


The purpose was to investigate the factors related to aerobic fitness levels of adolescents in southern Brazil.
MethodsThe sample consisted of 1081 students (545 males and 536 females), with mean age of 12.8 (± 1.2) years. This is a cross-sectional epidemiological study. Aerobic fitness was assessed by the 9-min running test. The independent variables analyzed were: age, socioeconomic status, school system (public/private), sedentary behavior, physical activity level, nutritional status and body adiposity. Analyses were stratified by sex. We used the Student “t” test for independent samples and logistic regression to estimate odds ratio (OR) and confidence intervals of 95% (95% CI).
ResultsThe prevalence of low aerobic fitness levels was 92.5%. Boys aged 13–14 years were 2.44 times more likely to have low aerobic fitness levels; poorer boys were 4.31 times more likely to have low aerobic fitness levels. Girls aged 13–14 years were 5.35 times more likely to have low aerobic fitness levels; poorer girls were 10.70 times more likely to have low aerobic fitness levels; girls with sedentary behavior were approximately 4 times more likely to have low aerobic fitness levels.
ConclusionThus, it was concluded that almost all adolescents show low aerobic fitness levels, which makes necessary effective interventions in the school environment with the promotion of sports and regular practice of physical activity.
El presente estudio tuvo como objetivo investigar los factores relacionados con los niveles de aptitud aeróbica de los adolescentes en el sur de Brasil.
MétodosLa muestra estuvo conformada por 1081 alumnos (545 varones y 536 mujeres), con edad media de 12.8 (± 1.2) años. Se trata de un estudio epidemiológico transversal. La condición física aeróbica se evaluó mediante Test de Caminata de 9 minutos. Las variables independientes analizadas fueron: edad, nivel socioeconómico, el sistema escolar (público/privado), el sedentarismo, el nivel de actividad física, el estado nutricional y la adiposidad corporal. Los análisis fueron estratificados por sexo. Se aplicó la prueba de “t” Student para muestras independientes y regresión logística para estimar la odds ratio (OR) y los intervalos de confianza de 95% (IC95%).
ResultadosLa prevalencia de bajos niveles de aptitud aeróbica fue de 92.5%. Los niños de edades de 13 a 14 años fueron 2.44 veces más propensos a tener bajos niveles de condición física aeróbica; los niños más pobres fueron 4.31 veces más propensos a tener bajos niveles de condición física aeróbica. Las niñas de 13 a 14 años fueron 5.35 veces más propensas, a tener bajos niveles de condición física aeróbica; las niñas más pobres eran 10.70 veces más propensas a tener bajos niveles de condición física aeróbica; las niñas con el comportamiento sedentario, fueron aproximadamente 4 veces más propensas a tener bajos niveles de condición física.
ConclusiónSe concluyó que casi todos los adolescentes muestran bajos niveles de condición física aeróbica, lo que hace necesarias intervenciones eficaces en el ámbito escolar para la promoción del deporte y la práctica regular de actividad física.
O objetivo foi investigar os fatores relacionados aos níveis de aptidão aeróbia dos adolescentes no Sul do Brasil.
MétodosA amostra foi constituída por 1081 estudantes (545 do sexo masculino e 536 do sexo feminino), com idade média de 12.8 (± 1.2) anos. Este é um estudo epidemiológico transversal. Aptidão aeróbica foi avaliada pelo teste de corrida de 9 minutos. As variáveis independentes analisadas foram: idade, nível socioeconômico, sistema de escola (pública/privada), comportamento sedentário, nível de atividade física, estado nutricional e adiposidade corporal. As análises foram estratificadas por sexo. Foi utilizado o teste de Student “t” para amostras independentes e regressão logística para estimar odds ratio (OR) e intervalos de confiança de 95% (CI95%).
ResultadosA prevalência de baixos níveis de aptidão aeróbia foi de 92.5%. Meninos com idades entre 13-14 anos foram 2.44 vezes mais propensos a ter baixos níveis de aptidão aeróbia; meninos mais pobres eram 4.31 vezes mais propensos a ter baixos níveis de aptidão aeróbia. Meninas com idades entre 13-14 anos foram 5.35 vezes mais propensos a ter baixos níveis de aptidão aeróbia; as moças pobres foram 10.70 vezes mais propensas a ter baixos níveis de aptidão aeróbia; Meninas com comportamento sedentário foram aproximadamente 4 vezes mais propensas a ter baixos níveis de aptidão aeróbia.
ConclusãoAssim, concluiu-se que quase todos os adolescentes apresentam baixos níveis de aptidão aeróbica, o que faz intervenções eficazes no ambiente escolar com a promoção do desporto e da prática regular de atividade física necessária.
The lifestyle of children and adolescents has undergone modifications along the last decades. Part of the free time is occupied by sedentary activities, mainly related to the technological advancement and to the wide offer of electronic games.1,2 In addition, the decreased safety in streets and other public places in urban centers reduce the possibility of playing popular games that encourage physical activity.3 Such changes reflect in low physical activity levels among young people and, consequently, in low health-related physical fitness levels.4
Among the health-related physical valences, aerobic fitness is considered a protective factor for cardiovascular diseases such as type-2 diabetes mellitus, hypertension, atherosclerosis and metabolic syndrome.5 Reduced aerobic fitness among young people has been reported in some studies.6–8 In the U.S. state of Georgia, 52% of adolescents were below the healthy condition in relation to aerobic fitness.8
Recent studies investigating factors associated with aerobic fitness6–8 observed that adolescents who participated in sports and lived in rural areas had higher aerobic fitness levels. Some factors still need elucidation such as socioeconomic status that in some studies is directly associated with low aerobic fitness levels9 and in others, it is inversely proportional.10
Thus, considering the importance of investigating aerobic fitness in adolescents, since low levels of this physical fitness component in adolescence is associated with chronic diseases in adulthood11 and taking into account the possible association of this physical fitness component with sociodemographic factors in order to direct intervention actions in this population, this study aims to investigate factors related to aerobic fitness among adolescents in southern Brazil.
MethodPopulation and sampleThis cross-sectional study was approved by the Ethics Committee on Human Research of the “Extremo Sul Catarinense” University under protocol 225/2009. Adolescents who participated in the survey and parents/guardians signed the consent form authorizing their participation in the study.
The study was conducted at the city of Criciúma, southern Brazil, located in the Brazilian state of Santa Catarina, with human development index of 0.788, considered high, and life expectancy at birth of 75.8 years.12
The target population for this study consisted of 13508 elementary school students from Criciúma, Santa Catarina, Brazil. The sample size was calculated using an unknown prevalence for the outcome (50%), confidence level of 95%, estimated error of 5%, design effect of 2.0 and increment of 20% for losses and refusals. Given these parameters, a sample of 897 adolescents was estimated.
To ensure that the sample represented the target population, distribution considered school system (public and private), and school size (small, with fewer than 200 students; intermediate, with 200–499 students and large, with 500 students or more). The sample selection used the sampling procedure of clusters in two stages: the school was the sampling unit of the first stage and the classes were the sampling unit of the second stage. All schools in Criciúma with basic education were eligible for inclusion in the study. In the first stage, school density was adopted as stratification criterion, according to system and size, so proportionately more schools in the school system that had more schools and higher density were selected. In the second stage, the density of classes in the selected schools was considered as a criterion to draw those in which the questionnaires would be applied. All students in the selected classes were invited to participate in the study.
Data collection was conducted in the first half of 2010. Questionnaires were applied in classroom, without the presence of teachers. The evaluation team attended a previous training program for the standardization of data collection procedures. Physical fitness tests were performed in school gyms. For these tests, the students received oral explanation and demonstration of their execution.
The following inclusion criteria were used in the study: (a) students aged 10–14 years, (b) absence of health problems that prevent them from performing physical tests and anthropometric measurements. Adolescents who refused to participate and those who did not have the consent form signed by parents/guardians were considered refusals.
Dependent variableThe dependent variable of this study was aerobic fitness. The aerobic fitness was assessed by the 9-min running test of the American Alliance for Health, Physical Education, Recreation and Dance (AAHPERD),13 which has been validated for children14 and adolescents.15 Students were instructed to run the longest distance as possible in 9min. The test took place in school gymnasiums that were prepared for this test. Walking during the test was allowed, but the goal was to cover the longest distance as possible in 9min.
The distance was measured in meters, so that it was later dichotomized as “high” and “low” aerobic fitness levels. For this classification, the cutoff points described in the AAHPERD Manual13 were used, which establish the 50th percentile as the minimum level for adequate cardiorespiratory function. The cutoff points of AAHPERD13 are in yards and for the present study, they were transformed into meters (1 yard≅0.91m).
Independent variablesThe independent variables of this study were age in years, which was dichotomized into (10–12 years/13–14 years) and socioeconomic level, which was collected through instrument of the Brazilian Association of Research Companies.16 In this instrument, the population was divided into eight classes in decreasing order of purchasing power (A1, A2, B1, B2, C1, C2, D and E). In this study, A1 and A2 were grouped into “High”, B1 and B2 into “Intermediate” and C1, C2, D and E into “Low”. Another independent variable was school system (public/private).
Physical activity was analyzed by estimating the energy expenditure.17 The diary was applied in two days, one day of the week and one day of the weekend. In the diary, the adolescent recorded the physical activities carried out on that day every 15min. Daily activities are classified on a continuum involving nine categories, according to estimates of the average energy expenditure of activities performed by humans: (1) resting in bed; (2) activities performed in a sitting position; (3) light activities in a standing position; (4) activities that require light walking (<4km/h); (5) light manual work; (6) active leisure activities and recreational sports; (7) manual labor at a moderate pace; (8) active leisure activities and sports of moderate intensity; and (9) and heavy manual labor in competitive sports. This instrument provides reproducibility of r=0.91 in subjects from 10 years of age.17 In addition, the diary showed a correlation coefficient of 0.87 with the TriTrac accelerometer.18 From the recorded activities, the physical activity level was determined by estimating the daily energy demand in kilocalories per kilogram of body weight (kcal/kg/day), considering the energy equivalents of activities involving humans. There are no cutoff points for the classification of the physical activity level from the daily energy demand in literature. Therefore, the sample was classified according to the division into energy expenditure percentiles. Subjects who were below the 25th percentile were classified as insufficiently active. Students showing energy expenditure above the 25th percentile were considered physically active. Similar strategy to classify adolescents as for the physical activity level was adopted by Eisenmann et al.19 The goal of dividing into percentile is to compare the most active with the least active. The study does not aim to analyze adolescents who reach the recommended physical activity levels, because the instrument used does not have this feature.
Sedentary behavior was verified by time spent watching television in a common day of the week and weekend. The results of the week were added of a weight of five, equivalent to the days of the week and the results of the weekend were added of weight of two, dividing the total result by seven, thus obtaining the average per day. Sedentary risk behavior was considered as time spent watching TV more than 2h/day.20
The nutritional status was assessed by collecting weight and height21 and calculating the body mass index (BMI). International cutoff points for BMI,22 according to age and sex were used. This variable was dichotomized into normal weight and overweight (overweight+obesity).
Triceps and subscapular skinfolds were measured according to procedures described in literature,21 which were measured using scientific caliper brand Cescorf®, a Brazilian model that features design and mechanics similar to English Harpenden model, with supposed constant pressure on any opening of its rods of approximately 10g/mm2, measurement unit of 0.1mm and contact area (surface) of 90mm2. Excess peripheral (triceps skinfold) and central adiposity (subscapular skinfold) was rated based on a value corresponding to the 90th percentile of the reference distribution for sex and age according to the Centers for Disease Control and Prevention curve (CDC).23 This study examined the variable considering with excess general body adiposity adolescents who had both triceps and subscapular skinfold thickness values above the 90th percentile.23
Statistical analysisAnalyses were stratified by sex using the Stata 11.0 software. Descriptive and inferential statistics was used. The “t” test for independent samples was used to compare continuous variables between sexes. In crude and adjusted association analysis, Wald test and binary logistic regression were used to estimate odds ratio (OR) and confidence intervals of 95% (95%). Regression analysis followed a hierarchical model to determine low aerobic fitness level, hypothetically temporal, according to recommendations of Victora et al.24 Statistical analysis followed the division into three groups of variables: (a) distal, which included sociodemographic variables (age, socioeconomic status, school system), (b) intermediate, which included health-related behaviors (physical activity and sedentary behavior); (c) proximal, which included nutritional status and body adiposity. All variables were adjusted for analysis, regardless of p-value in the crude analysis.
The adjusted analysis adopted hierarchical approach, following the backward procedure. Initially, the adjustment was made for variables of the distal block to the other factors of the same level. Then, variables of the intermediate block were controlled for variables of the same level and for those of the distal level that remained in the model. Finally, variables of the proximal block were adjusted for the other factors of intermediate and distal levels that remained in the model. The criterion used for the maintenance of the factor in the regression analyses was p-value in the Wald test below 0.20.25 In addition, factors whose p-value was less than 0.05 were considered significantly associated with the outcome.
ResultsThe sample of this study consisted of 1081 students due to the characteristics of the sampling process, and all students present in the classroom during the period of data collection were invited to participate in the study. Of all adolescents, 545 were male and 536 were female, with mean age of 12.8 (± 1.2) years.
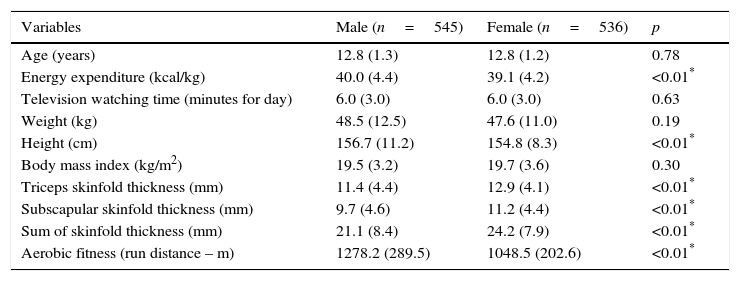
Males had higher values than females for energy expenditure, height and distance covered in the aerobic fitness test (p<0.05). On the other hand, females showed higher subscapular and triceps skinfold thickness values (Table 1).
Mean values and standard deviations of variables analyzed according to sex.
| Variables | Male (n=545) | Female (n=536) | p |
|---|---|---|---|
| Age (years) | 12.8 (1.3) | 12.8 (1.2) | 0.78 |
| Energy expenditure (kcal/kg) | 40.0 (4.4) | 39.1 (4.2) | <0.01* |
| Television watching time (minutes for day) | 6.0 (3.0) | 6.0 (3.0) | 0.63 |
| Weight (kg) | 48.5 (12.5) | 47.6 (11.0) | 0.19 |
| Height (cm) | 156.7 (11.2) | 154.8 (8.3) | <0.01* |
| Body mass index (kg/m2) | 19.5 (3.2) | 19.7 (3.6) | 0.30 |
| Triceps skinfold thickness (mm) | 11.4 (4.4) | 12.9 (4.1) | <0.01* |
| Subscapular skinfold thickness (mm) | 9.7 (4.6) | 11.2 (4.4) | <0.01* |
| Sum of skinfold thickness (mm) | 21.1 (8.4) | 24.2 (7.9) | <0.01* |
| Aerobic fitness (run distance – m) | 1278.2 (289.5) | 1048.5 (202.6) | <0.01* |
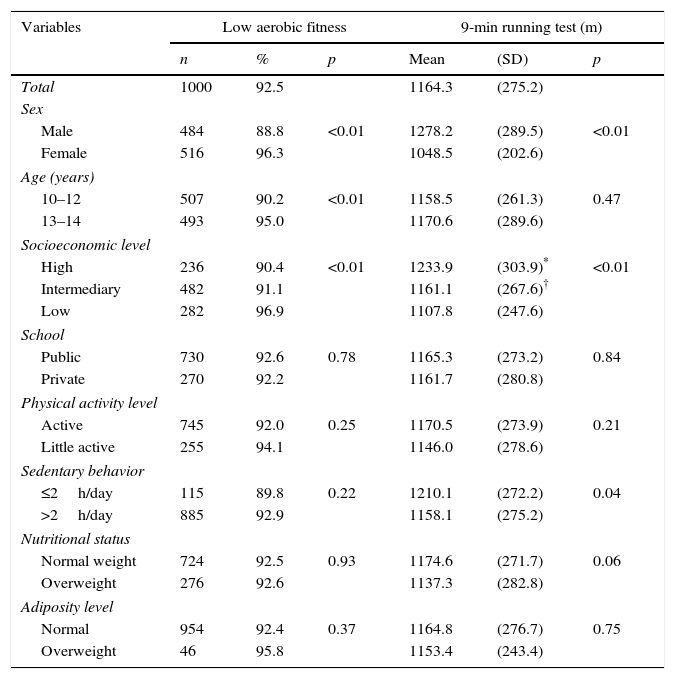
The prevalence of low aerobic fitness levels was 92.5%. This prevalence was higher among females, in those aged 13–14 years and in those with low socioeconomic level. Adolescents who covered the longest distance in the aerobic fitness test, those of higher economic level and those who watched fewer hours of TV per day were male (Table 2).
Prevalence of low aerobic fitness levels and mean values and standard deviation of the distance ran in the 9-min test according to independent variables.
| Variables | Low aerobic fitness | 9-min running test (m) | ||||
|---|---|---|---|---|---|---|
| n | % | p | Mean | (SD) | p | |
| Total | 1000 | 92.5 | 1164.3 | (275.2) | ||
| Sex | ||||||
| Male | 484 | 88.8 | <0.01 | 1278.2 | (289.5) | <0.01 |
| Female | 516 | 96.3 | 1048.5 | (202.6) | ||
| Age (years) | ||||||
| 10–12 | 507 | 90.2 | <0.01 | 1158.5 | (261.3) | 0.47 |
| 13–14 | 493 | 95.0 | 1170.6 | (289.6) | ||
| Socioeconomic level | ||||||
| High | 236 | 90.4 | <0.01 | 1233.9 | (303.9)* | <0.01 |
| Intermediary | 482 | 91.1 | 1161.1 | (267.6)† | ||
| Low | 282 | 96.9 | 1107.8 | (247.6) | ||
| School | ||||||
| Public | 730 | 92.6 | 0.78 | 1165.3 | (273.2) | 0.84 |
| Private | 270 | 92.2 | 1161.7 | (280.8) | ||
| Physical activity level | ||||||
| Active | 745 | 92.0 | 0.25 | 1170.5 | (273.9) | 0.21 |
| Little active | 255 | 94.1 | 1146.0 | (278.6) | ||
| Sedentary behavior | ||||||
| ≤2h/day | 115 | 89.8 | 0.22 | 1210.1 | (272.2) | 0.04 |
| >2h/day | 885 | 92.9 | 1158.1 | (275.2) | ||
| Nutritional status | ||||||
| Normal weight | 724 | 92.5 | 0.93 | 1174.6 | (271.7) | 0.06 |
| Overweight | 276 | 92.6 | 1137.3 | (282.8) | ||
| Adiposity level | ||||||
| Normal | 954 | 92.4 | 0.37 | 1164.8 | (276.7) | 0.75 |
| Overweight | 46 | 95.8 | 1153.4 | (243.4) | ||
(SD): standard deviation.
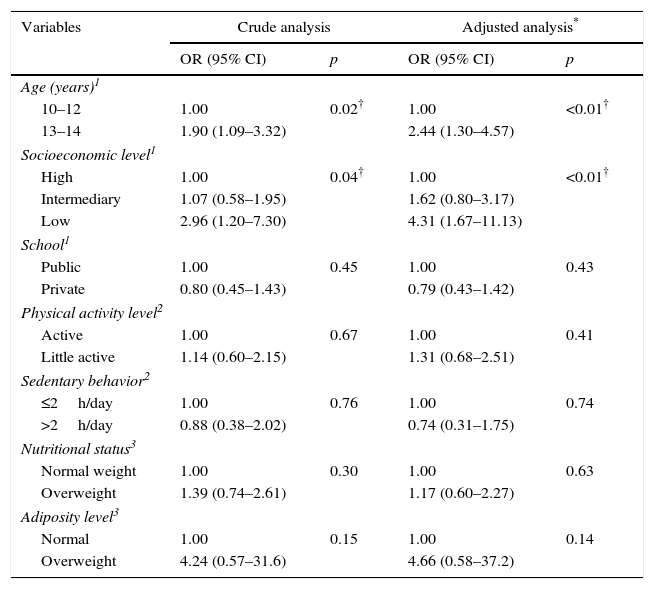
In the crude analysis, boys aged 13–14 years and those of low socioeconomic level were more likely to have low aerobic fitness levels. After adjustment, boys aged 13–14 years were 2.44 times more likely to have low aerobic fitness levels than younger boys; poorer boys were 4.31 times more likely to have low aerobic fitness levels than those of higher socioeconomic level (Table 3).
Crude and adjusted logistic regression analysis between low aerobic fitness levels and independent variables in male.
| Variables | Crude analysis | Adjusted analysis* | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age (years)1 | ||||
| 10–12 | 1.00 | 0.02† | 1.00 | <0.01† |
| 13–14 | 1.90 (1.09–3.32) | 2.44 (1.30–4.57) | ||
| Socioeconomic level1 | ||||
| High | 1.00 | 0.04† | 1.00 | <0.01† |
| Intermediary | 1.07 (0.58–1.95) | 1.62 (0.80–3.17) | ||
| Low | 2.96 (1.20–7.30) | 4.31 (1.67–11.13) | ||
| School1 | ||||
| Public | 1.00 | 0.45 | 1.00 | 0.43 |
| Private | 0.80 (0.45–1.43) | 0.79 (0.43–1.42) | ||
| Physical activity level2 | ||||
| Active | 1.00 | 0.67 | 1.00 | 0.41 |
| Little active | 1.14 (0.60–2.15) | 1.31 (0.68–2.51) | ||
| Sedentary behavior2 | ||||
| ≤2h/day | 1.00 | 0.76 | 1.00 | 0.74 |
| >2h/day | 0.88 (0.38–2.02) | 0.74 (0.31–1.75) | ||
| Nutritional status3 | ||||
| Normal weight | 1.00 | 0.30 | 1.00 | 0.63 |
| Overweight | 1.39 (0.74–2.61) | 1.17 (0.60–2.27) | ||
| Adiposity level3 | ||||
| Normal | 1.00 | 0.15 | 1.00 | 0.14 |
| Overweight | 4.24 (0.57–31.6) | 4.66 (0.58–37.2) | ||
OR: odds ratio; CI: confidence interval.
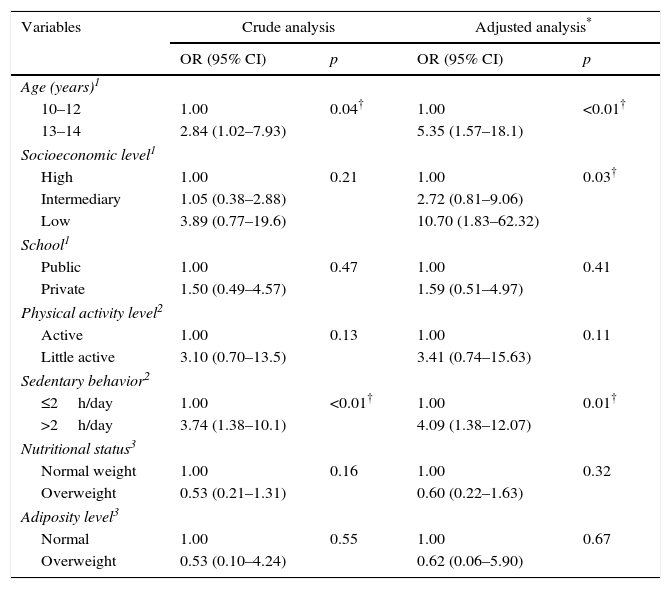
In the crude analysis, girls aged 13–14 years and those with sedentary behavior were more likely to have low aerobic fitness levels. After adjustment, girls aged 13–14 years were 5.35 times more likely to have low aerobic fitness levels than those aged 10–12 years; poorer girls were 10.70 times more likely to have low aerobic fitness levels than those of higher socioeconomic level and those showing sedentary behavior were approximately 4 times more likely to have low aerobic fitness levels than those without sedentary behavior (Table 4).
Crude and adjusted logistic regression analysis between low aerobic fitness levels and independent variables in female.
| Variables | Crude analysis | Adjusted analysis* | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age (years)1 | ||||
| 10–12 | 1.00 | 0.04† | 1.00 | <0.01† |
| 13–14 | 2.84 (1.02–7.93) | 5.35 (1.57–18.1) | ||
| Socioeconomic level1 | ||||
| High | 1.00 | 0.21 | 1.00 | 0.03† |
| Intermediary | 1.05 (0.38–2.88) | 2.72 (0.81–9.06) | ||
| Low | 3.89 (0.77–19.6) | 10.70 (1.83–62.32) | ||
| School1 | ||||
| Public | 1.00 | 0.47 | 1.00 | 0.41 |
| Private | 1.50 (0.49–4.57) | 1.59 (0.51–4.97) | ||
| Physical activity level2 | ||||
| Active | 1.00 | 0.13 | 1.00 | 0.11 |
| Little active | 3.10 (0.70–13.5) | 3.41 (0.74–15.63) | ||
| Sedentary behavior2 | ||||
| ≤2h/day | 1.00 | <0.01† | 1.00 | 0.01† |
| >2h/day | 3.74 (1.38–10.1) | 4.09 (1.38–12.07) | ||
| Nutritional status3 | ||||
| Normal weight | 1.00 | 0.16 | 1.00 | 0.32 |
| Overweight | 0.53 (0.21–1.31) | 0.60 (0.22–1.63) | ||
| Adiposity level3 | ||||
| Normal | 1.00 | 0.55 | 1.00 | 0.67 |
| Overweight | 0.53 (0.10–4.24) | 0.62 (0.06–5.90) | ||
OR: odds ratio; CI: confidence interval.
The main findings of this study showed that adolescents of both sexes, aged 13–14 years and of lower socioeconomic status were more likely to have low aerobic fitness levels. Furthermore, it was found that girls with sedentary behavior were less aerobically fit.
The prevalence of low aerobic fitness levels was 92.5% among adolescents investigated in the present study, a result higher than that found in Florianópolis, capital of Santa Catarina, Brazil (64.9%).10 In a study conducted in Europe by Cuenca-García et al.,26 the prevalence of adolescents with low aerobic fitness levels was 30.9%. In American children from California, approximately 45% of students had inadequate aerobic fitness levels.27 Through comparisons, it was observed that the results of this study indicate a high prevalence of low aerobic fitness levels. However, these comparisons should be made with caution, because the different field tests and cutoff points used in the aforementioned studies may explain the discrepancies found in terms of prevalence. A survey that used the same test and the same cutoff points used in the current study was conducted by Pelegrini et al.2 with data from 7507 students from seven to 10 years of age from all geographical regions. The authors found that approximately 80% of children had low aerobic fitness levels.2
The study by Aryana et al.9 with 8.4 million students from public schools in California showed results similar to the present study, in which for both sexes, worse aerobic fitness levels were found for children of low socioeconomic status. According to the study,9 adolescents who lived in cities with higher unemployment rates and lower incomes were more likely to have low aerobic fitness level when compared to their peers in more favorable conditions. Dissimilar results were revealed by Vasques et al.,10 who investigated adolescents of Brazil's capital with the highest human development index. The discrepancy between the results of this study and those revealed by Vasques et al.10 may be due to the difference between cities in which the studies were carried out. This study was conducted in a small town with characteristics different from those of cities with the highest HDI. In more developed cities, the problem of urban violence and lack of physical space for physical activity is more frequent, resulting in the participation of adolescents in sports activities developed at clubs and gyms, places of easy access to those of higher socioeconomic level. On the other hand, small urban centers, as in the present study, most physical activities occur outdoors.2
With respect to the lower aerobic fitness level in adolescents aged 13–14 years when compared to their younger peers, it could be inferred that this trend is similar to results found by Chillón et al.,7 since the VO2max results (mL/kg per min) among adolescents were lower than the values obtained for children of both sexes. The literature reveals that as adolescents grow older, their engagement in physical activities decreases, which can result in low health-related physical fitness levels.1
The female students in this study that were more likely to have low aerobic fitness levels were those who spent more hours watching of TV/day. Similar result was also found by Mota et al.4 in a two-year longitudinal study conducted with students from Portugal. This convergence of results points to an inverse relationship between these variables (time watching TV and aerobic fitness). Thus, initiatives in the school environment demonstrating the need for a reduction in sedentary behavior can have an effect on stimulating the regular practice of physical activities and improving aerobic fitness.
It is noteworthy that this study has some limitations such as the impossibility of knowing whether volunteers did their best in the aerobic fitness test. However, procedures to ensure standardization during the performance of the field test were adopted, which reinforces their reproducibility. In addition, the cutoff points adopted to characterize low aerobic fitness levels are from a sample of American adolescents, who have different life habits compared to Brazilians. The outcome and the exposures were collected at the same time, which does not allow establishing a causal relationship. All these limitations may have reflected the lack of association between low aerobic fitness levels and excess body fat, which is widely reported in literature.5
Despite the limitations described, this work was developed with a significant sample of adolescents of a city in southern Brazil and aimed to identify related factors such as socioeconomic status, which still does not have consensus in terms of association with aerobic fitness.
It is concluded that more than 90% of adolescents had low aerobic fitness levels, and this prevalence is higher among females. In both sexes, subjects who require special attention to increase the aerobic fitness levels are older adolescents, those with low socioeconomic status and girls with sedentary risk behavior. Further studies on this topic should be carried out in order to elucidate other factors associated with aerobic fitness that were not investigated in this study such as macroeconomic factors related to the environment in which adolescents live and free access to sports practice. Moreover, there is need to investigate whether Physical Education classes are sufficient to stimulate and improve the health-related physical fitness levels of children.
Conflicts of interestThe authors have no conflicts of interest to declare.
