






The modified Glasgow prognostic score (mGPS) has been reported to have a prognostic value in various patient populations. However, the prognostic significance of mGPS has not been studied inacute pulmonary embolism (APE).
ObjectiveThis study aimed to investigate the predictive value of mGPS on in-hospital mortality in patients with hemodynamically stableAPE.
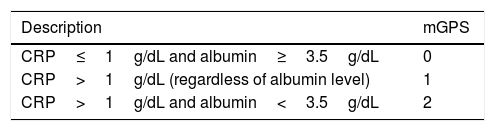
MethodsWe retrospectively included 258 hemodynamically stableAPE patients. Clinical, echocardiographic, and laboratory data recorded on admission. The mGPS scored as 0, 1, or 2 based on the C-reactive protein (CRP) and albumin levels.
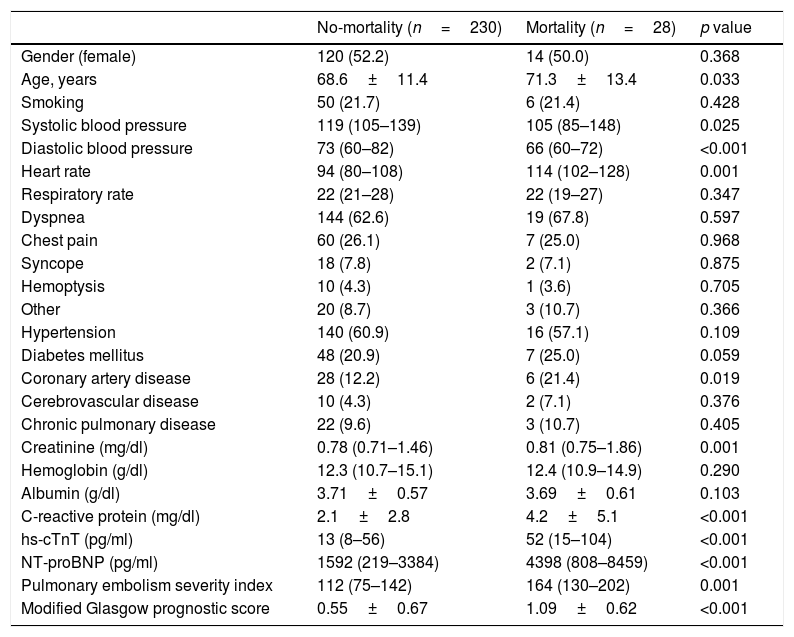
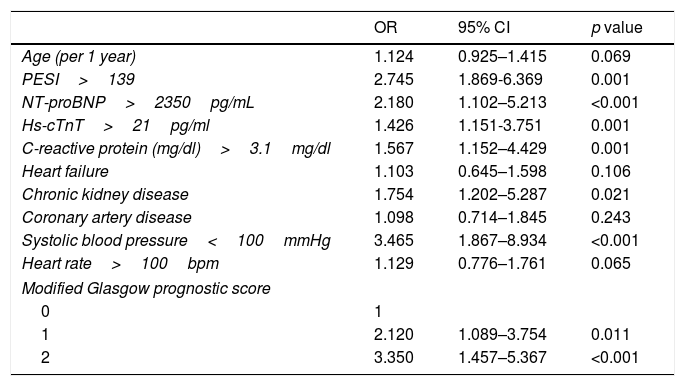
ResultsA total of 258hemodynamically stableAPE patients were included, and 28 (10.9%) died during the hospital stay. Compared with survivors, non-survivors were older, had higher N-terminal pro-B-type natriuretic peptide, CRP, creatinine, high-sensitive cardiac troponin T (hs-cTnT), and mGPS levels, and had higher pulmonary embolism severity index (PESI) at study entry. In the multivariate logistic regression analysis, NT-proBNP>2350pg/mL (OR: 2.180, 95% CI 1.102–5.213, p<0.001), hs-cTnT>21pg/mL (OR: 1.426, 95% CI 1.151–3.751, p=0.001), CRP>3.1mg/dL (OR: 1.567, 95% CI 1.072–4.429, p=0.001), PESI>139 (OR: 2.745, 95% CI 1.869–6.369, p=0.001), systolic blood pressure<100mmHg (OR: 3.465, 95% CI 1.867–8.934, p<0.001), mGPS=1 (OR: 2.120, 95% CI 1.089–3.754, p=0.011), and mGPS=2 (OR: 3.350, 95% CI 1.457–5.367, p<0.001) were independently associated with in-hospital mortality.
ConclusionThis study demonstrates the mGPS, which is a new and easily measurable marker, is a useful predictor in-hospital mortality in hemodynamically stableAPE.
La puntuación pronóstica de Glasgow modificada (mGPS) ha demostrado tener un valor pronóstico en varias poblaciones de pacientes. Sin embargo, no se ha estudiado la importancia pronóstica de la mGPS en la embolia pulmonar aguda (EPA).
ObjetivoEl objetivo de este estudio es investigar el valor predictivo del mGPS sobre la mortalidad intrahospitalaria en pacientes con EPA hemodinámicamente estable.
MétodosSe incluyeron retrospectivamente 258 pacientes con EPA hemodinámicamente estable. Se registraron datos clínicos, ecocardiográficos y de laboratorio al ingreso. El mGPS se calificó como 0, 1 o 2 en función de los niveles de proteína C reactiva (PCR) y albúmina.
ResultadosSe incluyeron un total de 258 pacientes con EPA hemodinámicamente estables, y 28 (10,9%) fallecieron durante la estancia hospitalaria. En comparación con los supervivientes, los no supervivientes eran de mayor edad, tenían niveles más altos de péptido natriurético N-terminal pro-B, PCR, creatinina, troponina T cardíaca de alta sensibilidad (hs-cTnT) y mGPS, y tenían un índice de gravedad de la embolia pulmonar (PESI) más alto al inicio del estudio. En el análisis de regresión logística multivariante, NT-proBNP>2350pg/mL (OR: 2,180; IC del 95%: 1,102-5,213; p<0,001), hs-cTnT>21pg/mL (OR: 1. 426; IC del 95%: 0,951-3,751; p=0,001), PCR>3,1mg/dL (OR: 1,567; IC del 95%: 1,072-4,429; p=0,001), PESI>139 (OR: 2,745; IC del 95%: 0,869-6,369; p=0,001), presión arterial sistólica<100mmHg (OR: 3. 465; IC del 95%: 0,867-8,934; p<0,001), mGPS=1 (OR: 2,120; IC del 95%: 1,089-3,754; p=0,011) y mGPS=2 (OR: 3,350; IC del 95%: 1,457-5,367; p<0,001) se asociaron de forma independiente con la mortalidad intrahospitalaria.
ConclusionesEste estudio demuestra que el mGPS, que es un marcador nuevo y fácilmente medible, es un predictor útil de la mortalidad intrahospitalaria en la EPA hemodinámicamente estable.
