






Evaluate the cardiorespiratory fitness (CRF) and the body mass index (BMI) of schoolchildren according to the cutoff points established by the Fitnessgram®. Just as determine the influence of BMI on CRF in children and propose an equation for predicting VO2max from the body composition.
MethodThe sample consisted of 288 students of basic level of public education in the city of Aracaju – Sergipe – Brazil, aged between 10 and 14 years, of these, 142 were female. To evaluate the CRF the 20-m shuttle run test was chosen. The results of the variable were classified in accordance with the criteria established by the Fitnessgram®.
ResultsIt was evidenced that the cardiorespiratory fitness on males was higher than females. Relative to BMI, there were no differences between the groups, while more than 80% of the entire sample behaved within criteria established by the Fitnessgram®. On the other hand, 57% of the female group presented VO2max below criterion. It was confirmed an inverse relationship between VO2max and BMI on children and adolescents.
ConclusionThe students in this study showed adequate levels of body composition and CRF below the area related to health, according to the criteria of the Fitnessgram®. The proposition of a linear regression equation to estimate VO2max without exercise pointed out an inverse relationship between both variables.
Evaluar la aptitud cardiorrespiratoria y el índice de masa corporal (IMC) de escolares mediante los puntos de corte establecidos por la batería internacional de test Fitnessgram®. Así como determinar la influencia del IMC en la aptitud cardiorrespiratoria (CRF) en niños y proponer una ecuación de predicción del VO2máx a partir de la composición corporal.
MétodoLa muestra estuvo conformada por 288 estudiantes de nivel básico de la educación pública de la ciudad de Aracaju-Sergipe-Brasil, de edades comprendidas entre 10-14 años, de los cuales, 142 eran mujeres. Para evaluar el CRF fue utilizada la prueba de 20-m shuttle run test (PCN). Los resultados de la variable se clasificaron de acuerdo con los criterios de aplicación establecidos por el test internacional Fitnessgram®.
ResultadosSe evidenció que la CRF en varones fue mayor que en las mujeres. Relativo al IMC, no hubo diferencias entre los grupos, mientras que más de 80% de toda la muestra se comportó dentro de los criterios establecidos por la Fitnessgram®. Por otro lado, el 57% del grupo femenino presentó VO2máx por debajo de los niveles. Se confirmó una relación inversa entre el VO2máx y el IMC en niños y adolescentes.
ConclusiónLos escolares, en este estudio, mostraron niveles adecuados de composición corporal y CRF por debajo del área relacionada con la salud de acuerdo con los criterios de Fitnessgram®. La proposición de una ecuación de regresión lineal, para estimar el VO2máx sin ejercicio señaló una relación inversa entre ambas variables.
Avaliar a aptidão cardiorrespiratória e índice de massa corporal (IMC) de escolares de acordo com os pontos de corte estabelecidos pela bateria de teste internacional Fitnessgram®. Além de determinar a influência do IMC sobre a aptidão cardiorrespiratória em crianças e propor uma equação de predição do VO2máx a partir da composição corporal.
MétodoA amostra consistiu de 288 estudantes do ensino básico da educação pública na cidade de Aracaju (Sergipe, Brasil), com idade entre 10-14 anos, dos quais 142 eram meninas. Para avaliar a aptidão cardiorrespiratória optou-se pelo 20-m shuttle run test. Os resultados das variáveis foram classificados de acordo com os critérios estabelecidos pelo Fitnessgram®.
ResultadosConstatou-se que a aptidão cardiorrespiratória dos meninos foi maior do que das meninas. Com relação ao IMC, não houve diferenças entre os grupos, enquanto mais de 80% de toda a amostra se comportou dentro dos critérios estabelecidos pelo Fitnessgram®. Por outro lado, 57% do grupo feminino apresentou VO2máx abaixo dos critérios. Confirmou-se uma relação inversa entre VO2máx e o IMC em crianças e adolescentes.
ConclusãoOs alunos deste estudo apresentaram níveis de composição corporal adequados e de aptidão aeróbia abaixo da área relacionada à saúde, de acordo com os critérios do Fitnessgram®. A proposição de uma equação de regressão linear para estimar o VO2máx sem exercício apontou uma relação inversa entre as 2 variáveis.
The decrease in the amount of motor activity observed on children and adolescents in different socioeconomic spectra1 has raised interest in the knowledge of physical fitness and health, in order to classify it from scores based on referenced criteria both nationally and internationally, which involve physical qualities able to reflect patterns of behavior and environmental.
Closely related to the health, the low levels of cardiorespiratory fitness (CFR) on childhood and adolescence are associated with an increased early death risk due to any cause, especially cardiovascular diseases.2,3 So the prevention of cardiovascular diseases should begin still during the school stage, given that the adoption of healthy attitudes on that age range is perpetuated into adulthood.
In this way it is important to detect in advance, even within the school environment, children and adolescents with a predisposition to low aerobic fitness. In this sense, the development of mathematical models for predicting CRF without exercise test could be feasible in epidemiological studies4 and very useful for physical education teachers.
From this perspective, the presented study aimed to evaluate the CRF and the BMI of schoolchildren of both sexes according to the cutoff points established by the Fitnessgram®, as well as determine the influence of BMI on CRF of children and propose an equation for predicting VO2max from the body composition.
MethodParticipantsData collection was performed in a cross-sectional mode, and the target population of this study consisted on students of both genders enrolled in eight elementary schools distributed in the urban area of Aracaju, a city located on the coast of the state of Sergipe, Brazil. It lies between the capitals with lower socioeconomic inequalities and contributes greatly to the second highest Human Developing Index (HDI) among the states in northeastern region. The intervention took place between the months of September and November 2005, in obedience to the school calendar of the season.
To determine the surveyed schools, the city was divided into three regions: north, center and south, and by means of a draw three schools were chosen by region. Schools should have the minimum physical structure for the tests (e.g. multi-sports court). The sample, selected randomly during physical education classes, composed by 288 children (142 females) with age range between 9.50 and 14.49 years. We used the decimal age children as Ross and Marfell-Jones,5 which accurately represents the interval between the date of birth and date of the test.
The present study adopted the following inclusion criteria: belong to the preset age group, attend school regularly and take part in physical education classes on the day and time scheduled. The exclusion criteria were: experience any clinical symptoms that prevented temporarily or permanently be subjected to the tests and do not agree with the terms of consent by the responsible person.
Two professionals and four physical education academics carried out tests and measurements. To avoid discrepancies between measurements, each team member performed the same activity during the intervention. Before data collection, a training program was conducted in the test battery.
Procedures and measuresAnthropometric measurementsAnthropometric variables whose values are presented in Table 1, were body mass (kg) and height (m), as well as measures of skinfolds, in conformity with stablished standards.5 The body fat percentage (BF%) was determined as proposed Lohman.6 We used the caliper skinfold Cescorf® (CSC). The CSC presents identical design and mobility to the Harpenden model, provides a pressure of approximately 10g/mm2, measures to an accuracy of 0.1 mm, up to a jaw width of 88 mm.7 Skinfolds considered for the study were: triceps and subscapularis.
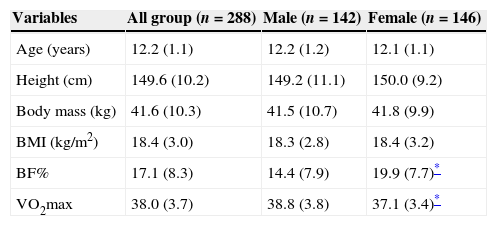
Descriptive profile of the sample (mean and standard deviation) for the anthropometry and cardiorespiratory fitness.
| Variables | All group (n=288) | Male (n=142) | Female (n=146) |
|---|---|---|---|
| Age (years) | 12.2 (1.1) | 12.2 (1.2) | 12.1 (1.1) |
| Height (cm) | 149.6 (10.2) | 149.2 (11.1) | 150.0 (9.2) |
| Body mass (kg) | 41.6 (10.3) | 41.5 (10.7) | 41.8 (9.9) |
| BMI (kg/m2) | 18.4 (3.0) | 18.3 (2.8) | 18.4 (3.2) |
| BF% | 17.1 (8.3) | 14.4 (7.9) | 19.9 (7.7)* |
| VO2max | 38.0 (3.7) | 38.8 (3.8) | 37.1 (3.4)* |
BMI: body mass index; BF%, body fat percentage; VO2max: maximal oxygen uptake.
The body mass index (BMI) was calculated as the ratio of the body mass (kg) and the squared height (m2). Therefore, the cutoff points of the Fitnessgram® were used to calculate the prevalence of children and adolescents located in the recommended range and in the range of risk of overweight and obesity.
Cardiorespiratory fitness (CRF)To evaluate the CRF from the maximal oxygen uptake (VO2max), we opted for the 20-m shuttle run test, according to what Léger et al.8 determine. This test was chosen because of its affordable implementation and compliance with the motor tests related to health contained in the Fitnessgram® battery, created by the Cooper Institute for Aerobics Research9 and because of its reliability and validity on children and adolescents has been widely documented.8,10,11 VO2max was calculated by the following equation, that covers the age range of this study. An r value of 0.71 was obtained:
y=31.025+3.238x1−3.248x2+0.1536x1x2, where:
y= VO2max (ml/kg/min)
x1 = maximal speed attained (km/h)
x2 = age (y)
To classify the performance level regarding the criteria established by the Fitnessgram® (VO2max: male 37.4–42.4, female 37.4–39.3; BMI: male 14.5–23.0, female 14.3–23.6),9 the results were categorize in three performance levels, “below”, “normal” and “above”. The following cutoff points were posted by Cooper Institute for Aerobics Research in 2013.
Ethics in researchThis study was conducted after the approval of the Municipal Education and according to the laws in force and in compliance with the Guidelines and Standards for Research Involving Humans, it was approved by the Ethics Committee of the Federal University of Sergipe under registration 1138.0.000.107-06.
Statistical analysisDescriptive statistics was used as first step to data analysis. A t-test for independent samples was chosen to compare means and the Chi-squared test was used to compare proportions. The relationship between VO2max and BMI was verified using the Pearson linear correlation and the lineal regression analysis. Level of significance was set at p< 0.05. The results were analysed by using GraphPadPrism 5 or SPSS software when necessary.
ResultsThe results of anthropometric variables observed in Table 1 were similar when comparing both sexes, regarding age, height, body mass (BM) and BMI. In terms of percentage of body fat, females had higher values (t=6.049, p<0.0001), and the boys showed higher values for maximum oxygen consumption (t=−4.106, p<0.0001).
Regarding the behavior of BMI in both sexes (Fig. 1), it may be noted no differences based on established criteria. Considering the cutoff points for the Fitnessgram®, 9.2% of girls were classified as “below”, 80.3% “normal,” and 10.5% “above”, the values considered in the same way for males were respectively, 8.2%, 79.5% and 12.3%.
.")
In relation to VO2max (Fig. 2), the percentage of boys classified as ‘above’, according to the cutoffs of the Fitnessgram®, was higher (41.8%) than the percentage of girls (19.7%). No statistically significant difference was found between girls and boys in the other classifications. The percentage of boys and girls classified as ‘below’ were 44.5% and 57.1%, respectively. The percentage of boys and girls classified as ‘normal’ were 13.7% and 23.2%, respectively.
. *p<0.05: statistically significant difference between male and female; %: percentage; VO2max: maximal oxygen uptake.")
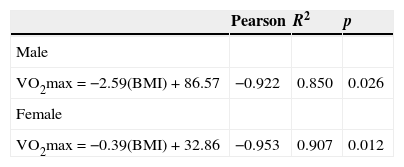
Both Figs. 3 and 4 show the correlation between the two variables, as well as the influence of the independent variable, BMI exerts on the dependent, VO2max, by determining the simple linear regression and the R2 value. This behavior was evaluated in both sexes and as many girls (R2=0.907) as boys (R2=0.850) presented strong correlation.
. VO2max: maximal oxygen uptake; BMI: body mass index.")
. VO2max: maximal oxygen uptake; BMI: body mass index.")
Analyzing Table 2, it was found in the study group a strong relationship in both sexes between the dependent and independent variables.
DiscussionThe present study aimed to evaluate the cardiorespiratory fitness and the BMI of schoolchildren of both sexes according to the cutoff points established by the Fitnessgram®, as well as determine the influence of BMI on CRF of children and propose an equation for predicting VO2max from the body composition.
There was a low compliance to the Fitnessgram® criteria associated with risk of obesity (Fig. 1). These results were better than those found by Bergmann et al.,12 in a study with students of 13–14 years old in the city of Canoas (Rio Grande do Sul, Brazil). In that occasion the authors detected 19% of boys and 15% of girls outside the health criteria recommended by Projeto Esporte Brasil (PROESP-BR). This may be attributed to the changes and differences in lifestyles of each region or country.13
In relation to other national studies, such as Hobold and Hübner14 with students of 10–14 years old, the BMI behaved as ‘below’, for both female and male from the city of Marechal Cândido Rondon (Paraná, Brazil). Ronque et al.15 in adolescents aged 10–15 years old from the city of Londrina (Paraná, Brazil), obtained higher BMI values than the present study, in individuals with low and high cardiorespiratory fitness based on the criteria of the Fitnessgram®. However, the sample here studied remained above the schoolchildren from the Vale do Cotinguiba (Sergipe, Brazil) studied by Petroski et al.16 Although with respect to Spanish 7–12 years old school children from Aragón, have shown to be equivalent.17
The investigation of morphological parameters becomes more relevant when detects possibilities of body fat accumulation, the emergence of chronic diseases and cardiovascular diseases. Malina and Bouchard18 emphasized that the female acquires greater gains of fat mass than boys from late childhood to late adolescence.
In this sense, the BF% (Table 1) of both groups were higher than those obtained by Dellagrana et al.19 and Hobold and Hübner.14 In this perspective, Lloyd et al.20 in students aged 10–12 years old from Texas – USA, found a BF% of 14.3 in males, at the same level of this study, although the female showed 8.5%, a value very below the results of this study. Despite variations, these results put the sample of this study far from risk of overweight and obesity according Fitnessgram® criteria.21 This evidence was corroborated by the parameters of the BMI (Fig. 1), which also report levels below normal.
Several studies22–25 over the past decade have reported the trend towards a minor cardiorespiratory fitness on female school students compared to their male counterparts. This phenomenon can be explained by sudden changes in body composition during puberty, particularly fat mass for girls.18 In addition to this, LaMonte et al.26 obtained that the maximal oxygen consumption is inversely proportional to BMI, in addition to other serum lipid parameters.
It was evidenced that the CRF of males was higher than females, while for the BMI, there were no differences between the groups. While most of the group remained in the normal range for BMI (79.9%), it drew attention to the high prevalence of the entire sample (50.8%) with poor performance for VO2max, particularly with respect to the female group, which 57.1% of them did not fit the health criteria adopted by Fitnessgram®. Furthermore, we proved the hypothesis of an inverse relationship between VO2max and BMI, in children and adolescents, a crucial period of life to develop these physical qualities.27
Because it is an important functional aspect, which if neglected in childhood and adolescence leads to extreme damage to health in adulthood, the result of this study on CRF requires specific attention by the government and educational authorities. It is well known the secular trend in the decline of this physical quality by several factors, including increased time spent in sedentary behaviors, like a high rate of exposure to television.28
This transition to sedentary lifestyle and its effects are strengthened by the phenomenon of urbanization of the society, as reported Chillón et al., 29 who studied spanish schoolchildren from antagonistic geographic areas, rural and urban, where lower levels of VO2max were found in the urban school children compared to their rural peers. Data from two cross-sectional studies in adolescents of 12.5-17.5 years old from Zaragoza (Spain) revealed an increase in CRF over 5 years.30 According to the authors, these data follow the opposite to the consistent decrease in cardiorespiratory fitness identified by studies around 27 countries and five geographic regions around the world.
The fact that the data from this study are aligned with the global trend is worrying, because low levels of this variable are related to risk of cardiovascular diseases, which begin in childhood and progress silently until adulthood, and are associated with a high number of deaths in some populations.22,31,32 The low performance of students from Aracaju (present study) on 20m shuttle-run test – only one boy for every ten (13.7% and one girl for every five (23.2%) met the cutoff points proposed by Fitnessgram® – contrasts with the results obtained by Guedes et al.,33 who found that about 50% on both boys and girls, reached health criteria. According to the authors, these results are not optimistic, especially because they observed a decline in proportion when increasing age, especially in physical tests that involve large muscle groups.
Usually, girls tend to be more affected by the advancement of puberty, as was also seen in Rodrigues et al.,34 who found an increase in aerobic power in men, from 43.5 to 49.5mlkg/min. However, similar to the present study, it was observed a decrease in values from 38.3 to 36.8mlkg/min on female, within the age range studied. In turn, 46.0% of students in Canoas (Rio Grande do Sul, Brazil)12 reached the zone of normality. Both studies corroborate the performance reached by the students from the present sample.
The development of estimative equations of CRF without exercise might be a low-cost alternative to applicate in the studies that involve large quantities of subjects, furthermore, it might provide a rapid diagnostic of the current status, mainly in physical education classes or before training program. However, these tools must be used carefully if the purpose is to predict more accurately VO2max in patients or athletes.35
In the present study it was also possible to identify how BMI exerted influence on VO2max values in males (R2=0.850) and females (R2=0.907). This evidence was also observed in Marques-Vidal and Dias36, who studied children in the same age than the present study, Monyeki et al.,37 in 14-year-old adolescents, Castro-Piñeiro et al.,38 in 6- to 17-year-old children and adolescents, Arruda et al.39, in children and adolescents participating in a sports project, and Botelho et al.,40 in which the higher the BMI, the lower the cardiorespiratory fitness and physical fitness in general.
It should be emphasized the study of Aires et al.,41 who evaluated 11- to 18-year-old boys and girls from Portugal. The authors obtained that the students in the range of overweight and obesity had lower levels of CRF, thereby confirming a negative correlation between high fat and VO2max, furthermore reaffirming that a sedentary lifestyle is a strong predictor of heart disease.
Although cross-sectional studies and the scores of field tests show relative limitation as to its reproducibility, as highlighted in the literature,42 they have been widely adopted as benchmarks for health-related physical fitness. Just as the Fitnessgram® tests battery, benchmarks such as Cole et al.43 and World Health Organization (WHO)44 play a key role, though Khadilkar et al.13 have emphasized the possible constraints in the adoption of their cutoff points due to the anthropometric changes in population over time and the hindering of the categorization of children and adolescents.
The findings of this study were explained to the managers of the Municipal Education from the city of Aracaju, in order to alert them of the need of the development of public policy towards the adoption of regular physical activities within the school community.
In conclusion, the data of the present study showed that CRF of boys was higher than the girls and there were no differences with respect to BMI. On the other hand, the BF% of the girls showed higher levels. On both sexes there were a minimal prevalence of schoolchildren at risk of overweight and obesity, according to the criteria proposed by Fitnessgram®. Relative to CRF, a high prevalence on both sexes behaved below the area related to health. The linear regression to estimate VO2max from BMI met expectations for studies on a population scale and confirmed an inverse relationship between both variables, which highlights the need of associate the parameters of physical fitness and health for an early diagnostic of exposure to physical inactivity, obesity and other cardiovascular risk factors.
Conflict of interestThe author declare not have conflict of interest.
