



Diabetes is a chronic, incurable disease affecting various aspects of the patient's life. Diagnosis of the disease is usually unexpected for both the patient and his relatives; this raises a number of emotions and can also provoke a variety of attitudes. A chronic, incurable disease is always a source of stress, and dealing with it demands the incorporation of various strategies. In coping with stress, a person can use both reactive strategies - focused on currently experienced stress; and proactive - taken to avoid, reduce or prevent the development of difficulties in the early stages of their appearance. Anticipating and preparing for difficult situations reduces tension and increases readiness to overcome them, this serves to use and strengthen a person's resources before experiencing difficulties.1,2 Undertaking any active action usually involves earlier acceptance of the disease. Acceptance of the disease means adopting a positive attitude towards the given situation, it is associated with realizing the disease's significance, promoting the mobilization of patient strength and facilitating the adaptation process. As a consequence, this prevents the reduction of quality of life and reduces the risk of complications associated with the disease.3 The process of accepting the disease is also connected with the various emotions that arise during the realization of the significance of the disease, its progression and consequences. Feelings such as anger, anxiety and depression, in the absence of acceptance of a new situation can lead to the appearance of chronic depression and anxiety. Acceptance of the disease may be important in the process of developing a different way of functioning with new habits and life restrictions. Attitudes to the disease differ, what's more, patients may accept the problem in varying degrees depending on the type of diabetes. With regard to type 1 diabetes, which affects children or young people, its manifestation usually affects the whole family system. In parallel with the diagnosis, parents “lose” a healthy child, and the patient must adapt his whole life, his future conditioned by the disease which must be included in his life planning. In the case of type 2 diabetes, which affects older people, the diagnosis of the disease, in turn, requires the patient to change his long-term habits which include eating habits and physical activity, as well as professional and social functioning. The process of accepting the disease and adaptation is usually long, multistage and depends on diverse individual factors, among others: age, gender, personality traits, ability to cope with crisis situations and the type and progression of the disease. It can also have a significant impact on the quality of life assessment.4
Aim of the studyThe aim of the study was to assess the degree of the acceptance of disease and its relation with the quality of life in patients with type 1 and type 2 diabetes.
Material and methodsA total of 191 patients who had been hospitalized in the Department of Internal Medicine and Diabetology in Zabrze were enrolled of which 101 (51 women, 50 men) were diagnosed with type1 diabetes (the average age of the patients was 33.8 ± 13.2 years) and 90 (50 women, 40 men) were diagnosed with type 2 diabetes (mean age 59.8 ± 6.6 years).
The criteria for inclusion in the study were as follow: at least one year of living with diabetes, and the absence of a mental disorder (including cognitive impairment) and diabetic complications. All patients gave written informed consent for participation in the study.
The following psychometric questionnaires were used to assess the examining parameters:
- 1.
The Acceptance of Illness Scale (AIS). The scale consists of 8 statements expressing specific difficulties and limitations caused by the disease, its range is from 8 to 40 points. The overall measure of disease acceptance is the sum of points obtained. The results can be grouped into three categories: Low (8–19 points), Medium (20-35 points) and High (36–40 points). A low result means a lack of acceptance and adaptation to the disease and a strong sense of mental discomfort. A high result indicates the acceptance of one's medical condition and is manifested by the lack of negative emotions associated with the disease.5
- 2.
The SF-36 Quality of Life Scale by J.E. Ware adapted to Polish conditions. This is a generic scale that allows you to compare the quality of life of patients with various diseases. This scale contains 36 questions regarding 8 areas of life: physical pain (BP), physical functioning (PF), physical limitations in performing roles (RP), emotional limitations in performing roles (RE), mental health (MH), social functioning (SF), vitality (VT), general health (GH), and two summary subscales comprehensively covering functioning in the physical dimension (PCS) and the mental dimension (MCS). After using the appropriate conversion formula, a score is obtained from 0-100 points in each of the domains. The higher the result achieved, the better the state of health.6,7
- 3.
The Satisfaction with Life Scale (SWLS). The scale examines the sense of satisfaction with life understood as a subjective assessment of the quality of functioning. It contains five sections. The respondent is asked to answer each of the statements by determining to what extent each of them relates to his current life, from strongly agree (7 points) to strongly disagree (1 point). The grades are totalled and the result obtained determines the degree of satisfaction with life. The results range from 5 to 35 points.5
In addition to the previous assessments, symptoms of depression and anxiety that could affect the degree acceptance of the disease and quality of life were included. The scales employed were:
- 4.
The Hospital Anxiety and Depression Scale (HADS). The scale consists of two independent subscales containing 7 statements, one of which evaluates anxiety (HADS-A) and the other depression (HADS-D). Obtaining to 7 points in both subscales is considered a norm.8
Sociodemographic data was collected using a data questionnaire constructed by the authors, obtaining information on the latest result of glycated hemoglobin (HbA1c), duration of the disease and absence of disease complications.
Statistical data analysisThe following statistical tests were used in the analysis - the Mann-Whitney U test; Spearman's rank correlation test was used to assess the relationships between the data. A significance level of p <0.05 was assumed as statistically significant.
ResultsDescription of the study groups.
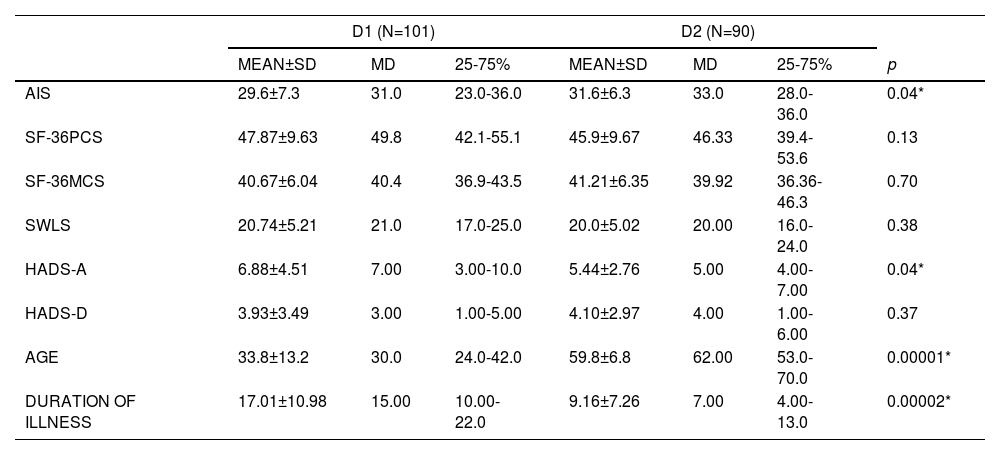
In the cohort of patients with type 1 diabetes, the duration of the disease was 17.01 ± 10.98 years and in the cohort of patients with type 2 diabetes, it was 9.16 ± 7.26 years. The patients in both groups differed significantly in age (p <0.000) however, the value of HbA1c in the group with type 1 diabetes was 7.93 ± 1.5, and type 2 diabetes - 8.09 ± 1.08 signalling that there were no statistically significant differences between the groups. Patients with any diabetes complications were not included in the study (Table 1).
Values of parameters tested in individual groups (D1 - patients with type 1 diabetes, D2 - patients with type 2 diabetes, N-number of patients, MEAN - mean value, MD – median, SD-standard deviation, 25% -75% - middle interval. AIS – score of the Acceptance of Illness Scale, PCS- Physical Component Summary Scale of the SF-36, MCS - Mental Component Summary Scale of the SF-36, SWLS -the Satisfaction with Life Scale and HADS –A anxiety subscale of the Hospital Anxiety and Depression Scale and HADS-D-depression subscale of the Hospital Anxiety and Depression Scale, HbA1c-the level of of glycated hemoglobin.
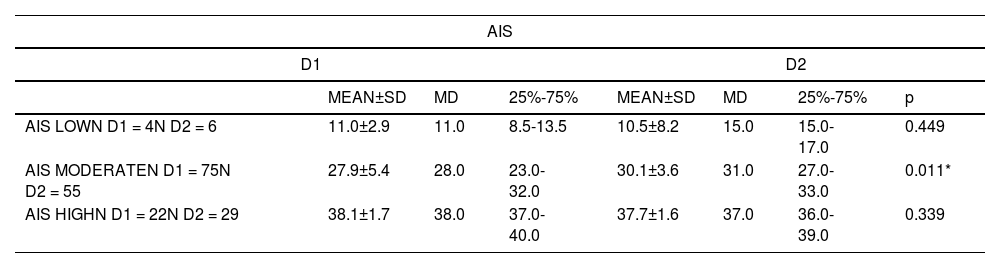
On the AIS scale, patients with type 1 diabetes obtained an average score of 29.56 ± 7.33 points; among people with type 2 diabetes an average score of 31.57 ± 6.25 points was noted. The difference was statistically significant (p = 0.04) (Table 1). Diabetic patients divided into three groups of the AIS scale were presented in the Table 3.
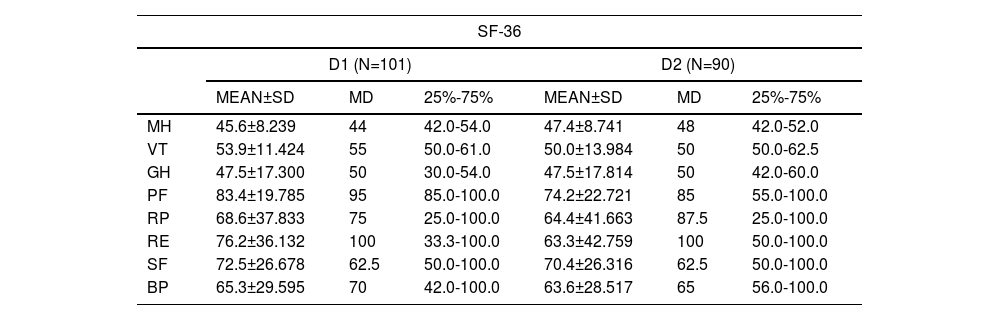
Quality of lifeIn order to simplify the data analysis in the assessment of quality of life using the SF-36 scale, only the PSC and the MCS summary scales were taken into account. Patients diagnosed with type 1 diabetes on the PCS subscale achieved a score of 47.87 ± 9.63 points and on the MCS 40.67 ± 6.04 points. Patients with type 2 diabetes on the PCS subscale achieved a score of 45.97 ± 9.59 points and on the MCS subscale a score of 41.21 ± 6.35 points. Comparing the obtained results, no statistically significant differences were noted, in either terms of physical functioning determined by the PCS scale or mental functioning determined by the MCS scale (Tables 1 and 2).
Values of domains of SF-36 in the group of patients with diabetes type 1 (D1) and type 2 (D2). N-number of patients, Mean-mean value, SD-standard deviation, MD – median, 25% -75% - middle interval.
On the SWLS scale, patients with type 1 diabetes obtained an average score of 20.74 ± 5.21 points; among people with type 2 diabetes it resulted in an average score of 20.03 ± 5.03 points. No statistically significant differences were observed in the tested values (Table 1).
Anxiety and depression assessmentPatients with type 1 diabetes achieved mean values on the depression scale of 3.93 ± 3.49 points, and on the anxiety scale 6.88 ± 4.51 points. Subjects with type 2 diabetes on the depression scale achieved 4.10 ± 2.97 points, and the anxiety scale measured 5.44 ± 2.76 points. Neither of the groups differed statistically significantly in the assessment of depression, while statistically significant differences were noted in the level of anxiety (p = 0.04) (Table 1).
In addition, in the cohort of diabetes type 2, women achieved statistically significantly worse results in terms of depression (p = 0.03) and anxiety (p = 0.01) than men.
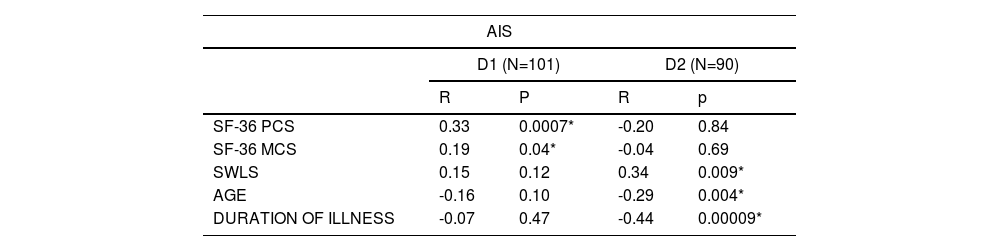
The relationship between the parametersIn the group of patients with type1 diabetes, positive correlations of the level of the acceptance of disease with physical functioning determined by the PCS scale (p = 0.0007) and the MCS scale (p = 0.04) were demonstrated. In the assessment of life satisfaction, no statistically significant relation of any of the parameters examined was found.
In the group of patients with type 2 diabetes, life satisfaction correlated positively with the acceptance of disease (p = 0.009). However, no statistically significant correlation between the acceptance of the disease with the PCS and the MCS results was found. In addition, the age of the respondents (p = 0.004) and the duration of the disease (p < 0.00) negatively correlated with the acceptance of the disease (Table 4). Women with type 2 diabetes demonstrated a better acceptance of the disease than men (p = 0.04).
Spearman's rank correlation coefficient R values in diabetic patients with type 1 and type 2 (D1 - patients with diabetes type 1, D2 - patients with diabetes type 2, N-number of patients, AIS the Acceptance of Illness Scale, PCS- Physical Component Summary Scale of the SF-36, MCS - Mental Component Summary Scale of the SF-36, SWLS -the Satisfaction with Life Scale).
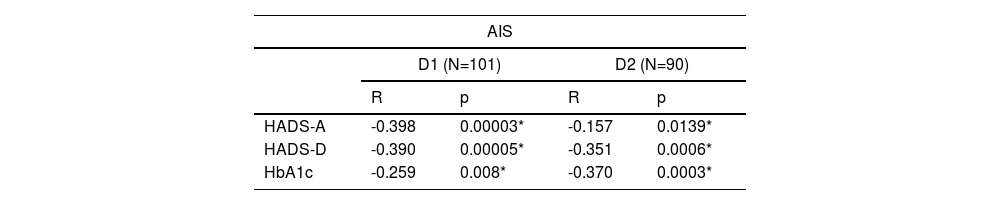
In both cohorts, acceptance of the disease correlated negatively with severity of anxiety and depression, and positively with metabolic control (Table 5).
Spearman's rank correlation coefficient R values and p-value in the group of patients with type 1 and type 2 diabetes (D1 - patients with diabetes type 1, D2 - patients with diabetes type 2, N-number of patients, AIS the Acceptance of Illness Scale, HADS –A anxiety subscale of the Hospital Anxiety and Depression Scale and HADS-D-depression subscale of the Hospital Anxiety and Depression Scale, HbA1c-the level of of glycated haemoglobin).
Due to the statistical differences (age and duration of disease) we have conducted additional analysis to check association with the above mention parameters, and quality of life and satisfaction with life. In both groups we did not notice any significant differences in most of the examined parameters, the only exception was a negative significant correlation between age and satisfaction with life in patients with type 2 diabetes (p = 0.0002)
DiscussionPrevious studies confirm that acceptance of the disease is an important element in the process of adaptation to life with a chronic disease. The greater the acceptance, the better the adaptation and the less discomfort arising from the disease.9-12 In this study, patients with both types of diabetes showed an average level acceptance of the disease. In the group of patients with type 2 diabetes, the average AIS score was 31.57 points. Similar values were obtained by other authors.4,13,14 In the studies of Olszak et al.,4 the average AIS score in the group of patients with diabetes was 27.2 points. In the studies presented by Kurpas et al.,15 the average score was 29.0 points. What's more, in studies conducted by Lewko et al.,13 patients achieved an average score of 29.5 points. These results are comparable to those obtained by patients in our study and indicate the average degree of acceptance of the disease. The cohort with type 1 diabetes achieved an average score of 29.56 points and it was statistically significantly worse than the result achieved by the cohort with type 2 diabetes. In Trojanowska studies conducted in the age group of patients 13-18 years with a diagnosis of type 1 diabetes, the average result was 27.8 points and negatively correlated with health-related behaviours and a tendency to abuse alcohol.16 It is difficult to explain lower level of acceptance of the disease among patients with type 1 diabetes. Perhaps this group of patients, younger in age, where diabetes is often the only chronic disease and largely conditions their future, may have greater problems accepting the disease. The appearance of a chronic, incurable disease at a young age is associated with a number of changes that must occur in the life of the patient and the whole family. The consequence of the diagnosis is a total change in terms of diet, physical and social activity. The patient must also include the disease in their life plans, both in the personal and professional sphere.
Diabetes may impede the emergence of sentimental relationships: in men for fear of rejection due to a chronic disease, and in women the issue of planned maternity, especially regarding pregnancy and childbirth, may become a serious worry. The illness can also be an obstacle in choosing some professions.3 The very fact of struggling with a chronic illness can lead to a number of negative emotions. Anxiety can be also associated with a potential, serious and sudden threat to life from complications arising from the disease and frustration can accompany the awareness that the disease is a permanent state for the remainder of their life. All of these factors can largely determine the acceptance process of functioning with type 1 diabetes. On the other hand, the diagnosis of type 2 diabetes concerns a vast majority of mature age patients, who have often faced a previous diagnosis of another chronic disease, therefore they have had to accept certain limitations associated with that chronic disease, hence "one additional disease" may no longer be considered such an issue, facilitating the acceptance of the diabetes. In our study, patients with both types of diabetes did not differ in terms of quality of life, life satisfaction, or symptoms of depressions studied. The only additional parameter differentiating both groups was the higher level of anxiety among patients with type 2 diabetes. Glińska17 showed a similar lack of differences in the assessment of the quality of life of patients with type 1 and type 2 diabetes,17 nonetheless that study noted a slight tendency to assess the quality of life worse in the group of patients with type 1 diabetes them type 2 diabetes. In our study, the diagnosis did not differentiate patients in terms of quality of life, but the group of patients with type 1 diabetes demonstrated to have a positive relationship between acceptance of the disease and quality of life. In the group of patients with type 2 diabetes, no such relationship was observed, while a positive connection of accepting the disease with the life satisfaction was noted. Most of the authors prove in their studies the positive impact of accepting the disease on the quality of life assessment and life satisfaction.3,10,12 Pantlinowska showed that patients accepting the disease function better physically, emotionally and professionally. In the study conducted in the group of patients with type 2 diabetes, older men with a longer duration of the disease showed worse acceptance of the disease. The analysis of available research shows diversity in this area. Some authors emphasize a worse acceptance of the disease in women,15,18,19 others take the view that men are less disciplined in respecting the restrictions associated with the disease, they cope with chronic diseases worse and accept them less.3,20,21 Men also often demonstrate adverse health behaviours, incorrect adaptation to stress, and tendencies to inadequately seek medical help.3,22
Our study cohorts varied in age and duration of disease; this fact is a consequence of the nature of disease. The diagnosis of type 1 diabetes usually concerns young people hence the duration of disease among these patients is usually longer. We tried to take into account an association of age and duration of disease with quality of life and satisfaction with life in both groups. We found that only patients with type 2 diabetes demonstrated a statistically significant negative correlation between age and satisfaction with life. In other literature we noticed similar findings.23,24 Another finding was a negative relationship between acceptance of the disease and anxiety and depression symptoms as well as metabolic control in both studied groups. Most researchers agree that the greater the acceptance of the disease, the lower the risk of negative emotions such as anxiety, anger, feelings of harm and depression.11,13,25,26 This relationship can have a two-way nature: the better the mental state, the less depression, fear and anxiety, the easier it becomes to accept one's life with a demanding illness. In other words, when we accept facts, we feel less tension, fear and anxiety. The relationship between the acceptance of the disease and metabolic control also seems logical. Patients accepting their disease have a greater tendency to show greater involvement in health-promoting behaviours, closely follow dietary recommendations, and undertake physical activity.27 The greater the acceptance of the disease, the better the patient's cooperation in the therapeutic process, which can be observe in the results of their HbA1c concentration in blood samples.26 Acceptance of a chronic disease can reduce stress and negative emotions that arise when diagnosed, it can be important in maintaining self-esteem as well as in the subjective perception of quality of life and the level of each person's activity in all their spheres of life.28,29 By accepting their health issue, patients express an attitude of understanding the chronicity of the disease symptoms and the awareness of its irreversible and sometimes life-threatening effects, permitting them to be more willing to undergo treatment and participate in the therapeutic process.
Our findings allow to conclude carefully that acceptance of the disease may play an important role as a preventive factor to psychological disorders such as anxiety and depression, and may be related with their quality of life, especially for those patients who live with type 1 diabetes.
Limitations of the study- 1.
The study applied a general quality of life questionnaire, a specific questionnaire would be a more appropriate choice.
- 2.
Other factors that may affect the acceptance of the disease, including medication, and other chronic diseases are not included.
- 3.
The examined cohorts differed in age as did the duration of their disease, hence our findings should be interpreted with some caution.
The Bioethics Committee of the Silesian Medical University agreed to conduct the research.
Funding1–29No funding was sought nor provided for this article.
Conflict of interestNone to declare by the authors.
The Head of the Department: Dr Hab. N. Med. Piotr W. Gorczyca profesor of Medical University of Silesia in Katowice
The Head of the Department: Prof. Dr Hab. N. Med. Janusz Gumprecht.