


Eighteen years after ICPD (Cairo, 1994), unsafe abortion (UA), contemplated thereby as a serious Public Health issue, persists in Brazil. This research, conducted in a slum in the outskirts of São Paulo by means of a cross-sectional study, intended estimating the prevalence of women who have had unsafe abortions, identifying the socio-demographic characteristics (SDC) related thereto, and their morbidity. This article refers to the SDC, the variables of which remained in the final model of the Multiple Multinomial Logistic Regression analysis carried out therefor - age at 1st sexual intercourse, number of partners, schooling, ethnicity/color, marital status and abortion acceptance driven by low-income conditions–with an approach intended for the social determinants of health and for the health inequities generated thereby in the case of UA, in an impoverished population. In conclusion, the UA and SDC are influenced by the SDH, creating health inequities in that population. The greatest proportion of women that induced unsafe abortion within this population was represented by black women, with lower income, with less than 4 years of school attendance and single, which indicates health inequalities and inequities.
Após 18 anos da CIPD, Cairo, 1994, a situação do Aborto Inseguro (AI), nela contemplado como um grave problema de Saúde Pública, permanece a mesma no Brasil. Esta pesquisa, um estudo transversal, realizada em uma favela da periferia de São Paulo, teve como objetivos estimar a prevalência de mulheres com aborto inseguro, identificar as características sociodemográficas (CSD) a ele associadas, e sua morbidade. São discutidas neste artigo as CSD cujas variáveis permaneceram no modelo final da análise de Regressão Logística Multinomial Múltipla efetuada com essa finalidade - idade da 1ª relação sexual, número de parceiros, escolaridade, etnia/cor, estado civil e aceitação do aborto por falta de condições econômicas - com uma abordagem voltada aos determinantes sociais e às iniquidades em saúde por esses geradas na ocorrência do AI, em uma população em situação de pobreza. A maior proporção de mulheres que provocaram aborto inseguro nesta população foi a de mulheres de cor preta, com renda mais baixa, menos de 4 anos de estudo e solteiras, o que demonstra a presença de desigualdades e iniquidades em saúde.
Women who face unintended or unplanned pregnancies are left with two difficult options: either give birth to an unwanted child, at least on that particular moment, or terminate pregnancy, inducing abortion. In countries where abortion is permitted by law, it is a safe procedure, practically risk-free; in countries where law is restrictive, abortion becomes unsafe.1
Unsafe abortion is defined as a procedure for terminating an unintended pregnancy either by people lacking the necessary professional skills or in an environment lacking the minimal medical standards, or both.2
Unsafe abortion is a serious Public Health issue acknowledged by the international scientific community at conferences organized by the United Nations in the 1990's. In countries where abortions are clandestine and unsafe, their consequences to women's health are harmful, in particular as regards young, poor and low-education women, not disregarding their impact on the local public health services.3–5
The World Health Organization (WHO) estimates that, each year, 20 million abortions occur worldwide in inadequate conditions2 and that between 10% and 50% of women that have abortion require medical care for complications. Therefore, unsafe abortion is a serious health hazard.
Most abortions carried out in risk conditions or unsafe abortions take place in developing or poor countries, in which abortions are restricted by law. In 2003, 97% of all unsafe abortions took place in developing countries, such as Brazil.6
Unsafe Abortion (UA) is the main cause for Maternal Mortality in Latin America and in the Caribbean.7 Approximately 21% of maternal deaths in that region result from complications related to clandestine abortions.2 It is also in that region that the highest rate of clandestine and unsafe abortions is recorded, 37/1,000.8 It is estimated that deaths resulting from abortions carried out in risk conditions total 30 to 100,000lb in Latin America, with an unsafe abortion case-fatality rate of 220/100,000 abortions, i.e., 0.22%, which means that out of one thousand procedures, at least two maternal deaths are expected, which constitutes a rate 350 times higher than the safe abortion case-fatality rate that, in turn, is insignificant.9
The total number of unsafe abortions in Brazil is estimated to be between 750,000 and 1,500,000 a year, if the methodology proposed by the Alan Guttmacher Institute to estimate the number of clandestine abortions is applied to the Brazilian data of 2000, solely taking into consideration the data on hospital admissions in the Brazilian Public Health Care System (Sistema Único de Saúde - SUS). Such methodology involves a correction factor and takes into account solely the cases of abortions that end up requiring hospitalization, which may represent solely one third to one fifth of the total number of voluntary abortions, for most women do not arrive at the hospitals in time. The same Institute estimated an amount of 4 million clandestine and unsafe abortions a year for Latin America and the Caribbean.10
Among the causes of maternal mortality in Brazil, unsafe abortion currently occupies the fourth place; nevertheless, it is known that unsafe abortion may be also included between the two causes that precede it–hemorrhagic syndromes and puerperal infections–which would make it, in fact, the third cause of maternal death for rarely is its occurrence referred to in the death certificate. Furthermore, clandestinity brings forth limitations for the diagnosis of abortion induced during the medical care, frequently hindering to the appropriate registration of abortion, worsening the already precarious manner in which the death certificate is frequently filled out.11 In view of the fact that induced abortion is a crime under the criminal code and in view of other deficiencies of the system to notify maternal deaths, a significant part is not registered even though maternal deaths must be registered since 1997.12 Deaths caused by abortions are preventable and avoidable.13
Most deaths resulting from abortion affect young, Afro-descendant, single or judicially separated women. The Maternal Mortality Ratio (MMR) per abortion, for Afro-descendant women (brown and black), was 11.28/100 thousand live births, twice the MMR for white women, from 1999 to 2002, indicating a high index of social injustice and health inequities.14 The maternal mortality risks are twice as higher for black women than for white women. If we take into account the MMR as a result of pregnancies ending in abortion, such relative difference is higher: black women support 2.5 times more risks than white women do.15
“Abortion is a public health issue and a social justice subject, for women with financial resources receive safe care and on occasion of different vulnerabilities, they recur to unsafe abortion”.14 Studies on clandestine abortions in contexts in which abortions are strictly restricted by law indicate that women with higher income present higher probability of success at inducing a safe abortion than those with lower income.1
The determinants of unsafe abortion include the legislative restriction on abortion, limited social support to this problem, inadequacy of family planning services and unsatisfactory infrastructure of health services.13
The social determinants of health (SDH) play an important role in the outcome of unintended or unplanned pregnancies. Women in social disadvantage are more likely to experiment unintended pregnancy than women with more financial and social resources.1
The main social determinant of recurrence of unsafe abortion is the legal, actual or perceived restriction to safe abortion. Developing countries are more likely to restrict access to legal abortion than developed countries, and such restriction disproportionately affects lower-income women, giving rise to health inequities.1
Brazil still faces shortage of epidemiological studies on unsafe abortion, in vulnerable low-income populations in which abortion plays an essential role in the maternal morbidity and mortality rates and in which there is greater need to work on the preventive family planning issue as one of the main issues inherent to reproductive health.12 It is further not yet sufficiently established to which social determinants of health those populations become more vulnerable, i.e., specifically to unsafe abortion or to the hazards to women health. Therefore, the purposes of this study were to estimate prevalence of unsafe abortion, identify the social-demographical characteristics (SDC) related thereto, and morbidity, with an approach focused on the social determinants of abortion and on health inequities, in a poverty stricken population.
Material and methodsThis is a cross-sectional study in which all women aged between 15–54 years old, resident in a slum of the North district of the City of São Paulo, were interviewed. Out of 382 women who reside in that location and belong to that age group, 375 women were interviewed and 7 (1.8%) refused to take part in the study.
Data has been collected by means of structured interviews, directly, by experienced interviewers, at the domicile of the women interviewed. The instrument of collection includes three elements gathered in one: Family Composition (with monthly household per capita income (PCI); Structured and pre-coded questionnaire, for collection of socio-demographic data; and Pregnancies’ History (with attachment on complications related to abortion and hospital admissions).
The interviews have been conducted by three community monitors and three college students majoring in Human Science that, subsequently to being submitted to training in offices, conducted the interviews by means of visits to the domicile of the women of that population, scheduled according to the availability of the women interviewed. This procedure has been previously tested in a pilot group and there was supervision during the entire data collection process. Women have been encouraged to take part in the survey, and not only absolute secrecy about the information gathered has been guaranteed thereto, but also the identification of the women interviewed has not been required.
The dependent variable Abortion was divided into 3 categories: NA/LB (no abortion or only live births), SA (spontaneous abortion) and IA (induced abortion). The independent variables were: age at 1st sexual intercourse; marital status on the occasion of 1st event; color/ethnicity; origin (State of São Paulo or other states); religion; remunerated activity; per capita income (divided into 2 categories with cut-off point based on average); educational level (low, up to 4 years of school attendance and not low, more than 4 years of school attendance); number of partners informed in the last year prior to the survey; use of contraceptives in each pregnancy; gap LB-IN (difference between the number of live-births and the ideal number of children in which the following categories were established: lower, whenever the number of live births is lower than the number of children informed as ideal (LB<IN); equal, whenever the figures of the two variables are equal (LB=IN); higher, whenever there are more live births than what is deemed ideal (LB>IN).
In addition to those variables, abortion acceptance level was investigated, procedure in which the following events were analyzed: non-acceptance of abortion and, in the event of acceptance, the reasons analyzed were - fetal malformation, mother's risk of death, mother's health problems, rape, lack of economical conditions, family already complete, single mother, separated mother, and mother's intention of not having any more children.
The Analysis of Data was carried out for 2 groups: one group with Total Women (TW) interviewed and the other group with Total Women that mentioned previous Pregnancy (TWP), with exception to 97 women that have never become pregnant.
Note: This article focuses on the 278 women of that population that have had at least one pregnancy (TWP).
Primarily, prevalence of abortion–induced and spontaneous–was calculated among women aged 15 to 54 years old, resident in the community. To analyze the data, the chi-square distribution or the Fisher association test, the Kruskal-Wallis test (for PCI) and univariate and multiple multinomial logistic regression models were used, and the reference category was variable NA/LB. The variables that indicated associations with p<0.20 were selected to enter an initial model of Multiple Multinomial Logistic Regression (MMLR) by the stepwise backward method. In all analyses, the association statistically significant was taken into consideration when p <0.05. The statistical analysis of data was carried out with assistance from software SPSS 16.0 for Windows, using two Databases generated from two structural units: one per Individual and another one per Pregnancy.
Both stages of this study were approved by the Research Ethics Committee of UNIFESP (CEP 1300/06 and 0990/10).
ResultsA high rate of abortions was verified - 144 abortions in a population of 375 women, out of which 93 suffered or induced abortion, which corresponds to a prevalence of 24.8. Eighty-two (82) out of 144 abortions, related to 51 women (18.34% in TWP group) were confirmed as induced (IA), and sixty-two (62) abortions, related to 42 women (15.1%), were confirmed as spontaneous (SA). The mean number of abortions per woman was 1.55 abortions.
All induced abortions were clandestine and unsafe for having been induced at the very own household of the women interviewed, in locations with no hygiene conditions whatsoever, with no asepsis, with no follow-up of any type, and by the pregnant women themselves or by individuals lacking the minimum professional skills.
It is very much possible that a large number of omitted induced abortions are among the abortions confirmed as spontaneous. Nevertheless, this survey, for a matter of methodological strictness, considered unsafe abortions only those confirmed as induced (IA=UA).
As regards income, the assessed per capita income (PCI) was the current monthly household PCI. The PCI means, for women that informed the PCI, were distributed as follows:
- •
PCI of women with No Abortions=R$241.00
- •
PCI of women with Spontaneous Abortion=R$232.10
- •
PCI of women with Induced Abortion=R$173.60 (< 1/2 MW - minimum wage)
*PCI is significantly lower for group IA from the statistical point of view, with p=0.017 and mean lower than half a minimum wage (MW).
The mean age of women related to all abortions (SA and IA) was 23.1 years old. The age average of women at their first IA was lower, i.e., 21.6 years old, who further had the age average of 17.7 years old at their first pregnancy. Only 33.3% of women had their first IA at 1st pregnancy and 66.6% induced abortion in subsequent pregnancies.
At 24 years old, more than 70% of the women had already had their first IA (50% of the women had their 1st IA before 20 years old). More than 50% of the women started their sexual lives between 11 and 16 years old; out of the women who had abortions (SA and IA), 52% did so.
Percentage of Interrupted Pregnancies=37.3% at WA (W with history of Abortion)
Pregnancies’ mean: group 1 (with abortion)=4.15
group 0 (no abortion)=2.4
Pregnancies–age group: 13–41 years old
Approximately 70% of women that induced unsafe abortion did not use contraceptives on the occasion of pregnancies.
A high index of morbidity was also verified as a result of complications related to unsafe abortion–94.12%, resulting in 83.3% of admissions in public hospitals.
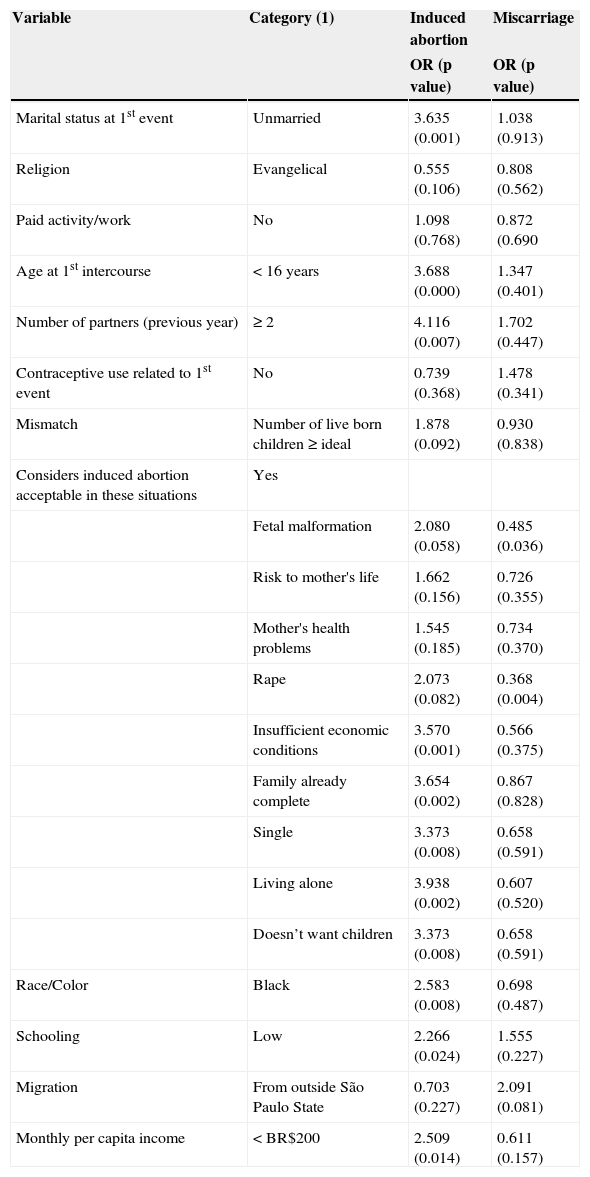
Table 1 indicates the results of the univariate analyses for group TWP.
Univariate analysis of variables (socio-demographic characteristics) associated with induced abortion and miscarriage for the sample of women with history of pregnancy.
| Variable | Category (1) | Induced abortion | Miscarriage |
|---|---|---|---|
| OR (p value) | OR (p value) | ||
| Marital status at 1st event | Unmarried | 3.635 (0.001) | 1.038 (0.913) |
| Religion | Evangelical | 0.555 (0.106) | 0.808 (0.562) |
| Paid activity/work | No | 1.098 (0.768) | 0.872 (0.690 |
| Age at 1st intercourse | < 16 years | 3.688 (0.000) | 1.347 (0.401) |
| Number of partners (previous year) | ≥ 2 | 4.116 (0.007) | 1.702 (0.447) |
| Contraceptive use related to 1st event | No | 0.739 (0.368) | 1.478 (0.341) |
| Mismatch | Number of live born children ≥ ideal | 1.878 (0.092) | 0.930 (0.838) |
| Considers induced abortion acceptable in these situations | Yes | ||
| Fetal malformation | 2.080 (0.058) | 0.485 (0.036) | |
| Risk to mother's life | 1.662 (0.156) | 0.726 (0.355) | |
| Mother's health problems | 1.545 (0.185) | 0.734 (0.370) | |
| Rape | 2.073 (0.082) | 0.368 (0.004) | |
| Insufficient economic conditions | 3.570 (0.001) | 0.566 (0.375) | |
| Family already complete | 3.654 (0.002) | 0.867 (0.828) | |
| Single | 3.373 (0.008) | 0.658 (0.591) | |
| Living alone | 3.938 (0.002) | 0.607 (0.520) | |
| Doesn’t want children | 3.373 (0.008) | 0.658 (0.591) | |
| Race/Color | Black | 2.583 (0.008) | 0.698 (0.487) |
| Schooling | Low | 2.266 (0.024) | 1.555 (0.227) |
| Migration | From outside São Paulo State | 0.703 (0.227) | 2.091 (0.081) |
| Monthly per capita income | < BR$200 | 2.509 (0.014) | 0.611 (0.157) |
Reference category: no abortion.
For the total number of women with history of previous pregnancy (TWP), in relation to IA, the following variables indicated significant associations: single; black ethnicity/color; low educational level; per capita income lower than R$200.00; age at 1st sexual intercourse: younger than 16 years old; had 2 or more partners in the year prior to the survey; and the situations surveyed in relation to acceptance of abortion as regards lack of economical conditions, family already complete, single mother, separated mother and mother's intention not to have any more children. In relation to SA, there were no significant associations for that group (Table 1).
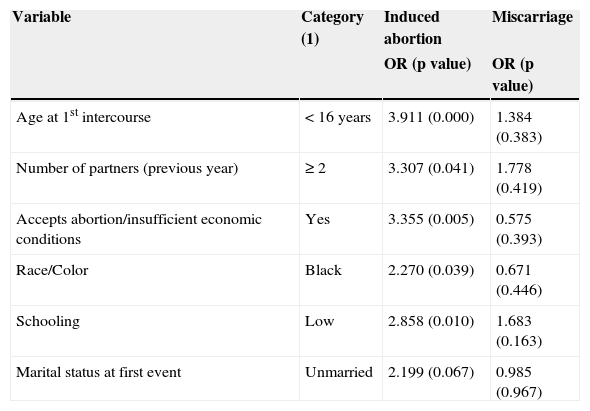
As regards the final models of MMLR, after removing, one by one, the variables that declined in importance, there were 6 variables left, which were statistically significant to group TW, out of which 5 remained in the group TWP (Table 2). The following variables remained for the final model of TWP IA/UA–Table 2: age at first sexual intercourse: younger than 16 years old (OR=3.91; p<0.001); number of partners: more than 2 in the last year (OR=3.31; p=0.041); acceptance of abortion for lack of economical conditions (OR=3.35; p=0.005); black ethnicity/color (OR=2.27; p=0.039); and low educational level (OR=2.86; p=0.010). The variable marital status to the 1st event, category not married, although marginally significant (OR=2.2; p=0.67), remained in the model in light of its relevance in the specialized literature. The variable gap (LB - ideal), category 1–having a number of children LB>ideal (OR=3.09; p=0.008), present in the final model for TW, lost statistical strength and did not remain in this model. As for SA, none of the variables indicated significant association.
Multivariate analysis of variables (socio-demographic characteristics) associated with induced abortion and miscarriage for the sample of women with history of pregnancy.
| Variable | Category (1) | Induced abortion | Miscarriage |
|---|---|---|---|
| OR (p value) | OR (p value) | ||
| Age at 1st intercourse | < 16 years | 3.911 (0.000) | 1.384 (0.383) |
| Number of partners (previous year) | ≥ 2 | 3.307 (0.041) | 1.778 (0.419) |
| Accepts abortion/insufficient economic conditions | Yes | 3.355 (0.005) | 0.575 (0.393) |
| Race/Color | Black | 2.270 (0.039) | 0.671 (0.446) |
| Schooling | Low | 2.858 (0.010) | 1.683 (0.163) |
| Marital status at first event | Unmarried | 2.199 (0.067) | 0.985 (0.967) |
Reference category: no abortion.
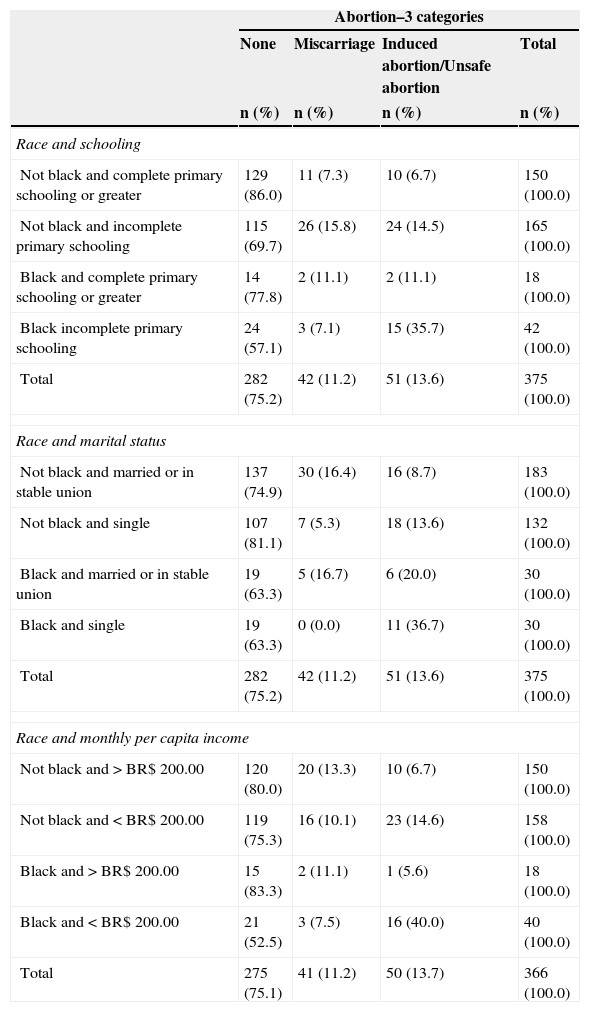
To assist with the survey on the social determinants of unsafe abortion and health inequities, an epidemiological interaction between variable ethnicity/color and variables educational level, marital status and income was analyzed (Table 3). There was strong statistical association between these interactions and IA/UA. Considering ethnicity/color and educational level, the highest proportion of women with IA (35.7%) occurred among black women with elementary school incomplete. Similar proportion (36.7%) was verified among black and single women and among black women with income below R$200.00 (40.0%). The lowest proportions of women with IA were verified among non- black women with elementary school or higher complete (6.7%), among non- black and married/united women (8.7%), and among non-black women with income above R$200.00 (6.7%).
Prevalence (%) of women with miscarriage and induced abortion/unsafe abortion in the total sample of women according to race/color.
| Abortion–3 categories | ||||
|---|---|---|---|---|
| None | Miscarriage | Induced abortion/Unsafe abortion | Total | |
| n (%) | n (%) | n (%) | n (%) | |
| Race and schooling | ||||
| Not black and complete primary schooling or greater | 129 (86.0) | 11 (7.3) | 10 (6.7) | 150 (100.0) |
| Not black and incomplete primary schooling | 115 (69.7) | 26 (15.8) | 24 (14.5) | 165 (100.0) |
| Black and complete primary schooling or greater | 14 (77.8) | 2 (11.1) | 2 (11.1) | 18 (100.0) |
| Black incomplete primary schooling | 24 (57.1) | 3 (7.1) | 15 (35.7) | 42 (100.0) |
| Total | 282 (75.2) | 42 (11.2) | 51 (13.6) | 375 (100.0) |
| Race and marital status | ||||
| Not black and married or in stable union | 137 (74.9) | 30 (16.4) | 16 (8.7) | 183 (100.0) |
| Not black and single | 107 (81.1) | 7 (5.3) | 18 (13.6) | 132 (100.0) |
| Black and married or in stable union | 19 (63.3) | 5 (16.7) | 6 (20.0) | 30 (100.0) |
| Black and single | 19 (63.3) | 0 (0.0) | 11 (36.7) | 30 (100.0) |
| Total | 282 (75.2) | 42 (11.2) | 51 (13.6) | 375 (100.0) |
| Race and monthly per capita income | ||||
| Not black and>BR$ 200.00 | 120 (80.0) | 20 (13.3) | 10 (6.7) | 150 (100.0) |
| Not black and<BR$ 200.00 | 119 (75.3) | 16 (10.1) | 23 (14.6) | 158 (100.0) |
| Black and>BR$ 200.00 | 15 (83.3) | 2 (11.1) | 1 (5.6) | 18 (100.0) |
| Black and<BR$ 200.00 | 21 (52.5) | 3 (7.5) | 16 (40.0) | 40 (100.0) |
| Total | 275 (75.1) | 41 (11.2) | 50 (13.7) | 366 (100.0) |
p<0.001 for the 3 analyses.
Health inequalities may be defined as differences in health conditions or in the distribution of their determinants among different population groups. Whenever they give rise to inequity, they refer to health inequities.16 The main determinants of such inequities are related to how social life is structured. Health inequities among groups and individuals must be considered avoidable, unfair and unnecessary.16
People who are vulnerable and at social risk, belonging to families with per capita income of up to half a minimum wage, in Brazil, are considered affected by poverty and social exclusion by the Ministry of Social Development of the Government. They belong to “populations in poverty and indigence” and are the greatest victims of social inequality.17 Even though the best index of assessment of such situation is the HDI (Human Development Index), it is hard to apply such index to small populations, for it involves knowledge of other indicators that are not always available. For the time being, the HDI has solely been used for countries, states and municipalities.
One of the immediate effects generated by social inequality is the high level of vulnerability of youngsters belonging to families with minimum income, which is not sufficient to lead a dignified life. Such youngsters suffer a process of social exclusion, varying in intensity.
The Per Capita Income (PCI) of the population enquired, assessed based upon the Family Composition Table and acknowledged on the occasion of the interview for subsequent calculation, was the monthly house PCI of 2005. It is not possible to have access to the PCI related to the moment of each event; however, based upon statements, it is possible to acknowledge that such PCI was much lower, especially among women with induced abortion.
Education, in a way, represents the income whenever income cannot be measured (therefore its doubled relevance).12
The complex relationship between education and other demographical characteristics, preferences in fertility, contraception and abortion is reflected in the significantly different standards observed in the few studies in which such information is available.18
As an example of the indirect effects of education on pregnancies and abortion, the use of contraceptives is closely related to the level of instruction of women. In that sense, women with higher levels of education have better knowledge of contraceptive methods and, therefore, may select the most effective ones, unlike less instructed women.19 Approximately 70% of women from Inajar slum that induced unsafe abortion did not use contraceptives on the occasion of pregnancies.12
The National Survey on Demography and Health–1996,20 conducted by BEMFAM with adolescents aged 15 to 19 years old, indicated that, among young women that became pregnant at least once (TWP), 54% of them had practically no instruction and 6% had 9 to 11 years of school attendance, indicating “an inverse relation between level of education and pregnancy of adolescents”.20
Results of the survey conducted at Inajar slum indicated that, as for the TWP group, women with less than 4 years of school attendance have three times more probability than the other ones to induce unsafe abortion. As regards the group of women with IA, there was a very high concentration (68.6%) of women with incomplete elementary school, which, if added to the proportion of illiterate women, results in 75% of women with low level of education or lower than 4 years of school attendance. Results differing from the results of this survey concerning associating low level of education and IA result from studies conducted with women belonging to other socioeconomic and/or regional realities.21,22
The ethnicity/color variable further indicates an interaction with income for the population surveyed, as well as with the instruction level and with marital status. Generally speaking, “as far as health conditions are concerned, differences between blacks and whites are notable”.23
The ethnicity prevailing in a surveyed population may solely be detected by measuring the number of women of a certain color, self-classified and self-declared. In doubt, this population has been inquired about family kinship.24
In 2000, according to the census data, the Brazilian black population corresponded to 45% of the total population. Nevertheless, blacks represent 63% of the poor population, among which women are majority.25
Black women (Afro-descendants) in Brazil have less access to education, live in worse living and housing conditions, have less access to contraceptive methods and have greater chances of becoming pregnant, even if not desired thereby.26 Thus, the North, Northeast and Midwest regions concentrate the highest rates of black women deaths as a result of problems in the puerperal pregnancy cycle (pregnancy, delivery and puerperium), including abortion, as well as the highest rates of maternal deaths.27
Results obtained at Inajar slum in relation to color/ethnicity are consistent with literature. Epidemiological interaction demonstrated that women induced unsafe abortion according to the following percentages: 35.7% of black women with low instruction level; 40.0% of black women with income lower than $200.00; and 37.7% of black and single women. For purposes of comparison, out of women that are not black and with complete elementary school or higher, only 6.7% thereof induced abortion (interaction table), i.e., among all women that induced unsafe abortion, the highest proportion was represented by black women, with low income, less than 4 years of school attendance and single–such proportion is approximately 5 times the proportion of white women, with higher instruction level and higher income and married, for the same occurrence (IA).
Out of the afro-descendant black women, their great majority have migrated from other states, especially from the Northeast (NE).
“The history of Brazilian people is a history of migrations, continuously searching for better living conditions or even conditions to survive… People from the Northeast are Brazilian migrants par excellence”.12
Internal migration was a sociodemographic characteristic that was distinguishably more relevant within the group of women with SA, in which 81% of the women are from “Out of São Paulo”, the majority of which from the Northeast.12 Therefore, such variable remained in the final model of SA only, with an odds ratio of 3.18, i.e., out of the total number of women interviewed (TW), migrating women present a chance approximately 3.2 times higher of suffering a spontaneous abortion (SA).
To be better understood, such data deserves a more thorough investigation. Why would so many women coming from other regions have so many more spontaneous abortions? Is their health, in general, more jeopardized? Response bias, or omission of induced abortion, for some kind of emotional or behavioral weakness–would they be more afraid to declare IA as a result of a law restrictive to abortion?
Furthermore, regarding Afro-descendant women, 34.5% of black and single women (first event) presented unsafe abortion.
Priority was given to the analysis of the marital status on the occasion of the events (LB, SA, IA) to study the data of the Inajar slum community, for this variable is one of the possible variables to define the occurrence or not of an induced abortion in view of the existence of unintended pregnancy. The distribution of abortions per marital status varies in accordance with specialized literature, notably, according to the regions analyzed.
As regards women with IA, 51% of them were alone (single and separated) on the occasion of their 1st abortion and 86.4% of the total number of them had no emotional or financial support from their partners regarding their decision of interrupting pregnancy or how to do so, which reveals gender issues in this population.12
As previously mentioned, the Marital Status, associated to abortion, varies significantly according to the regions analyzed. In the United States and Cuba, two countries with different socioeconomic and political realities, IA occurs more often among single women, as in Brazil. In the United States, single women have a probability more than four times higher than married women to induce abortion.18
According to a World Review about induced abortion, published in 2001, which referred to countries in which abortion has been legalized and countries in which abortion is restricted by law, developed and emerging countries, the authors conclude that: “In more than half of the countries analyzed, married women present a higher percentage of abortions than single women do Once pregnant, however, single women have more probability to opt for abortion than married women do”.18
In turn, the Alan Guttmacher Institute stated in 1996 that most Latin-American women that are submitted to induced abortions are married; such survey refers to seven countries that concentrate over 70% of the population of that region. Although extremely comprehensive, the survey solely includes data about hospitalized women. Out of all studies mentioned in this survey, only in the study related to Brazil has the proportion of single and separated women, or divorced, or widows, i.e., not in a stable union, been higher (62%) than the proportion of married women.
According to the survey of this community, 33.3% of women induced abortion prior to their 1st live birth, at their first pregnancy; 15.7% had their 1st IA at their 2nd pregnancy; 33.3% at their 3rd; 17.6% at their 4th and subsequent pregnancies. Therefore, in this population, most women (66.6%) had their 1st IA after their first live birth or live births. The marital status of those women presented, for each one of them, a significant oscillation between single, “living together” and married, throughout the pregnancies.
The “not married” marital status, as opposed to married, regarding the first event, indicates that the women that have not ever been married have approximately 3.6 times more probability of inducing unsafe abortion in relation to married women, in the univariate analysis for TWP, remaining as marginally significant in the final model.
Analyzing the variable “age at first sexual intercourse” it's noticed that it remains in the 2 final models of multiple multinomial regression of this survey, with odds ratio of 4.59 for TWP, i.e., women belonging to this latter group that started their sexual activities before they reached 16 years of age present a chance of inducing unsafe abortion approximately 4.6 times higher than the women whose the first sexual intercourse occurred after that age.
Age at first sexual intercourse is a good predictor to begin exposure to pregnancy28 that, in turn, is a necessary condition for abortion. More than 50% of the young women in this population started their sexual activities when they were between 11 and 16 years old; and practically with no measures to prevent an eventual pregnancy.12
That is how 76.6% of the women belonging to the TWP group had their 1st pregnancy before they reached 21 years old. Fifty percent of the women with IA induced their first abortion before they were 20 years old (from 13 to 20 years old inclusive) with an age average of 17.8 years. The quinquennial group from 15 to 19 years old presented the highest concentration of women with first induced abortion (IA), which also occurred with the group of women with LB, and with no abortions, in relation to the first child. More than 57% of all events, of all types (LB, SA, IA), occurred before they were 24 years old, characterizing the precociousness of this population concerning reproductive life.12
The “number of partners” in relation to the year prior to the survey, which remains in the final models of Regression for the 2 groups, TW and TWP, probably reflects a more systematic “risky behavior” to pregnancy, further being indicated by lack of adherence to the use of contraceptives, which, consequently, leads to induced abortion.
The variable “Gap LB-IN”, which refers to the difference between the number of live birth children and the declared ideal number of children,21 indicates a higher proportion of women with LB>IN for the category IA, 47%. The variable presents odds ratio of 3.10 within this group of women, i.e., women with abortion present 3 times more probability than the others of continuing inducing unsafe abortions. The behavior of such variable, differently than what has been observed by Silva in her researches, as well as to the fact that 76.5% of those women have stated that “they no longer wish to become pregnant”,12 indicates the use of abortion to control fertility.
Finally, 94.12% of women that induced unsafe abortions, in this population, mentioned complications related to the abortions, in particular bleeding, with a rate of 83% of hospitalizations, most of them at public hospitals of the area,12 a morbidity rate much higher than that reported in higher income women's populations or those with access to safe abortion.
Conclusions- 1)
The main sociodemographic characteristics (SDC) associated to the occurrence of UA, in this community, analyzed by MMLR, were age at 1st sexual intercourse, number of partners, instruction level, color/ethnicity and acceptance of abortion for lack of economical conditions.
- 2)
Several of those SDC associated to UA promoted health inequalities and even health inequities.
- 3)
The greatest proportion of women that induced unsafe abortion within this population was represented by black women, with lower income, with less than 4 years of school attendance and single, which indicates health inequalities and inequities.
Women in poor conditions belonging to this population that would directly benefit from the legalization of abortion would deserve to be inserted in an effective Family Planning Program or in a program to reduce damages, at least for as long as the respective legislation is not amended.
Conflict of interestThe authors declare no conflicts of interest.