



Endometriosis is a progressive and chronic disease characterized by the presence of endometrial tissue outside the womb location. The main symptoms are dyspareunia, dysmenorrhea and infertility, and affects mainly women in fertile age. It causes numerous problems in various social, psychological and emotional levels. Its incidence ranges from 5 to 15% in the female population of reproductive age. The aim of the study is to describe the women's quality of life with endometriosis and related factors. It is about a systematized review study conducted in electronic databases SciELO and PubMed. The descriptors used were “endometriosis” and “quality of life”, using the advanced search strategy with the Boolean AND. The research period was from March to October 2015. The inclusion criteria were extended to articles published in the last five years in Portuguese and English. The exclusion criteria involved non-original studies, case series, commentaries and editorials. The search resulted in 18 articles divided into three categories. The results indicate that women with endometriosis have quality of life affected, either in the physical, social or mental level. Understanding family members and partner represents an improvement in this confrontation, being, therefore, a specific intervention to improve the quality of life of women with this disease.
A endometriose é uma doença progressiva e crônica caracterizada pela presença de tecido endometrial em localização extrauterina. Os principais sintomas são dispareunia, dismenorreia e infertilidade, acomete, principalmente, mulheres em idade fértil. Acarreta inúmeros problemas nos diversos âmbitos social, psicológico e emocional. Sua incidência varia de 5 a 15% na população feminina em idade reprodutiva. O objetivo do estudo é descrever a qualidade de vida da mulher com endometriose e os fatores relacionados. Trata-se de estudo de revisão sistematizada feito nas bases de dados eletrônicas SciELO e PubMed. Os descritores usados foram “endometriosis” e “quality of life”, com a estratégia de busca avançada com o boleano AND. O período de pesquisa foi de março a outubro de 2015. Os critérios de inclusão se estenderam a artigos publicados nos últimos cinco anos em português e inglês. Os critérios de exclusão envolveram estudos não originais, série de casos, comentários e editoriais. A busca resultou em 18 artigos divididos em três categorias. Os resultados indicam que mulheres com endometriose têm qualidade de vida afetada, seja no bem-estar físico, social e mental. A compreensão dos parentes e do parceiro representa melhoria nesse enfrentamento. É, portanto, uma intervenção especifica para melhoria da qualidade de vida nas mulheres portadoras dessa doença.
Endometriosis is an estrogen-dependent disease characterized by the growth of endometrial tissue that can be evidenced in the extrauterine ovarian, uterine ligaments, the sigmoid colon, the peritoneal pelvis, the cervix and rarely extending to the pleura and pericardium. In the words of Gao et al., 1 the disease is defined by the stromal implant and/or extrauterine endometrial glandular epithelium in location
Some patients with endometriosis are asymptomatic. However, most symptoms have different intensities, the main being dysmenorrhoea, chronic pelvic pain, infertility, deep dyspareunia, or cyclic intestinal and urinary symptoms, such as pain or bleeding when defecating or urinating during menstruation.2
In the United States, endometriosis is the third leading cause of hospitalization for gynecological reasons.3 The reasons are estimated to occur in at least 5.5 million women affected by this disease in the United States and Canada.4 Its incidence in different studies ranges from 5 to 15% in women in the reproductive age and 2–5% in postmenopausal women.5 The highest rates of endometriosis are found in infertile women, with variations from 5 to 50%.6
The typical endometriosis triad (dyspareunia, dysmenorrhea and infertility) has a direct impact on the lives of women in different areas, whether social, physical or psychological.7 Pain has a cyclic nature and is, therefore, repeated and prone to worsening condition in every cycle, interfering with women's health from a holistic point of view.
The deep dyspareunia, in turn, is another symptom that will make the diagnosis of this condition. It will focus on sexual and reproductive health of women, limiting their sexual activity and consequently changing their social and psychological dynamics.8
However, infertility is the biggest challenge to be faced by women with endometriosis. The inability to bear a child or to maintain a pregnancy may have a larger impact on the lives of patients who yearn to have a child.9
Thus, it is evident that the symptoms of endometriosis are affecting the quality of life of these women, causing difficulties in daily activities and social life, altering the general health and personal relationships. The sense of frustration or uncertainty about their reproductive capacity is noteworthy in this context.
Given the range of factors triggered by endometriosis, it must examine the quality of life of the women affected, how the symptoms of the disease have impacted their daily life. Because of the great repercussion of endometriosis on different aspects of life and health of women, it is necessary to understand the confrontation mechanisms of the disease for patients as well as the impact on the quality of their lives. This can determine the improvement of care and the quality of humanization addressed to women from diagnosis to treatment.
The high and increasing rates of endometriosis make relevant research on the subject, considering that its carriers are seen in all walks of life. Given the above, this study has the scope to describe the impact of endometriosis on the quality of life of women.
MethodSystematized review study of the literature on quality of life of women with endometriosis was undertaken. We proceeded to search the literature through online databases of the Scientific Electronic Library Online (SciELO) and the Medical Literature Analysis and Retrieval System Online (MEDLINE), accessed by PubMed between March and October 2015, limiting the articles published between January 2010 and October 10th 2015.
We used the following key words for searching the PubMed database, “endometriosis” (descriptor advanced [Term MeSH]) and “qualify of life” (descriptor advanced [Term and MeSH]). In addition to the MeSH descriptor it was decided to include the descriptor in Health Sciences (DeCS) [“endometriosis” AND “quality of life”] in Advanced search strategy. The search strategy and the articles obtained in the search were reviewed on two separate occasions to ensure the proper selection of the sample. Similar search strategy was held in SciELO database, using the equivalent descriptors in Portuguese.
Analysis of articles followed predetermined eligibility criteria. The following inclusion criteria were adopted: (a) items that had the title of at least one combination of the terms described in the search strategy; (b) publications in English or Portuguese; (c) studies that addressed the theme quality of life of women with endometriosis; and (d) prospective observational studies or retrospective (analytical or descriptive) studies, clinical trial, newspaper article, case report, integrated review and systematic review. Exclusion criteria were (a) other study designs; and (b) publishing, prefaces, and brief letter to the editor communications. The search strategies resulted in 208 studies. After analyzing the titles and abstracts of articles found for eligibility based on the inclusion criteria, 190 articles were excluded and 18 articles were selected in the final sample (Fig. 1).
Results
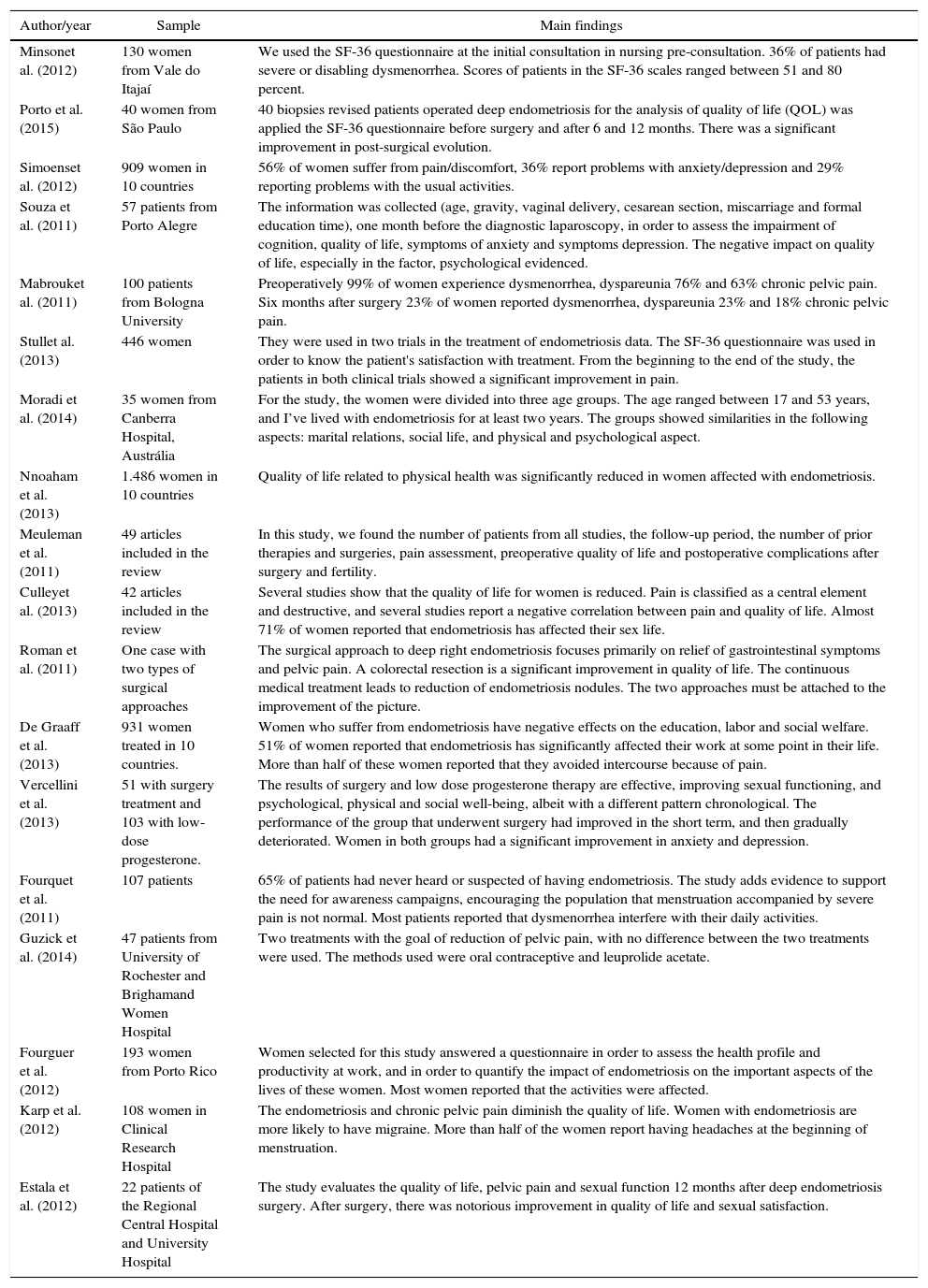
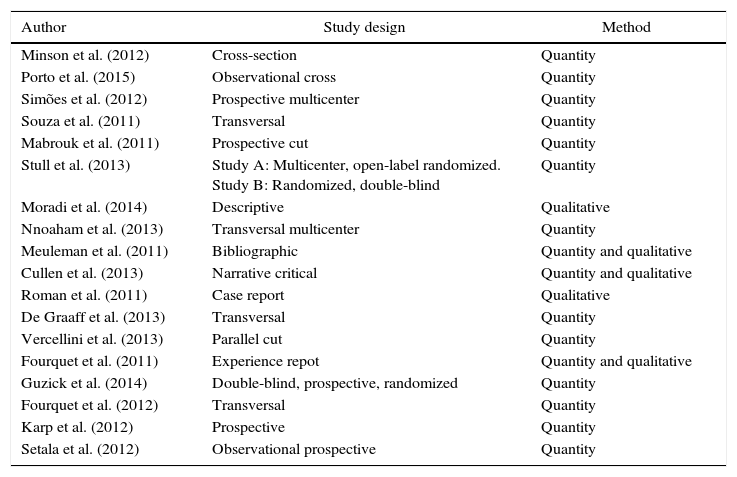
Table 1 provides the summary of the studies included in the final sample and all used in the process of analyzing the information. The 18 studies were divided into three categories: impact of symptoms of endometriosis; endometriosis impact on women's quality of life; and treatment of endometriosis for a better quality of life. Table 2 provides information on the study design that was included in the study.
Summary of articles that discuss the relationship between endometriosis and women's quality of life.
| Author/year | Sample | Main findings |
|---|---|---|
| Minsonet al. (2012) | 130 women from Vale do Itajaí | We used the SF-36 questionnaire at the initial consultation in nursing pre-consultation. 36% of patients had severe or disabling dysmenorrhea. Scores of patients in the SF-36 scales ranged between 51 and 80 percent. |
| Porto et al. (2015) | 40 women from São Paulo | 40 biopsies revised patients operated deep endometriosis for the analysis of quality of life (QOL) was applied the SF-36 questionnaire before surgery and after 6 and 12 months. There was a significant improvement in post-surgical evolution. |
| Simoenset al. (2012) | 909 women in 10 countries | 56% of women suffer from pain/discomfort, 36% report problems with anxiety/depression and 29% reporting problems with the usual activities. |
| Souza et al. (2011) | 57 patients from Porto Alegre | The information was collected (age, gravity, vaginal delivery, cesarean section, miscarriage and formal education time), one month before the diagnostic laparoscopy, in order to assess the impairment of cognition, quality of life, symptoms of anxiety and symptoms depression. The negative impact on quality of life, especially in the factor, psychological evidenced. |
| Mabrouket al. (2011) | 100 patients from Bologna University | Preoperatively 99% of women experience dysmenorrhea, dyspareunia 76% and 63% chronic pelvic pain. Six months after surgery 23% of women reported dysmenorrhea, dyspareunia 23% and 18% chronic pelvic pain. |
| Stullet al. (2013) | 446 women | They were used in two trials in the treatment of endometriosis data. The SF-36 questionnaire was used in order to know the patient's satisfaction with treatment. From the beginning to the end of the study, the patients in both clinical trials showed a significant improvement in pain. |
| Moradi et al. (2014) | 35 women from Canberra Hospital, Austrália | For the study, the women were divided into three age groups. The age ranged between 17 and 53 years, and I’ve lived with endometriosis for at least two years. The groups showed similarities in the following aspects: marital relations, social life, and physical and psychological aspect. |
| Nnoaham et al. (2013) | 1.486 women in 10 countries | Quality of life related to physical health was significantly reduced in women affected with endometriosis. |
| Meuleman et al. (2011) | 49 articles included in the review | In this study, we found the number of patients from all studies, the follow-up period, the number of prior therapies and surgeries, pain assessment, preoperative quality of life and postoperative complications after surgery and fertility. |
| Culleyet al. (2013) | 42 articles included in the review | Several studies show that the quality of life for women is reduced. Pain is classified as a central element and destructive, and several studies report a negative correlation between pain and quality of life. Almost 71% of women reported that endometriosis has affected their sex life. |
| Roman et al. (2011) | One case with two types of surgical approaches | The surgical approach to deep right endometriosis focuses primarily on relief of gastrointestinal symptoms and pelvic pain. A colorectal resection is a significant improvement in quality of life. The continuous medical treatment leads to reduction of endometriosis nodules. The two approaches must be attached to the improvement of the picture. |
| De Graaff et al. (2013) | 931 women treated in 10 countries. | Women who suffer from endometriosis have negative effects on the education, labor and social welfare. 51% of women reported that endometriosis has significantly affected their work at some point in their life. More than half of these women reported that they avoided intercourse because of pain. |
| Vercellini et al. (2013) | 51 with surgery treatment and 103 with low-dose progesterone. | The results of surgery and low dose progesterone therapy are effective, improving sexual functioning, and psychological, physical and social well-being, albeit with a different pattern chronological. The performance of the group that underwent surgery had improved in the short term, and then gradually deteriorated. Women in both groups had a significant improvement in anxiety and depression. |
| Fourquet et al. (2011) | 107 patients | 65% of patients had never heard or suspected of having endometriosis. The study adds evidence to support the need for awareness campaigns, encouraging the population that menstruation accompanied by severe pain is not normal. Most patients reported that dysmenorrhea interfere with their daily activities. |
| Guzick et al. (2014) | 47 patients from University of Rochester and Brighamand Women Hospital | Two treatments with the goal of reduction of pelvic pain, with no difference between the two treatments were used. The methods used were oral contraceptive and leuprolide acetate. |
| Fourguer et al. (2012) | 193 women from Porto Rico | Women selected for this study answered a questionnaire in order to assess the health profile and productivity at work, and in order to quantify the impact of endometriosis on the important aspects of the lives of these women. Most women reported that the activities were affected. |
| Karp et al. (2012) | 108 women in Clinical Research Hospital | The endometriosis and chronic pelvic pain diminish the quality of life. Women with endometriosis are more likely to have migraine. More than half of the women report having headaches at the beginning of menstruation. |
| Estala et al. (2012) | 22 patients of the Regional Central Hospital and University Hospital | The study evaluates the quality of life, pelvic pain and sexual function 12 months after deep endometriosis surgery. After surgery, there was notorious improvement in quality of life and sexual satisfaction. |
Methodological design of the articles that discuss the relationship between endometriosis and women's quality of life.
| Author | Study design | Method |
|---|---|---|
| Minson et al. (2012) | Cross-section | Quantity |
| Porto et al. (2015) | Observational cross | Quantity |
| Simões et al. (2012) | Prospective multicenter | Quantity |
| Souza et al. (2011) | Transversal | Quantity |
| Mabrouk et al. (2011) | Prospective cut | Quantity |
| Stull et al. (2013) | Study A: Multicenter, open-label randomized. Study B: Randomized, double-blind | Quantity |
| Moradi et al. (2014) | Descriptive | Qualitative |
| Nnoaham et al. (2013) | Transversal multicenter | Quantity |
| Meuleman et al. (2011) | Bibliographic | Quantity and qualitative |
| Cullen et al. (2013) | Narrative critical | Quantity and qualitative |
| Roman et al. (2011) | Case report | Qualitative |
| De Graaff et al. (2013) | Transversal | Quantity |
| Vercellini et al. (2013) | Parallel cut | Quantity |
| Fourquet et al. (2011) | Experience repot | Quantity and qualitative |
| Guzick et al. (2014) | Double-blind, prospective, randomized | Quantity |
| Fourquet et al. (2012) | Transversal | Quantity |
| Karp et al. (2012) | Prospective | Quantity |
| Setala et al. (2012) | Observational prospective | Quantity |
In recent years, there has been growing interest on the effect of endometriosis in health-related quality of life. Women are increasingly willing to be informed of the treatment options and decide on how best to adapt to their needs.7 Qualitative studies have shown that symptoms of endometriosis have substantial impact on the physical, emotional and social well-being of patients that were affected during the most productive years of their lives.8
Endometriosis causes severe painful symptoms, often incapacitating.10 The condition is associated with a variety of clinical symptoms such as dysmenorrhea, dyspareunia, dyschezia, back pain and chronic pelvic pain.
It has been found that chronic pelvic pain is the most important clinical factor of endometriosis.11 Accordingly, the pain is a major concern of patients with endometriosis as well as their effects on the quality of life,9 because several studies have reported negative relationship between both.12
Pelvic pain can be cyclical or chronic, and often disabling,8 presenting itself as the most pronounced complaint having an impact on every aspect of daily life,13 like sleeping, eating or moving.12 Evaluate the complaint isolated pain in patients with endometriosis is difficult to assess in women with endometriosis, as the site of the disease and the type of pain are variable and generate numerous questions and daily graded recitations of how trustworthy are in the final.14
The intensity of symptoms is directly related to the size and location of outbreaks and the disease stage.14 The intensity of pain associated with endometriosis occurs not only due to the staging of the disease but also because of the symptoms manifesting time, and may be influenced by other variables such as psychosocial factors.15
Women with endometriosis suffer from severe and progressive pain during menstrual and non-menstrual phases in different areas, such as the lower abdomen, intestine, bladder, lower back and legs that significantly affect their lives.16
Problems with sexual life and intimate relationships are also common.11 Some studies have shown that symptomatic women have less sex than asymptomatic women.12 Pain during coital activity may originate from pressure on the endometrial nodules embedded in fibrotic tissue, traction scars, inelastic parametrium and immobilization of posterior uterine pelvic structures.7
Women with endometriosis have reported having less sex and more frequent interruption of intercourse due to pain.13 Half the women reported continue to suffer from dyspareunia, with significant effect on quality of life.7
Infertility is another important feature of endometriosis patients.9 Most women have difficulty getting pregnant, 71% of these have tried to conceive and 90% had difficulties in the experience. Infertility is reported as a concern, which results in depression and feelings of inadequacy among women, as well as uncertainty about future fertility, contributing to the breakdown of a relationship.12
Fertility improvement is often an important goal for women undergoing endometriosis surgery. In mild endometriosis, laparoscopic surgery is used in the recovery of fertility and pregnancy outcomes, with less negative impact than the approach by laparotomy.17
In fact, women with endometriosis were significantly more likely to have migraine than those without endometriosis. Seeking a common pathophysiology involving migraine and endometriosis, note that prostaglandins play a role in the pathogenesis of migraine and that endometriosis is associated with elevated circulatory levels of prostaglandins.18
Endometriosis impact on women's quality of lifeEndometriosis is a benign disease that affects young women, professionally active, who may plan to get pregnant.19 Deep endometriosis promotes significant impact on quality of life.14 The impact of endometriosis has been little researched, and so has influenced the quality of life, as well as the severity of symptoms and seeking care.20
The existence of symptomatic endometriosis has physical, mental and adverse impact on the social well-being and thus has a negative effect on health-related quality of life.11 The impact includes the areas on fertility, sexuality, ability to work and maintain personal relationships.16
The reduction in quality of life in this population may be explained by the complexity of the etiology and manifestations of the disease; non-responsiveness of some patients to interventions; pain as a major symptom; endometriosis interference in the reproductive capacity of women and the existence of pain during intercourse.15
Relate the health and quality of life in patients with endometriosis requires intregral approach.21 Another more commonly affected quality of life factor was the change in mood. In addition, feeling depressed because of the possibility of not being able to conceive is commonly reported as a great distress.10
Endometriosis reduces the quality of life of women and most are absent at work due to pain.18 Severe pain and dyspareunia predict loss in social and sexual aspects of life,8 such as reduced quality of life and lost productivity at work, accounting for nearly 60% loss of productivity at work.10
Chronic pelvic pain caused by endometriosis has reduced sexual satisfaction and also led to significant damage in health-related quality of life compared to the general population.22
Bleeding during and after sex are experienced by only a few women, demonstrating the concern expressed by the partners of women affected by the disease.16 The painful sex also has intimate and personal implications, with substantial psychological distress in the relationship, as well as negative emotional impact on the partner.7
The management of post-diagnostic healthcare needs to be more holistic. This should be clarified by an understanding of the multidimensional endometriosis impact and supported by a biopsychosocial approach that includes emotional support, stress reduction, social support, coping strategies, psychosexual treatment and focus on quality of life issues, sex and relationships, control of pain and career counseling.12
Treatment of endometriosis for a better quality of lifeMedical and surgical treatments aim to control symptoms and remove or reduce disease.21 Conservative surgery is typically associated with a significant reduction of short-term pain. Many studies confirm that the laparoscopic treatment of endometriosis is effective in the relief of dysmenorrhoea, dyspareunia, pelvic pain and menstrual pain, not dyschezia.19
The delay in diagnosis may impact the treatment and hence the quality of life. And there may be complications in the condition, as it may worsen every cycle; meanwhile, the woman will suffer with the symptoms and is dealing with the consequences of it in her routine.
There is no cure for endometriosis and there is no guarantee that it will not return.16 However, it was shown that after surgery there is a significant improvement in quality of life. Preoperative accurate assessment of the extent of the disease to select the appropriate treatment, adapting to the specific case is needed.17
Many women have been trying to become pregnant, however, only a few seek infertility treatments, including in vitro fertilization, artificial insemination, surgery, or a combination thereof. Having a partner seems to be a factor with a strong positive effect on the mental component of quality of life. It is understandable that the support of partners can contribute to improving the mental aspect of quality of life of women. However, this effect cannot be reserved exclusively for women with endometriosis.13
According to the literature, both surgical and pharmacological treatments improve the physical and psychological functioning, vitality, level of pain and general health.7 In addition to medical and surgical treatment, other alternatives are used for the management of endometriosis, as a complementary or alternative therapy in lifestyle changes such as exercise, diet and sleep.16
It is believed that characterizing the histological type may be related to pain; well-differentiated glandular type predominates in superficial injury, while in deep injury, the mixed glandular type and the undifferentiated type dominates. Therefore, it is understood that this assumption is valid; drugs will be developed and selectively prescribed to alleviate pain from the knowledge of histological type and thus provide better quality of life. For this, the identification and the agent response may be the key to success for greater drug efficacy and better quality of life for women with endometriosis.14
Although able to significantly reduce pelvic pain, continuous hormonal treatment does not lead to the complete disappearance of deep endometriosis nodules, but a slight decrease in volume.23
Many authors believe that incomplete excision of endometriosis is a major cause for clinical recurrence. In assessing the endometriosis recurrence rate, several factors must be taken into consideration. First, it is important to distinguish symptom recurrence and the actual recurrence of the disease and the need for drugs or surgical therapy. Second, it is difficult to distinguish between residual disease and recurrent disease.17
However the long-term results of the surgical treatment of endometriosis are positively correlated with the medical therapy, leading to the conclusion that only the combination of most medical therapies and surgery can ensure long-term effect.19
A treatment that only aims to eradicate the underlying condition is not sufficient. In addition to seeking to improve the quality of life of these women, medical care should also address the emotional, sexual and social problems that come with the disease. So in addition to continued improvement of surgical and medical therapy techniques, future directions of treatment should also include teaching patients how to deal with chronic pelvic pain, to explore ways to have sexual intercourse without pain and to teach patients to strengthen relations with its partners and friends so that they are in solidarity in dealing with the disease.13
Final considerationsEndometriosis affects the everyday lives of women, hindering their daily activities, in personal relationships, and interferes with the reproductive capacity. Therefore, to improve the quality of life of the woman who has endometriosis, it is first necessary to understand the patients according to their clinical condition, and which appropriate medical treatment she should undergo, if surgical or medical, for a better quality of life.
Conflicts of interestThe authors declare no conflicts of interest.
Study conducted at Faculdade de Juazeiro do Norte, Juazeiro do Norte, CE, Brazil.