



The aim of this study was to analyze the effects of aerobic exercise on biochemical, anthropometric and hemodynamic profiles of patients with type 2 diabetes mellitus, in randomized clinical trials and case–control studies.
MethodThe databases used in the study were: MEDLINE, BVS (LiLacs), IBECS (Spain), MED Caribbean and Central Controlled Clinical Trial Registry. We included studies published from 2004 to 2014. Were analyzed anthropometric (body mass index, waist circumference and percentage of body fat), hemodynamic (blood pressure and heart rate) and biochemical parameters (glycemia, glycated hemoglobin, insulin, cholesterol-HDL, cholesterol-LDL and triglycerides).
ResultsThe results showed that, aerobic exercise of moderate intensity and often three or more times a week, promoted a significant reduction in waist circumference, blood glucose and diastolic blood pressure.
ConclusionIt is concluded that there are benefits of aerobic exercise of moderate intensity practiced regularly often more than three times a week on waist circumference, glycemia and diastolic blood pressure in diabetes mellitus type 2.
El propósito de este estudio fue analizar los efectos del ejercicio aeróbico sobre los perfiles bioquímicos, antropométricos y hemodinámicos de pacientes con diabetes mellitus tipo 2, en ensayos clínicos aleatorizados y estudios de casos y controles.
MétodoLas bases de datos utilizadas en el estudio fueron: MEDLINE, BVS (LiLacs), IBECS (España), MED Caribe y el Registro Central de Ensayos Clínicos Controlados. Se incluyeron estudios publicados desde 2004 hasta 2014. Se analizaron medidas antropométricas (índice de masa corporal, circunferencia de la cintura y porcentaje graso), hemodinámicas (presión arterial y frecuencia cardíaca) y bioquímicas (glucemia, hemoglobina glicosilada, insulina, Colesterol-HDL, Colesterol-LDL y triglicéridos).
ResultadosLos resultados mostraron que el ejercicio aeróbico, de intensidad moderada, realizado de 3 veces o más por semana causó una reducción significativa en la circunferencia de la cintura, la glucemia y la presión arterial diastólica.
ConclusiónSe concluye que hay beneficios del ejercicio aeróbico de intensidad moderada, practicado regularmente más de 3 veces a la semana, en el perímetro de la cintura, glucemia y presión arterial diastólica en pacientes con diabetes tipo 2.
O objetivo do presente estudo foi analisar os efeitos do exercício aeróbico sobre os perfis bioquímico, antropométrico e hemodinâmico de pacientes com diabetes mellitus tipo 2, em ensaios clínicos randomizados e estudos de caso-controle.
MétodoAs bases de dados utilizadas no estudo foram: MEDLINE, BVS (LiLacs), IBECS (Espanha), MED Caribe e Central de Registros de Ensaios Clínicos Controlados. Foram incluídos estudos publicados nos anos de 2004-2014. Foram analisadas as medidas antropométricas (IMC, circunferência de cintura e percentual de gordura), hemodinâmicas (pressão arterial e frequência cardíaca) e bioquímicas (glicemia, hemoglobina glicada, insulina, colesterol-HDL, colesterol-LDL, triglicérides).
ResultadosOs resultados evidenciaram que o exercício aeróbico, de intensidade moderada e com frequência igual ou superior a três vezes por semana promoveu redução significativa no perímetro da cintura, na glicemia e na pressão arterial diastólica.
ConclusãoConclui-se que há efeitos benéficos do exercício físico aeróbio de moderada intensidade, praticado de forma regular com frequência de 3 ou mais vezes por semana, sobre o perímetro da cintura, glicemia e pressão arterial diastólica em indivíduos com diabetes mellitus tipo 2.
Diabetes mellitus type 2 (DM2) is a metabolic disease characterized by insulin resistance and dysfunctional pancreatic beta cells. Patients are often concomitantly overweight or obese.1 DM2 is one of the leading causes of death worldwide, and is primarily associated with an aging population, urbanization, and high prevalence of physical inactivity. Diabetes affects 382 million people worldwide, of which 61 million are located in the Americas, with 24 million in Central and South America.2 In developed countries, DM2 is ranked between the fourth and eighth position among the major diseases in terms of prevalence, and the direct costs of treatment vary between 2.5 and 15% of annual health budgets.3 In Brazil, between 1991 and 2000 there was a 19% increase in the number of cases, followed by a decline of 8% between 2000 and 2009; however, in 2009 alone, incidence increased by 24%.4 The Brazilian capitals with the highest prevalence of DM2 in 2012 were São Paulo (9.3%) and Florianópolis (7.3%).4
Given this epidemiological situation, it is critical to invest in studies that provide scientific evidence on the efficiency and effectiveness of targeted protocols and intervention processes that improve the quality of life for DM2 patients. In this context, active participation in exercise programs is the unanimous recommendation of health professionals for both prevention and treatment of DM2.
Physical exercise programs may aid long-term control of blood glucose levels, and can acutely stimulate glucose uptake, which helps to increase the sensitivity of insulin to receptors.5 An understanding of the underlying physiological responses to physical exercise is crucial for adequate medical management and proper counseling with respect to suggested activity and/or physical exercise load. This goal will improve the efficiency of diabetes interventions, increasing exercise and activity levels in DM2 patients.6
Current recommendations for DM2 patients include at least 150min of moderate intensity exercise per week (over 3–7 days), or 75min of high intensity exercise per week (over 3 days).1 This review article evaluated the effects of aerobic exercise on biochemical, anthropometric, and hemodynamic profiles of patients with DM2 in randomized clinical trials, case studies, and controls.
MethodLiterature search strategySystematic survey of the primary studies was conducted using the following databases: MEDLINE (PubMed), BVS (LiLacs), IBECS (Spain), Med Caribe, and the Central Registry of Controlled Clinical Trials (Cochrane), published between 2004 and December 2014. A search strategy was developed for MEDLINE, accessed via PubMed, based on titles of Medical Subject Headings (MeSH) identified through article terms and key words. We searched for articles in LiLacs using Health Sciences Descriptors (DeCS). We reviewed reference lists of all articles included in the study.
The search strategy for Med Caribbean used MeSH terms and their synonyms as a starting point. However, the search strategy for articles in the Central Registry of Controlled Clinical Trials was based on the keywords to yield a greater number of articles.
Various combinations of the keywords “physical exercise”, “physical activity” and “diabetes mellitus type 2” were used in English, Portuguese, and Spanish as appropriate, using the MeSH terms “exercise”, “motor activity”, and “diabetes mellitus type 2” crossed with Boolean connectors AND, OR, or AND OR.
The search strategy began with selection of a diabetic population (type 2) consisting of groups with diabetic intervention via regular exercise or physical activity, and control patients (with or without diabetes) that received only counseling/education about intervention methods and related health outcomes. An additional search filter was used to select only clinical controlled studies and/or randomized trials performed with adult humans.
Criteria for inclusion and exclusionThe following inclusion criteria were selected, which were applied independently: (a) the study presented a controlled clinical trial design (to identify impacts of the intervention) and/or randomized or case studies and controls (identical risk factors for the outcome) with the use of proposal-based activity and/or aerobic exercise; (b) the study contained a population with individuals over the age of 19; (c) the study had at least two groups; (d) the duration of the study included more than 3 months of intervention; (e) the intervention group was composed of a diabetic population; (f) the study evaluated anthropometric measurements (body fat, body weight, or waist circumference) and/or biochemical (cholesterol, fasting glucose, or glycated hemoglobin) and/or hemodynamic (blood pressure or heart rate) parameters; and (g) the study presented intervention data (type of exercise, load, and intensity).
The studies were separated for analysis according to the objectives and parameters evaluated. Researchers assessed aerobic training vs. education or sedentary lifestyle intervention, and the relationship between the weekly frequency of exercise and improvement in biochemical, anthropometric and hemodynamic profiles. We excluded studies with children or teenagers, or including patients with pathologies associated with diabetes. We also excluded studies of systematic review, narrative review, overview and meta-analysis, as well as animal studies.
Data extractionTwo independent examiners searched for articles in the databases by analysis of titles, abstracts, and full papers, and assessed eligibility for inclusion of each study. Disagreements were discussed and, if unresolved, a third reviewer was consulted to decide whether the study should be included or excluded. Standardized worksheets were designed for data extraction such that the reviewers were able to extract information about the study characteristics, participants, eligibility criteria, intervention methods, and the observed outcomes, including measures of variability when available.
For data mining, results were considered as outcomes related to the chosen anthropometric, biochemical, and hemodynamic parameters. Researchers reviewed articles twice to ensure accuracy.
ResultsInclusion of studiesDatabase searched yielded 119 articles in total. Of these, 87 were excluded after evaluation of titles and abstracts, leaving 32 articles identified as eligible. Of these, 13 did not evaluate biochemical and anthropometric profiles, one studied an adolescent population, three evaluated the effect of only a single intervention session, one evaluated a monitoring program, seven did not evaluate the effects of an exercise program, and two did not include diabetes type 2 (Fig. 1).

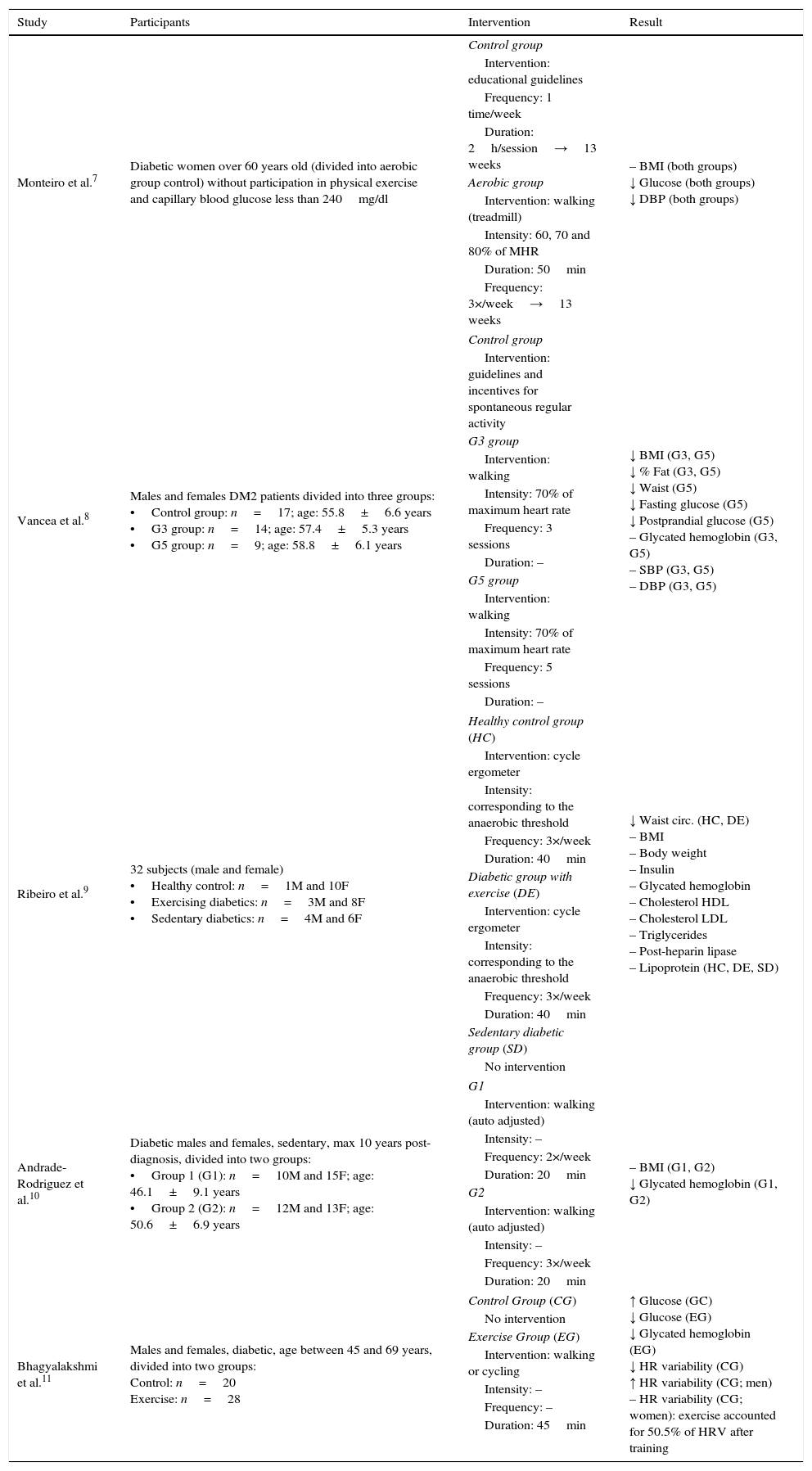
Five studies met all inclusion criteria, all of which had a case–control design. Studies were arranged alphabetically by first author name. Table 1 presents the main results of analysis, considering the population sampled, type of treatment (frequency, volume and intensity), and the outcomes achieved.
Main characteristics of the studies included in this review.
| Study | Participants | Intervention | Result |
|---|---|---|---|
| Monteiro et al.7 | Diabetic women over 60 years old (divided into aerobic group control) without participation in physical exercise and capillary blood glucose less than 240mg/dl | Control group | – BMI (both groups) ↓ Glucose (both groups) ↓ DBP (both groups) |
| Intervention: educational guidelines | |||
| Frequency: 1 time/week | |||
| Duration: 2h/session→13 weeks | |||
| Aerobic group | |||
| Intervention: walking (treadmill) | |||
| Intensity: 60, 70 and 80% of MHR | |||
| Duration: 50min | |||
| Frequency: 3×/week→13 weeks | |||
| Vancea et al.8 | Males and females DM2 patients divided into three groups: •Control group: n=17; age: 55.8±6.6 years •G3 group: n=14; age: 57.4±5.3 years •G5 group: n=9; age: 58.8±6.1 years | Control group | ↓ BMI (G3, G5) ↓ % Fat (G3, G5) ↓ Waist (G5) ↓ Fasting glucose (G5) ↓ Postprandial glucose (G5) – Glycated hemoglobin (G3, G5) – SBP (G3, G5) – DBP (G3, G5) |
| Intervention: guidelines and incentives for spontaneous regular activity | |||
| G3 group | |||
| Intervention: walking | |||
| Intensity: 70% of maximum heart rate | |||
| Frequency: 3 sessions | |||
| Duration: – | |||
| G5 group | |||
| Intervention: walking | |||
| Intensity: 70% of maximum heart rate | |||
| Frequency: 5 sessions | |||
| Duration: – | |||
| Ribeiro et al.9 | 32 subjects (male and female) •Healthy control: n=1M and 10F •Exercising diabetics: n=3M and 8F •Sedentary diabetics: n=4M and 6F | Healthy control group (HC) | ↓ Waist circ. (HC, DE) – BMI – Body weight – Insulin – Glycated hemoglobin – Cholesterol HDL – Cholesterol LDL – Triglycerides – Post-heparin lipase – Lipoprotein (HC, DE, SD) |
| Intervention: cycle ergometer | |||
| Intensity: corresponding to the anaerobic threshold | |||
| Frequency: 3×/week | |||
| Duration: 40min | |||
| Diabetic group with exercise (DE) | |||
| Intervention: cycle ergometer | |||
| Intensity: corresponding to the anaerobic threshold | |||
| Frequency: 3×/week | |||
| Duration: 40min | |||
| Sedentary diabetic group (SD) | |||
| No intervention | |||
| Andrade-Rodriguez et al.10 | Diabetic males and females, sedentary, max 10 years post-diagnosis, divided into two groups: •Group 1 (G1): n=10M and 15F; age: 46.1±9.1 years •Group 2 (G2): n=12M and 13F; age: 50.6±6.9 years | G1 | – BMI (G1, G2) ↓ Glycated hemoglobin (G1, G2) |
| Intervention: walking (auto adjusted) | |||
| Intensity: – | |||
| Frequency: 2×/week | |||
| Duration: 20min | |||
| G2 | |||
| Intervention: walking (auto adjusted) | |||
| Intensity: – | |||
| Frequency: 3×/week | |||
| Duration: 20min | |||
| Bhagyalakshmi et al.11 | Males and females, diabetic, age between 45 and 69 years, divided into two groups: Control: n=20 Exercise: n=28 | Control Group (CG) | ↑ Glucose (GC) ↓ Glucose (EG) ↓ Glycated hemoglobin (EG) ↓ HR variability (CG) ↑ HR variability (CG; men) – HR variability (CG; women): exercise accounted for 50.5% of HRV after training |
| No intervention | |||
| Exercise Group (EG) | |||
| Intervention: walking or cycling | |||
| Intensity: – | |||
| Frequency: – | |||
| Duration: 45min | |||
BMI, body mass index; CG, control group; DBP, diastolic blood pressure; DE, diabetic group with exercise; DM2, diabetes mellitus type 2; EC, exercise group; F, female; G1, Group 1; G2, Group 2; HC, healthy control group; HR, heart rate; HRV, heart rate variability; M, male; MHR, maximum heart rate; SBP, systolic blood pressure; SD, sedentary diabetic group; ↑, increase in parameter evaluated; ↓, reduction in parameter evaluated; –, no changes in parameter evaluated.
Four studies assessed the effects of aerobic exercise on anthropometric measures in diabetic patients.7–10 Of these, only Vancea et al.8 demonstrated significant effects of the intervention programs. In this study, the intervention protocol consisted of exercise for 45min either three or five times per week, with 30min of that time walking to 70% of maximum HR. Patients showed a significant reduction in BMI, waist circumference, percent body fat, and fasting glucose, and the magnitude of these changes was greater in the five times per week group than in the three times per week group. The authors also point out that capillary blood glucose showed a downward trend after exercise in the group that exercised five times per week.
In a study by Monteiro et al.7 older female DM2 patients practiced aerobic exercise three times a week for 13 weeks, with an intensity of 60–80% maximum heart rate. Results from the exercise group were compared to those from a control group that underwent DM2 educational sessions only. This study found no influence of aerobic exercise on BMI, however there was a BMI reduction of 1kg/m2 in the control group and 1.2kg/m2 in the experimental group.
Ribeiro et al.9 compared 32 subjects divided into three groups: 10 sedentary individuals with DM2; 11 physically active subjects without diabetes; 11 physically active diabetic subjects. The subjects with healthy vs. diabetic attributes were participated in an aerobic exercise program using a cycle ergometer (40min, three times per week for 4 months), while the sedentary DM2 subjects participated only a regular care program at the Clinical Hospital in Sao Paulo and did not engage in regular exercise. The aerobic exercise group had no changes in body weight or BMI, but did show a statistically significant reduction in waist circumference compared to the DM2 sedentary group.
Andrade-Rodriguez et al.10 evaluated the effects of weekly frequency of aerobic training (walking 2–3 times per week with moderate intensity, 20min per session, for 16 weeks) in two groups of 25 DM2 patients. In addition to the exercise protocol, all patients received 20h of educational lectures about the various benefits of exercise, food, and drug treatments. The subjects had no changes in BMI as a function of the training regimens. However, the distance covered in 12-min test increased significantly at the end of the training period in both groups, and glycated hemoglobin reduced significantly in both treatments (exercise and educational sessions).
Chronic effects of aerobic exercise on biochemical parametersThe studies showed a reduction in blood glucose7,8,11 and postprandial glucose,7 however results vary with respect to glycated hemoglobin. Ribeiro et al.9 and Vancea et al.8 reported no changes in glycated hemoglobin, while Bhagyalakshmi et al.11 and Andrade-Rodriguez et al.9 reported a decrease in these values.
According to Monteiro et al.,7 13 weeks of aerobic exercise was as effective as educational sessions for reducing blood glucose levels in their experimental population. They also found that aerobic exercise sessions did not improve triglycerides, glycemia, or insulinemia in diabetic or healthy adults (i.e., no differences compared to sedentary diabetic adults).
Ribeiro et al.9 reported that groups performing exercise for 4 months (both diabetic and non-diabetic) showed no changes in plasma concentrations of total cholesterol, cholesterol-LDL (LDL), cholesterol-HDL (HDL), triglycerides (TG), glucose or insulin compared to the sedentary DM2 groups. However, HDL particles were converted to larger particles in the exercise group, which improved LDL oxidation rates.
Bhagyalakshmi et al.11 observed improvement in blood glucose and glycated hemoglobin rate in DM2 patients that participated in an exercise program for 9 months. In this study, 48 patients (male and female) were separated into two groups, an aerobic training group (30min/session, n=28), and a control group that did not perform physical exercise (n=20).
Vancea et al.8 evaluated the effects of 20 weeks of aerobic training at 70% maximum heart rate in three groups of diabetic patients aged 55–59 years, in order to compare the effects of exercise programs performed with three and five weekly sessions, and controls. Results showed that neither training regimen influenced glycated hemoglobin levels, however fasting plasma glucose and postprandial glucose significantly reduced after 20 weeks in the in five times per week group compared to controls.
Andrade-Rodriguez et al.10 evaluated the effects of the weekly frequency of aerobic training on glycated hemoglobin level and aerobic capacity in 50 male and female subjects. Subjects were divided in two groups, that walked with moderate intensity for 20min either two (Group 1=G1) or three times per week (Group 2=G2), for 16 weeks. During this period all patients received 20h of educational lectures on exercise, food, and drug therapies, and the associated benefits. At the start of the program majority of participants had high glycated hemoglobin levels, which reduced after 16 weeks in both groups (7.38% and 7.10% in groups G1 and G2, respectively). Although there were no significant changes in aerobic capacity, glycated hemoglobin index was three times less in the G2 group, a result that could have been related to other factors as well.
Chronic effects of aerobic exercise on hemodynamic parametersOnly three studies reported chronic effect of aerobic exercise on hemodynamic parameters.7,8,11 Monteiro et al.7 found that systolic blood pressure (SBP) benefited from both aerobic exercise and educational interventions, with the control group (educational) decreasing from 139.8mmHg to 128.1mmHg and the aerobic group decreasing from 140.0mmHg to 124.5mmHg. Diastolic blood pressure (DBP) reduced to a greater extent in the aerobic exercise group (75.4–54.4mmHg) than in the educational group (77.5–69.1mmHg).
Vancea et al.8 evaluated the effects of 20 weeks of aerobic training at 70% maximum heart rate, and found no changes in SBP and DBP in groups training either three or five times per week. The latter showed a slight drop in blood pressure (SBP decreased from 128.0±2.0 to 125.0±2.0mmHg, and DBP increased from 80.0±2.0 to 76.0±3.0mm Hg). Further, Bhagyalakshmi et al.11 assessed the effects of aerobic exercise in DM2 patients after nine months of training, and demonstrated improvements in heart rate variability. The improvement was greater in men than in women, and greater in younger than in older subjects.
In general, hemodynamic improvements from aerobic training regimens can provide favorable long-term prognosis for patients with DM2.
DiscussionAfter an exhaustive search of the selected databases, we were only able to include five studies in this review. This highlights the lack of controlled clinical trials and case studies, and lack of appropriate controls in studies assessing chronic effects of aerobic exercise in DM2 patients.
Chronic effects of aerobic exercise on anthropometric parametersThe anthropometric measurements most affected in the studies were BMI, body fat percentage, and waist circumference. Waist circumference was evaluated in Vancea et al.,8 with a greater reduction in individuals who exercised five times per week compared to three times per week. Ribeiro et al.9 also found a reduction in waist circumference of healthy and diabetic groups after a 4-month aerobic exercise program. There was also a significant reduction in body fat percentage in both groups. Considering the positive relationship between abdominal circumference, central obesity, insulin resistance, metabolic syndrome and cardiovascular disease, exercise programs that promote reduction in these variables are good candidates for inclusion in DM2 treatment programs.12
Mathieu et al.13 showed a reduction in body fat percentage in diabetics who increased their level of physical activity, resulting in improved physical fitness and reduced cardiovascular risk in participants. Adipose tissue, stores energy, but is also considered an active endocrine organ. It is responsible for secreting hormones that form the link between muscle tissue, the central nervous system, and adipocytes in carbohydrate metabolism regulation, intermediary metabolism, and insulin signaling pathways.14 However, excess adipose tissue impedes the uptake of glucose by muscle tissue. Accordingly, reducing body fat percentage plays an important role in metabolic regulation, reducing the risk of developing diseases, particularly those of cardiovascular origin.14
The effects of aerobic training on BMI were assessed in Miller et al.,7 Vancea et al.,8 Ribeiro et al.9 and Andrade-Rodriguez et al.;10 Vancea et al.8 was the only one to show significant differences in BMI of DM2 patients in response to intervention. Vancea et al.8 believe that the delayed decrease in BMI (which occurred only after the 20th week of training) was likely due to unconscious compensatory increase in caloric intake (i.e., due to training). It is also worth noting that individuals with BMI close to normal may still have a waist circumference associated with risk for cardiovascular disease, especially in males. For this reason, this particular method may not be as reliable for diagnosing risk cardiovascular risk.15 Reduction in BMI as the primary purpose of aerobic exercise programs from diabetics should be reviewed, since the protocols used in the studies analyzed in this review did not find significant reductions in BMI over their respective intervention periods.
Chronic effects of aerobic exercise on biochemical measuresThe studies analyzed in this review evaluated biochemical responses to different intervention protocols with various relationships between exercise duration, intensity, and weekly frequency. Blood glucose levels, glycated hemoglobin, total cholesterol, HDL, and LDL were measured.
Blood glucose decreased significantly only in groups with high weekly training frequency (five times a week).8,11 In one study, changes in basal blood glucose levels were similar in the groups that exercised three times a week and control groups.7 These studies provide evidence that the positive responses in the control of DM2 patient blood glucose levels are associated with higher weekly frequency of exercise.
Ribeiro et al.9 was the only study evaluating effects of aerobic exercise on lipid profile. Although the authors did not find positive treatment effects on lipid profile, they did find that aerobic exercise practiced three times a week at moderate intensity increased the efficiency of HDL in LDL oxidation (regardless of changes in insulin resistance), and increased HDL plasma concentrations.
One of the main targets in the treatment of diabetic dyslipidemia is HDL. Low HDL levels are often associated with elevated levels of TG, and may be associated with the aggressive nature of cardiovascular disease in diabetic patients.16 According to the American Association of Diabetes,17 DM2 patients generally do not show quantitative differences in the mean concentration of cholesterol and LDL compared to healthy individuals. However, from a qualitative point of view, are distinguished by high profile atherogenicity by the higher proportion of small, dense LDL particles.
Andrade-Rodriguez et al.10 and Bhagyalakshmi et al.11 showed that aerobic exercise at a frequency of three times a week is more efficient than twice per week for controlling glycated hemoglobin levels, a result also found in other studies.18,19 Although glycated hemoglobin is an important parameter for the diagnosis and monitoring of diabetes and pre-diabetes, studies by Andrade-Rodriguez et al.,10 Bhagyalakshmi et al.,11 and Miller et al.7 suggest that only high-frequency training protocols (five times a week) promote positive changes in this parameter. Thus, intervention programs for patients with DM2 should be structured to include aerobic activity of moderate to high intensity, and should aim for five times per week.
Chronic effects of aerobic exercise on hemodynamic measurementsSeveral studies evaluated chronic effect of exercise on heart rate variability and blood pressure (systolic and diastolic). Bhagyalakshmi et al.11 was the only study that found that exercise training increasing Heart Rate Variability (HRV) (i.e., exercise training provided benefits relative to the control group). HRV quantifies changes in beat-to-beat heart rate caused by changes in autonomic activity, and low HRV is a strong predictor of mortality in diabetic patients. A healthy body system responds quickly and completely to environmental challenges in order to maintain homeostasis.20
Monteiro et al.7 showed significant decrease in DBP rates in subjects that exercised compared to those that received only educational sessions. SBP reduced in both groups. Vancea et al.8 demonstrated marginal influence of aerobic exercise on SBP. However, weekly frequency of training also seems to affect blood pressure response, where greater reduction in DBP was observed in the group that performed exercise five times weekly compared to other groups (three times weekly and sedentary).
According to Green et al.6 the cardiovascular system is designed to perfuse the cells of all tissues. Each tissue has control over its own perfusion or blood flow, but the level of local control depends on a sufficiently high level of blood pressure maintained by a central control mechanism. Local control of blood flow occurs through regulation of systemic arterial pressure systems. Among systems controls, central regulation of blood pressure is the most important feature of the cardiovascular system because it allows local control of blood flow. In DM2 patients, heart rate is one variable that can be monitored to control progression of the training regimen.
All studies required training at least twice a week, and for at least 20min per session. Balducci et al.21 concluded that, at least in diabetic subjects with low physical fitness, low-intensity training is as effective as a high-intensity training to improve modifiable risk factors for cardiovascular disease. This suggests that, for practical and therapeutical purposes, intensity is not as important as training frequency and type of exercise.
Studies have shown that suitable training intensity for diabetic patients should be between 60 and 80% maximum heart rate.8,10 Aerobic exercise of moderate intensity performed between 3 and 5 times a week can aid control of cardiometabolic parameters in type 2 diabetics.
Sigal et al.22 recommend that to control glycemic parameters, maintain weight, and reduce cardiovascular disease risk, diabetics should perform moderate-intensity aerobic exercise more than 150min per week (40–60% of VO2max or 50–70% HR), or more than 90min/week of vigorous aerobic exercise (>60% of VO2max or >70% HR). Physical activity should be occur 3 days per week, with no more than two consecutive days of no activity. Boulé et al.23 assert that the effects of a single aerobic exercise session on insulin sensitivity lasts 24–72h, depending on duration and intensity. Although the acute response rarely exceeds 72h,23 it nonetheless plays an important role in modulation of glucose, independent of drug treatments or other interventions.
LimitationsOne limitation of the study is heterogeneity in the variables observed in the reviewed studies. Although the studies addressed the same theme, heterogeneity may result in reducing the power of generated conclusions. Another limitation was that not all the potential effects were evaluated.
ConclusionThe scientific literature demonstrates beneficial effects of moderate-intensity aerobic exercise practiced with a frequency of three times a week or more on waist circumference, blood glucose and diastolic blood pressure in DM2 patients. This study also points to the need for development of randomized clinical trials to provide more information about the types of exercises, as well as duration, intensity, and appropriate weekly frequency to yield positive effects for patients with DM2.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
