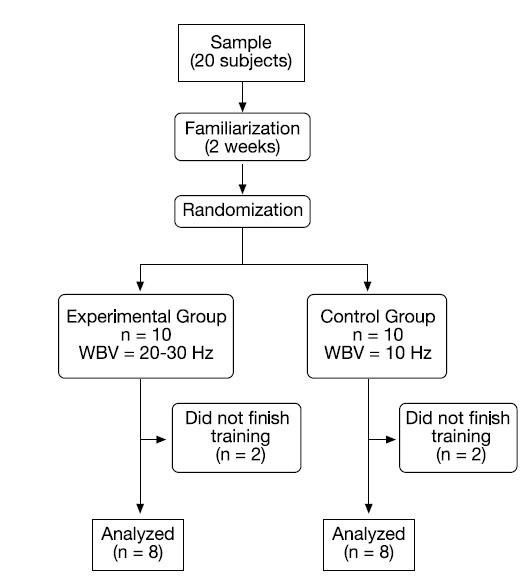
Fig. 1. Flow diagram of participants. WBV: whole body vibration.
MaterialsA vibration platform (NEMES, Ergotest, Rome, Italy) allowing work frequencies of 10-50 Hz, and vertical displacements of 4 mm was used. For the anthropometric assessment and for height, a skinfold calliper, and a stadiometer were used, respectively (Holtain Ltd., Dyfed, UK); for perimeter measurements and weight measurements, a metallic metric tape (Holtain Ltd., Dyfed, UK), and a commercial digital scale were employed, respectively.
Anthropometric measurements and 30-second chair stand testAnthropometric measurements were performed according to ISAAC’s instructions48, assessing weight, height, body mass index, skinfolds (triceps, subscapular, suprailiac, abdominal, upper-thigh, and mid-calf), and thigh and calf perimeters (to estimate muscle area).
In order to estimate lower limb muscular strength, the 30-sec chair stand test was performed as described by Rikli and Jones49; briefly, the test started with the subject sitting down with the back resting on the chair and feet on the floor. When the researcher indicated, the subject would stand up and go back to the initial position. The subject was encouraged to complete the highest possible number of repetitions in a 30 second-period. Before commencing the test, the researcher showed how to perform the exercise correctly, with the subjects practicing it one to three times in order to become familiar with the task, and starting the test immediately after.
ProcedureAll subjects participated from the familiarization period during which they learnt to correctly perform the exercises without the use of the vibration platform. In a second phase, the exercises were repeated on a vibration platform using a 10 Hz vibration.
For the experimental phase, subjects underwent 24 training sessions (3 days per week-1). Each session consisted of performing three exercises according to the protocol described in table 1:
1) Static standing position.
2) Dynamic squatting exercises.
3) Static squatting position.
Table 1 Whole body vibration (WBV) training sessions used for the experimental group (EG; n = 8) and the control group (CG; n = 8)
Briefly, the technical characteristics of the exercises were the following: a) static standing position: the hands should grip the platform handle in a relaxed way. The head had to be kept in the anatomical position, the legs in a 180° knee extension, and feet had to be resting on the metatarsus with a slight heel elevation; b) dynamic squatting exercise: with the hands on the handle, a flexion of the knee joint was performed, with a range of motion from 120 to 180°. The execution speed, four seconds for each repetition, was marked by means of a digital metronome; c) static squatting position: with the hands on the handle, a sustained flexion of the knee joint is performed at approximately 160-170°. For all exercises and sessions, the used work/recovery ratio was 1/1.
Previous to each session, a warm-up phase, consisting of articular mobility exercises and muscular groups’ activation exercises, was performed. At the end of the session, a series of static stretch exercises for plantar flexor, knee extensor and hip flexor muscles was performed.
Clinical assessmentBefore and after the training protocol, all subjects underwent a clinical analysis test (blood and urine) to determine the following biochemical parameters: PTH (Immulite 2000 intact PTH) by solid-phase; enzyme-labe-lled, chemiluminescent sequential immunometric assay; calcium (Roche/ Hitachi Modular) by color test with final point and white sample determination; inorganic phosphate (Roche/Hitachi Phosphorus) and β-crosslap (β-CTX) by electrochemiluminescence immunoassay (ECLIA, Roche Eclecsys automated analyzers/E170 module). The analysis were performed at Teror Health Center after overnight fasting, both one day before familiarization and two days after finishing the training program sessions.
Statistical analysisA basic descriptive statistics (mean and standard deviation) and a comparative statistics ANOVA (2 x 2) with a 95% confidence interval were performed. In addition, the effect size has been calculated as described by Cohen47. The statistical package SPSS 12.0 was used for all statistical tests.
ResultsThe results of blood PTH, calcium, phosphate, and β-crosslap concentrations are shown in table 2. There were no changes observed for the values of calcium, phosphate, and β-crosslap at the end of the training program for any of the groups. We should highlight that the measured calcium corresponds to total blood calcium, not ionized calcium. On the contrary, PTH shows a significant improve for EG (p < 0.05). None of the subjects commented on having experienced any negative side effects.
Table 2 Values of parathormone (PTH), calcium, phosphate, and β-crosslap forexperimental group (EG; n = 8) and control group (CG; n = 8) before and after the 8-week WBV training are given as mean ± standard deviation
By means of the complementary pre-post tests applied for the assessment of physical condition and anthropometry (table 3), it is confirmed that, after training, there were significant changes (p < 0.05) in knee extensor musculature strength levels for both groups, with changes being more marked for EG in comparison to CG (see effect size). In addition, EG also showed a significant increase in calf and thigh muscle area (16.9%, p < 0.05, and 8.3%, p < 0.05; respectively); conversely, CG showed only small increments that did not reach statistical significance. The mean skinfold sum showed a statistical significant decrease in EG albeit no statistically significant changes were observed in body weight in any of the analyzed groups.
Table 3 Morphofunctional parameters for experimental group (EG; n = 8) and control group (CG; n = 8) before and after the 8-week whole body vibration training
DiscussionThe obtained results indicate that, after finishing the WBV training program, PTH concentration significantly increased in EG. Thus, it seems there is a relationship between the PTH production increase and the vibrating stimuli from the WBV platforms.
The lesser-intensity (very low) vibration stimulus (frequency 10 Hz) used in CG also provoked an increase in PTH although it was not statistically significant. The increases observed were not accompanied by any changes in calcium or phosphate values in neither one of the groups (EG and CG). Normally, calcium concentration in extracellular fluids is regulated in a very precise manner, and very rarely varies in a small percentage from its reference values (8.2-10.5 mg · dl-1), with daily variations that are not above 5%. Minimal changes in this parameter are rapidly detected and influence PTH. In our case, calcium levels of the analyzed subjects were high, as expected in subjects of such age range, staying elevated until the end of the study (table 2). Phosphate, which normal blood concentration oscillates between 3 and 4.5 mg · dl-1 in adults, showed a tendency towards a slight decrease in EG (4.2%; effect size: 0.45) although values were always within normal range. Such tendency was not observed in CG, which even showed increasing values.
The regulation of PTH secretion is basically related to blood calcium concentration. However, during physical exercise, other factors, in addition to calcium, may modify PTH secretion; such factors are catecholamines, and acidosis, which are influenced by the training load. While PTH secretion is related to blood calcium concentration, several studies show that the variations in PTH response during exercise are independent from calcium concentration 39, 50,51. The adrenergic system is activated during exercise52, and it has been proved that this system influences the regulation of PTH secretion53. Elevated values of blood PTH concentration upon finishing training seem to be more related to this hormone’s anabolic function39. Although the complex mechanisms by which PTH may promote osseous mass gain are not clearly understood34, there are several studies showing that an intermittent infusion of PTH increases bone formation more than it increases bone resorption54,55, leading to an increased bone mass54,56-58.
In the present study, serum PTH values increased in both groups (EG: 44.3%; CG: 17.3%) although the increase only reached statistical relevance in EG. However, it should be noted that the increase in PTH levels does not surpass the normality range estimated for this population (0-68.2 mg · dl-1). In our study, we cannot accurately conclude that the in-creases in PTH levels might result in an osseous remodeling. However, the described behaviour and the moderate decrease in phosphate levels could make us think it might be happening indeed. We could infer that there are no significant changes in pro-collagen I levels since β-crosslap, a resorption marker, which indicates that the degraded type I collagen fragments appear as a consequence of the osteoclasts’ action during the degradation of collagen in bones59 did not experience any significant modification in its values (table 2). Since no changes were observed in this marker, this could indicate that, while osseous degradation has not been increased, other construction processes have done it indeed.
It is worth mentioning, due to the possible important repercussion of the finding, that most of the participants subjectively referred to having experienced an increase in strength in lower limbs. Complementary pre-post tests applied for assessing physical condition and anthropometry, showed that: a) in spite of both CG and EG significantly improving lower limb muscle strength after the training period, such increase was greater in EG than in CG; by the effect size calculation (1.49 vs 0.94, respectively), we could postulate that, when increasing sample size, the difference among groups could reach statistical significance; b) thigh and calf muscle area were significantly higher in EG as compared to CG after training; c) the skinfold sum showed that EG experienced a greater decrease in fat mass than CG after training. Both the increase in muscle strength and in muscle area are substantially important for improving the quality of life in the elderly, in aspects such as a greater autonomy, and, possibly, less sarcopenia60.
In conclusion, it seems that low-intensity training programs using the vibration platform, in elderly subjects, generate an endocrine response on PTH which results favorable to osseous construction processes. However, the development of more exhaustive studies, assessing a bigger sample, are needed in order to advance the knowledge on the effect the vibration stimulus produces on osseous remodeling markers.
AcknowledgementsWe would like to thank all the participants in the present study for having volunteered and adhered to the whole study protocol. Likewise, we would like to thank Dr. Prof. Clodoaldo de Sá for his numerous and valuable suggestions and contributions during the correction and editing process of the manuscript.
Correspondence:
J. M. García-Manso. Departamento de Educación Física. Facultad de Ciencias de la Actividad Física y el Deporte. Universidad de Las Palmas de Gran Canaria. 35017 Islas Canarias. España. E-mail: jgarcia@def.ulpgc.es
