







The standard treatment for endometrial cancer is simple hysterectomy with bilateral salpingo-oophorectomy. Patients with high risk also benefit from lumbo-aortic lymphadenectomy. High risk patients include those with grades and histologic subtypes associated with poor prognosis and depth of myometrial invasion greater than 50% (M2). To determine which patients would benefit from lumbo-aortic lymphadenectomy, the depth of myometrial invasion can be assessed by intraoperative frozen section or by magnetic resonance imaging (MRI). We aimed to determine the diagnostic yield of intraoperative frozen section and MRI for detecting the presence of M2 in patients with endometrial cancer.
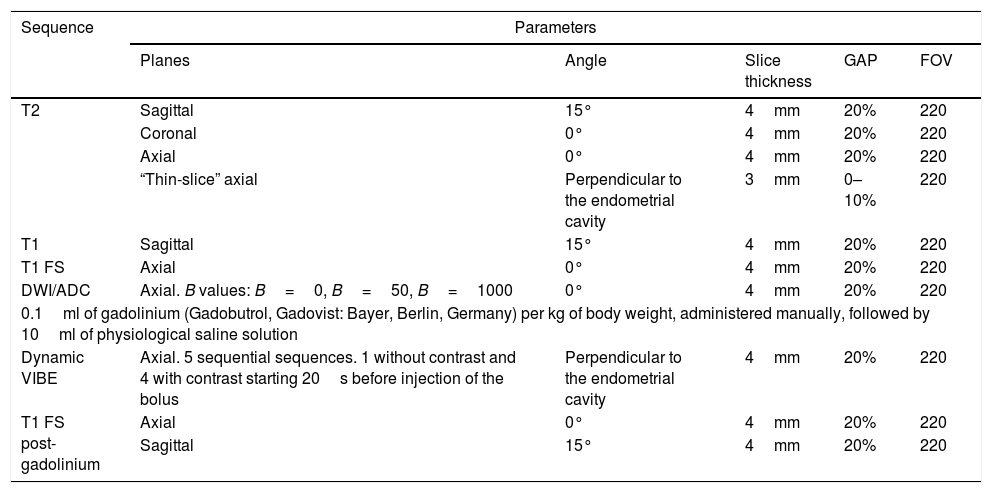
Materials and methodsThis cross-sectional study included women with a histologically confirmed diagnosis of endometrial cancer who underwent baseline MRI and surgical intervention in our institution between 1 January 2010 and 31 December 2017. We reviewed the MRI studies and the intraoperative frozen section reports and compared them with the information in the histopathology report. We compared the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the two tests. We also calculated the diagnostic accuracy of each method and the percentages of underestimation and overestimation. Finally, we calculated the predictive value of MRI for the presence of M2, adjusting it for the histologic variables known to be associated with poor prognosis.
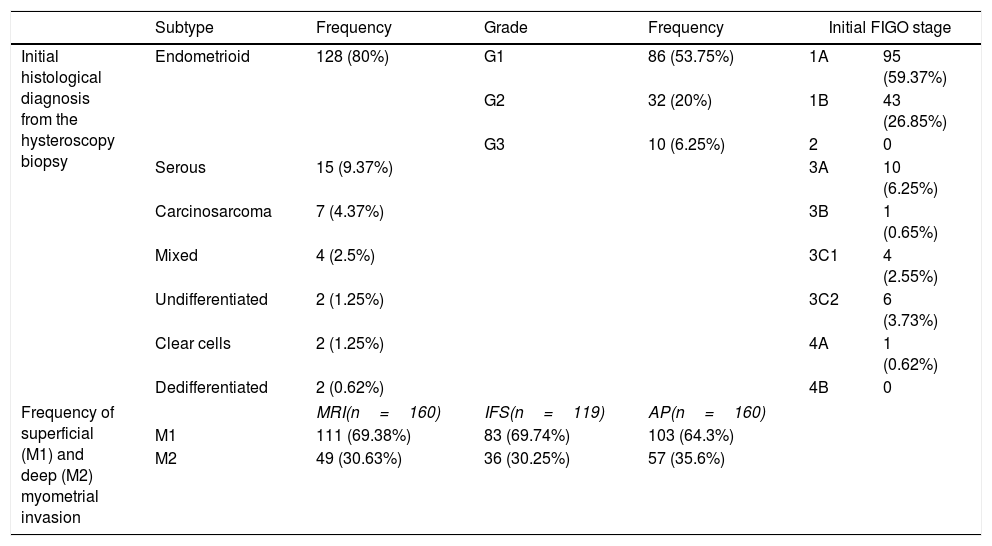
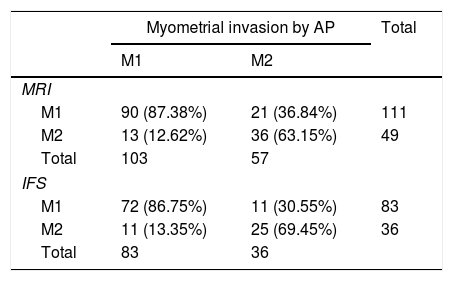
ResultsTo detect M2, MRI had 63% sensitivity, 87% specificity, 73% PPV, and 81% NPV; the diagnostic accuracy was 78.8%, with 13.12% underestimation and 8.13% overestimation of M2. Intraoperative frozen section had 69% sensitivity, 86.7% specificity, 69% PPV, and 86% NPV; the diagnostic accuracy was 81.5%, with 9.24% underestimation and 9.24% overestimation of M2. The degree of concordance between the two methods was moderate (k=0.54, p<0.00001).
ConclusionsIn our experience, MRI and intraoperative frozen section have adequate diagnostic yields for determining M2, though intraoperative frozen section is slightly better. The contribution of MRI in determining the presence and the site of deep myometrial invasion, as well as the factors that can confound the diagnosis, when added to the contribution of intraoperative frozen section, means that both methods help reduce the number of unnecessary lymph node dissections and the morbidity, mortality, and health costs associated with this practice.
El tratamiento estándar para el cáncer de endometrio (CE) es la histerectomía simple con salpingo-ooforectomía bilateral. Las pacientes dentro del grupo de alto riesgo son las que se benefician de la linfadenectomía lumboaórtica. En dicho grupo se encuentran las que presentan grado y subtipo histológico de mal pronóstico y profundidad de invasión miometrial superior al 50% (M2). Este último parámetro puede ser brindado por el estudio intraoperatorio por congelación (EIC) y la resonancia magnética (RM), contribuyendo a decidir quiénes se beneficiarán de la linfadenectomía. El objetivo es establecer el rédito diagnóstico de la RM y EIC para determinar la presencia de M2 en pacientes con CE.
Materiales y métodosEstudio de tipo test diagnóstico, corte transversal. Se incluyeron pacientes de sexo femenino con diagnóstico histopatológico de CE, a las que se realizó RM inicial o basal y fueron intervenidas quirúrgicamente en nuestra institución entre el 1 de enero de 2010 y el 31 de diciembre de 2017. Se estudiaron las RM y los informes de EIC y se compararon con los datos del informe de anatomía patológica. Se efectuó un análisis estadístico de sensibilidad, especificidad, valor predictivo positivo (VPP) y valor predictivo negativo (VPN) de ambas pruebas diagnósticas. También se calculó la tasa de precisión diagnóstica de cada método discriminado, el porcentaje de subestimación y sobrestimación. Finalmente, se calculó el valor predictivo de la RM para determinar la presencia de M2 ajustándolo por las variables histológicas de mal pronóstico conocidas.
ResultadosPara la determinación de M2, la RM presentó una sensibilidad del 63%, una especificidad del 87%, un VPP del 73% y un VPN del 81%. La tasa de precisión diagnóstica fue del 78,8%, un 13,12% por subestimación y un 8,13% por sobrestimación de M2. Por su parte, el EIC presentó una sensibilidad del 69%, una especificidad del 86,7%, un VPP del 69% y un VPN del 86%. La tasa de precisión diagnóstica fue del 81,5%, un 9,24% por subestimación y 9,24% por sobrestimación de M2. El grado de concordancia entre ambos métodos es moderada (valor de kappa de 0,54, p<0,00001).
ConclusionesEn nuestra experiencia, la RM y el EIC presentan un adecuado rédito diagnóstico, pero a favor del EIC, para determinar M2. La contribución de la RM al determinar la presencia y el sitio de invasión miometrial profunda, así como de los factores que puedan resultar confundidores, sumado al aporte de la EIC, se traduce en que ambos métodos ayudan a disminuir el número innecesario de linfadenectomías, con la morbimortalidad y los costos en salud asociados.

