






Patients in palliative care are found in different places where care is provided, including the intensive care environment with important role of the nursing staff.
ObjectiveThe aim of this systematic review was to answer the following question: which nursing interventions are aimed to the palliative care patients who are in the intensive care unit (ICU).
Data sourcesUS National Library of Medicine (PUBMED), Virtual Health Library (BVS), SciELO, The Cochrane Library (Cochrane) and Lilacs databases were used.
Data extractionAfter applying inclusion and exclusion criteria in accordance with the PRISMA method, a total of 36 entries published between 2010 and 2020 were used.
Data analysisThe records extracted were analyzed from a qualitative approach, so no statistical analysis was carried out.
ResultsThe findings demonstrated that the interventions that focus on promoting the patient's autonomy and respect their needs on ICU involves effective communication, promoting shared decision with patient and family, individualize care for each patient including the family on the daily care and decisions, maintaining basic nursing care as hygiene and comfort and encouraging self-care, as well as the involvement of nursing palliative care specialists the care is important. Other interventions included promoting a continuing education program for the nursing staff and other professionals involved in caring for patients in palliative care at ICU.
ConclusionThis review highlighted the need for specific nursing interventions aimed at palliative care patients at ICU to promote patient autonomy and the focus on patient needs, always sharing decisions with the patient and family. However, it showed that there is a need for the continuous training of the nursing staff because factors such as the nurses’ lack of technical-scientific knowledge and, concomitantly, the absence of a standardized and specific intervention model linked to a bureaucratic system, make it difficult to carry out a specialized care for this type of patient.
Los pacientes en cuidados paliativos se encuentran en varios lugares, incluso en cuidados intensivos, y las enfermeras tienen un papel importante en el cuidado de este tipo de pacientes.
ObjetivoEsta revisión sistemática buscó responder a la siguiente pregunta: ¿Cuáles son las intervenciones de enfermería dirigidas a los pacientes en cuidados paliativos en la unidad de cuidados intensivos (UCI)?
Fuentes de datosBiblioteca Nacional de Medicina de EE. UU. (PUBMED), Biblioteca Virtual de Salud (BVS), SciELO, The Cochrane Library y Lilacs.
Extracción de datosAplicación de los criterios de inclusión y exclusión según el método PRISMA, totalizando 36 estudios publicados entre 2010 y 2020.
Análisis de datosLos datos extraídos se analizaron con un enfoque cualitativo, por lo que no se realizó ningún análisis estadístico.
ResultadosLas intervenciones que promueven la autonomía del paciente y respetan sus necesidades en la UCI involucran: comunicación efectiva, decisión compartida de individualizar el cuidado e incluir a la familia en el cuidado. Se debe mantener la higiene, el confort y la promoción del autocuidado, involucrando equipos de especialistas en cuidados paliativos, impulsando programas de educación continua para enfermeras de cuidados intensivos y otros profesionales implicados.
ConclusiónSon necesarias intervenciones enfermeras dirigidas a pacientes con cuidados paliativos en la UC para promover la autonomía y satisfacer las necesidades del paciente, compartiendo siempre las decisiones con el paciente y su familia, y asimismo es necesaria la formación continua de las enfermeras en factores como el desconocimiento técnico-científico de este colectivo y, concomitantemente, la ausencia de un modelo estandarizado de intervención vinculado a un sistema burocrático. Todo ello dificulta la atención especializada a este tipo de pacientes.
Palliative Care is a consolidated science mainly in the area of oncology, currently present in the most diverse environments, including the intensive care unit, due to population aging and, consequently, the emergence and advancement of chronic diseases and poor prognosis.
What it contributesGuide nurses to prescribe nursing interventions that meet the needs presented by patients in Palliative Care within the Intensive Care Unit and, thus, ensure that the care provided promotes quality of life and guarantees individualized care for this population.
Implications of the studyContribute to a better clinical practice of nurses, as the ICU is considered a hostile environment, and most professionals, especially nurses, have a deficit of training and technical/scientific knowledge to meet the demand and needs of this specific audience.
As defined by the World Health Organization (WHO), in the concept defined in 1990 and updated in 2002, “palliative care (PC) consists of care provided by a multidisciplinary team, which aims to improve the quality of life of patients and their families, in the face of a life-threatening disease, through prevention and relief of suffering, early identification, impeccable assessment and treatment of pain and other physical, social, psychological and spiritual symptoms.”1
Approximately 90 million Americans live with serious, life-threatening illnesses. And of these, about 80% of patients who die needed PC, and only half of hospitalized patients receive the PC they need.2
Patients in PC are found in different places where care is provided, including the intensive care environment. The care provided in an ICU focuses on assisting critical and highly complex patients, usually for acute illnesses, in an environment surrounded by equipment and advanced technology, with professionals who work in imminent emergency situations, with a frequent need for agility in the care provided, with a focus on technique, which provides an environment without humanization and with little interaction from family members3 and which is often described as a cold, traumatizing environment with a lot of noise, intended only for critically ill patients. In summary, the perception of the ICU is still that of a place little value on human individuality.4
According to the screening tool for inclusion of PC patients (Project IMPACT), in a general ICU population, one in seven patients, meet the PC inclusion criteria, but even when these patients undergo PC, it was observed that their needs are not met.5
In palliative care, nurses have as their main objective, to provide quality of life to these patients, in this way they work in interdisciplinary teams and seek to offer professional care that reduces suffering and promotes the comfort and dignity of the patient and family and that meets basic physical, emotional, spiritual and social health needs.4
Studies show that nurses recognize changes in patients’ health status, and these are the moments when PC can be introduced. Although the provision of PC encompasses several nursing care competencies, all nurses are particularly involved in the primary aspects of PC, which include symptom management, communication and defense.6
Some authors also evaluated the impact of PC conducted by nurses, which showed positive effects on the quality of life of patients and in reduction of medical costs.7,8
Prospective study that aimed do evaluate an intervention that involved a PC clinician and nurse interacting with the ICU physicians on daily rounds for high-risk patients on ICU identified association with more and earlier ICU family meetings and shorter hospital length of stay in these group of patients.9
In addition to the difficulties related to the implementation of specific interventions for this public, the use of electronic systems and medical records has contributed to these interventions being prescribed in an automated, bureaucratic way that only aims at the agility in performing the task, requiring the nurse to observe what must be essentially performed in the care plans and nursing developments.7
Given the above, the relevance of this systematic review can be observed, which aimed to identify evidence in the national and international literature on the need for nursing interventions aimed at patients in PC within the ICU.
MethodsSearch strategyThe study is a systematic literature review of secondary data sources collected in electronic databases, being organized according to the norms and recommendations of the PRISMA Checklist10 and registered in the International Prospective Register of Systematic Reviews (PROSPERO) under No.: CRD42020205584. The selected electronic databases were: US National Library of Medicine (PUBMED), Virtual Health Library (BVS), SciELO, The Cochrane Library (Cochrane) and Lilacs.
The preparation of this systematic review was developed following six distinct steps: (1) identification of the problem with definition of the research question; (2) establishment of inclusion and/or exclusion criteria for studies to search for scientific literature; (3) definition of the information to be extracted from the studies; (4) evaluation of studies; (5) interpretation of results and 6) presentation of the review/synthesis of knowledge.11
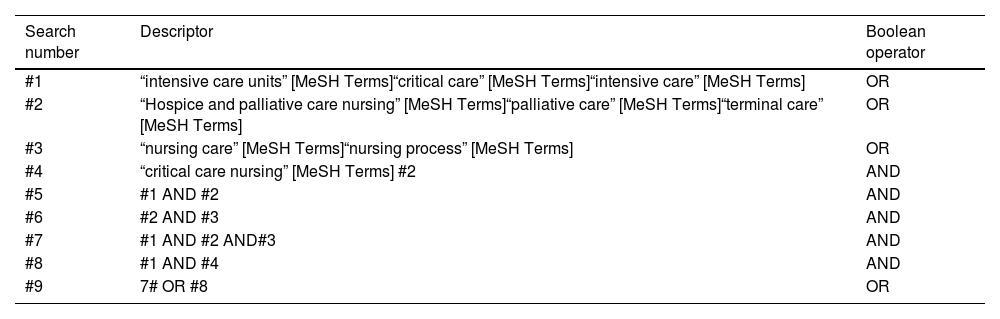
The keywords used were: “hospice and palliative care nursing”, “palliative care”, “terminal care”, “nursing care”, “nursing process”, “nursing critical care” and “critical care”. “intensive care units” and “intensive care”. The above keywords are found in Medical Subject Headings (MeSH), respectively, and were combined using the Boolean operators AND and OR. All articles that had any keyword in the title or body of the article were selected, in addition to extending the search limits to the last 10 years, all articles in English, Portuguese and Spanish of any nationality were considered. Table 1 shows the search strategy adopted all databases utilizing MeSH keywords.
Search strategy in all databases – São Paulo, 2020.
| Search number | Descriptor | Boolean operator |
|---|---|---|
| #1 | “intensive care units” [MeSH Terms]“critical care” [MeSH Terms]“intensive care” [MeSH Terms] | OR |
| #2 | “Hospice and palliative care nursing” [MeSH Terms]“palliative care” [MeSH Terms]“terminal care” [MeSH Terms] | OR |
| #3 | “nursing care” [MeSH Terms]“nursing process” [MeSH Terms] | OR |
| #4 | “critical care nursing” [MeSH Terms] #2 | AND |
| #5 | #1 AND #2 | AND |
| #6 | #2 AND #3 | AND |
| #7 | #1 AND #2 AND#3 | AND |
| #8 | #1 AND #4 | AND |
| #9 | 7# OR #8 | OR |
The articles included followed the inclusion criteria: (1) articles published in Portuguese, English and Spanish; (2) full articles that portray interventions aimed at adult patients in PC in the ICU; (3) any study design. Exclusion criteria were: (1) expert opinion, book chapters, literature review, patents, guidelines and editorials; (2) articles that were not obtained in full.
After articles selection, the results were summarized in a descriptive way.
Study selectionThe search and selection of articles by title and abstract was performed by two researchers in a dual and independent manner, organized in an electronic spreadsheet, bringing together the following topics: title, author, database, journal, year of publication, country and study objective, method, methodological rigor (Grade System) and synthesis of results. The first author selected 75 articles in his search and the second author 75 articles, totaling 75 studies. Later, there was a meeting to define the articles that would be read in full, 68 articles were selected from the previously chosen studies, based on the consensus between the pair.
Data extractionThe full reading allowed the inclusion of articles published in the selected period from 2010 to December 2020, a period in which there was a great advance in health technologies.
By December 2020, a total of 815,911 articles were obtained in the search strategy with the keywords in all databases. These were the findings in each database: PubMed: 356,217, BVS: 375,750, Scielo: 15,052, Cochrane: 813, Lilacs: 33,633 articles and other research sources: 34,446. All duplicate records were removed (n=18,750), records removed for other reasons (articles that were not available in full, books, editorials, guidelines, literature review, thesis and dissertation) were 15,846. The authors emphasize that automation tools were not used in this review.
From the total of total records screened, 781,315, a number of 706,314 were eliminated for not answering the research question, for not being in the previously selected languages, for not being studies carried out with intensive care unit patients and for not being studies carried out with patients in palliative care and/or terminal care, ending in 75 articles. So, from these, only 68 were chosen according to the eligibility of the inclusion criteria, and of these 32 articles were not available in full, approaching only medical literature and did not answer the research question, leaving 36 articles at the end (Fig. 1).
Main outcomes.")
This review aimed to answer which nursing interventions are aimed at patients in PC who are in ICU. All studies that evaluated at least one of these results were included.
Quality assessmentSubsequently, the articles founded were analyzed, and the results obtained were presented descriptively in a synoptic table containing data regarding authorship, study objective, type of study, result and conclusion. From this framework, the relevance of implementing specific nursing interventions for patients in PC within the ICU environment was demonstrated, as well as their implications in practice to guide a better care of intensive care nurses and meet the real needs of patients in PC.
After the selection of articles and journals, the results were summarized in a descriptive way.
For the reliability of the results, the authors used, in addition to the aforementioned inclusion and exclusion criteria, the methodological rigor: GRADE system (Grading of Recommendations Assessment, Development and Evaluation).
ResultsIncluded studiesA total of 75 articles that were selected, form these, only 68 were elected according to the eligibility of the inclusion criteria, but 32 articles were not available in full, approaching only medical literature and did not answer the research question, leaving 36 articles at the end (Fig. 1 – presents the PRISMA flow Diagram 2020).
Study characteristicsIt was founded 36 articles that met the inclusion criteria and answered the research question, the other studies were not selected for being part of the exclusion criteria, for being repeated and for not meeting the inclusion criteria of this review as described in method section. Table 2 shows the results of the 36 articles elected for this review. The predominant language was English with 18 articles (48.6%), followed by Portuguese with 17 articles (47.2%) and Spanish with one article (2.70%). Regarding the location of the studies: seventeen (47.2%) of them were produced in Brazil, twelve (32.4%) in the United States of America, Two (5.40%) in Canada, one (2.70%) in Spain, one (2.70%) in Norway, one (2.70%) in Israel, one (2.70%) in South Africa, one (2.70%) in England. Among the selected studies, the oldest dates are from 2010 and the most recent, from 2020, according to the study's limited search period.
Synthesis of the studies analyzed regarding authorship, study objective, type of study, result and conclusion.
| Authors/country/year | Type of study | Methodological rigor (grid system) | Study objective | Interventions and results | Implications for practice |
|---|---|---|---|---|---|
| Monteiro FF; Miriam VJ. Brazil, 2010.12 | Literature review | Low | Analyze the Brazilian scientific production on palliative care. | • Integrate and meet the patient's expectations and needs and recognize their autonomy.• Valuing palliative care within nursing interventions. | • Encourage patient autonomy in activities of daily living.• Encourage self-care during nursing care |
| Kaasalainen S, Brazil K, Willison K, Marshall D, Taniguchi A, Williams A, Wilson DM. Canada, 2011.13 | Exploratory descriptive study with a qualitative approach. | High | The objective of this study was to examine the differences between the provision of palliative care services by nurses in the rural and urban community. | • Develop best clinical practice and equip nurses with the knowledge, tools and skill sets to enable them to provide quality, specialized palliative care in a consistent and competent manner. | • Promote training in loco once a week for the team.• Conduct periodic multidisciplinary visits to clarify goals for each patient.• Include the patient in multi-professional visits. |
| Santana JCB, Wenceslau DR, Martins FS, Almeida MF, Costa MMS. Brazil, 2012.14 | Literature review | Low | Identify the nursing actions that promote palliative care in Intensive Care Units and discuss palliative care in these units. | Prescribe nursing actions with the objective of alleviating human suffering, providing a pleasant environment, respecting bathing and sleeping times, performing interventions in the most human way possible, in line with the patient's needs and the participation of family members. | • Promote daytime rest periods.• Provide a peaceful and pleasant environment.• Promote a favorable time for bathing and hygiene care according to the individual's preference.• Allow the patient to remain in the ICU without continuous monitoring. |
| Barros NCB, Oliveira CDB, Alves ERP, France ISX, Nascimento RM, Freire MEM. Brazil, 2012.15 | Exploratory descriptive study with a qualitative approach. | Moderate | Check the understanding, limits and possibilities faced by nurses to provide palliative care to patients in the ICU of a hospital in João Pessoa/PB. | • Identifying the care expressed and/or referred to by patients and family members, constitute an adequate strategy for a practice centered on the person and not just on tasks. | Identify the need for person-centered care. |
| Doorenbos AZ, Juntasopeepun P, Eaton LH, Rue T, Hong E, Coenen A. United States, 2013.16 | Cross-sectional study. | High | This study aimed to describe the nursing interventions that nurses in Thailand identify as the most important in promoting dignified dying. | • Nursing interventions to promote dignified dying: (a) maintain dignity and privacy, (b) establish trust, (c) control pain, (d) establish relationship, and (e) manage dyspnea.• Religion and culture play an important role in providing palliative care, as well as the encouragement of professional nurses to encourage holistic practices. | Establish a bond with the patient and family.Encourage religious and cultural practices and rituals in your routine. |
| Fernandes MA, Evangelista CB, Platel ICS, Agra, G, Lopes MS, Rodrigues FA. Brazil, 2017.17 | Exploratory descriptive study with a qualitative approach. | Moderate | Knowing the nurse's perception of cancer patients under palliative care. | • Use communication as an essential element of care for the patient and family under palliative care. | Encourage communication between patient and nursing staff.Perform listening therapy. |
| Dacher JE. United States, 2014.18 | Literature review | Low | The purpose of this article is to provide critical care nurses with information about the practice of palliative care with critically ill elderly patients, as well as evidence-based content and resources, allowing for the defense of palliative care in their own work environments, accompanied by the necessary resources that will support efficient implementation. | • Promote holistic, comprehensive and individualized care, involve the family, promote autonomy and include patients as much as possible in decision-making.• Adjust nursing interventions according to the physiological changes and age of each patient. | • Encourage holistic care and practices.• Promote patient autonomy.• Individualize care according to the age and physiological needs of each patient. |
| Susín ABP, Arzoz EY, Fernández MS, Ros EZ, Calatayud MV. Spain, 2015.19 | Literature review. | Moderate | Knowing the perceptions, experiences and knowledge of intensive care nurses in the care of terminal patients. | • Respect the patient's dignity and provide a personalized service aimed at well-being to promote a “good death”.• Optimize the environment for noise and routine procedures.• Leave the family with loved ones as long as possible and facilitate their inclusion in care. | Promote patient well-being.Make visiting hours more flexible. Allow the presence of full-time companions. |
| Silva RS, Pereira A, Mussi FC. Brazil, 2015.20 | Exploratory descriptive study with a qualitative approach. | Moderate | Knowing the meaning of nursing care for a good death from the perspective of an intensive care nurse. | • Plan therapeutic interventions for people in the terminal process to alleviate current discomfort and promote well-being.• Promote practices focused on relieving physical and emotional discomfort and providing social support. | Provide comfort and well-being to the patient.Identify practices that accentuate discomfort, such as repeated exam collections.Request follow-up from the multidisciplinary team (psychology and social worker, among others) |
| Fitch MI, Fliedner MC, O’Connor M. Canada, 2015.21 | Literature review | Low | Outline nursing perspectives in relation to early palliative care, highlighting the role nurses can play in the process, the identified challenges and barriers that currently impede the performance of these roles and possible solutions to the barriers. | • Make any necessary adjustments to meet the person's needs.• Include family members and other important people in the care plan. | Encourage individual comfort and well-being practices.Integrate family members and important people in patient care. |
| Tornoe K, Danbolt LJ, Kvigne K, Sorlie V. Norway, 2015.22 | Exploratory descriptive study with a qualitative approach. | Low | Illuminate the experience of a nursing teaching team in a pioneering Norwegian hospice by teaching and training spiritual and existential care workers for the dying in nursing homes | • Develop existential and spiritual conversations that can convey comfort through active presence and silence.• Encourage and address the spiritual and existential suffering of palliated patients. | Provide therapeutic conversations and active listening during the shift. |
| Kisorio LC, Langley GC. South Africa, 2016.23 | Exploratory descriptive study with a qualitative approach. | High | Explore the experiences of intensive care nurses about end-of-life care in adult intensive care units. | • Support religious and spiritual practices.• Prescribe measures to reduce noise.• Allow the patient's family to visit at any time of the day without restrictions.• Prescribe specific interventions for comfort until death and pay careful attention to the families of the sick. | Allow religious teachers to visit.Promote moments of silence throughout the day.Allow unrestricted entry of family members.Perform comfort massage.Perform decubitus changes every 2h. |
| Silva RS, Santos RD, Evangelista CL, Marinho CLA, Lira GG, Andrade MS. Brazil, 2016.24 | Exploratory-descriptive and cross-sectional study. | Moderate | Knowing the perception of family members about the role of the nurses’ in the care of patients in palliative care | • Promote the link between the palliative care team and the care unit team. | Request evaluation from the multidisciplinary team whenever necessary. |
| Silveira NR, Nascimento ERP, Rosa LM, Jung W, Martins SR, Fontes MS. Brazil, 2016.25 | Exploratory descriptive study with a qualitative approach. | Moderate | Know the nurses’ feelings about palliative care in adult intensive care units. | • Offer physical comfort care, such as reducing pain/suffering with the adoption of non-pharmacological measures.• These care and comfort measures must be congruent with the patient's wishes. | Encourage meditation techniques and breath control.Encourage entertainment activities. |
| Ramos KJ, Downey L, Nielsen EL, Treece PD, Shannon SE, Curtis JR, Engelberg RA. United States, 2016.26 | Cross-sectional study | Moderate | Our aim was to identify appropriate communication aspects for interventions to improve the quality of dying in the intensive care unit (ICU). | • Exchange information mainly between nurses, doctors and patients about their main desires to promote a better quality of death for patients. | Encourage dialogs that allow the patient to express their desires, anxieties and anxieties. |
| Santos EC, Oliveira ICM, Feijão AL. Brazil, 2016.27 | Cross-sectional study | Moderate | The objective of this research was to describe the process of content validation of nursing care protocol for patients in palliative care hospitalized in the ICU. | • Encourage practices such as: acupressure, electro-acupuncture, shiatsu, reflexology, aromatherapy, meditation, art therapy, flower therapy, reiki, therapeutic touch, psychotherapy, acupuncture, massage, body relaxation techniques and music therapy. | • Explain about non-pharmacological techniques to the patient.• Promote symptom relief through non-pharmacological techniques according to the patient's preference.• Promote therapy with dogs. |
| Silva MM, Buscher A, Moreira MC. Brazil, 2016.28 | Exploratory descriptive study with a qualitative approach. | Moderate | The aim of this study was to provide insights into the Brazilian palliative care system from the perspective of nurses and physicians. | • Integrate and organize services and staff to optimize resources and prescriptions to promote specific care that meets the needs of patients at this stage of life. | • Prescribe specific and personalized interventions for each patient. |
| Lutz BJ, Green T. United States, 2016.29 | Literature review | Low | The purpose of this article is to provide an overview of palliative care in stroke patients and to present recommendations for nurses who care for stroke patients and their families. | • Ensure essential nursing care (e.g., oral hygiene, changing positions, bathing, oxygen therapy, symptom/pain control, comfort and support). | • Bathe in bed.• Perform oral hygiene after meals.• Apply dressings.• Apply adequate pain scale and promote pain management.• Perform body hydration. |
| Gulini JEHMB, Nascimento ERP, Moritz RD, Rosa LM, Silveira NR, Vargas MAO. Brazil, 2017.30 | Exploratory descriptive study with a qualitative approach. | Moderate | Knowing the perception of health professionals in an ICU bout palliative care. | • Relieve symptoms, respect wishes and allow the presence of loved ones without restriction. | • Carry out management of signs and symptoms.• Allow small celebrations and meetings within the hospital environment |
| Gerritsen RT, Koopmans M, Hofhuis JGM, Curtis JR, Jensen HI, Zilstra JG, et al. United States, 2017.31 | Cross-sectional study | Moderate | Evaluate the end-of-life experiences measured by QODD (Quality as Dying and Death Perceived**) completed by families and nurses in the United States and the Netherlands to explore similarities and differences in these experiences and identify opportunities to improve end-of-life care * *Comparing the quality of dying and assisted dying | • Ensure that the patient can eat, laugh or smile, spend time alone and with family, say goodbye, and allow a spiritual counselor to be present. | • Allow food consumption according to the patient's preferences.• Promote a less restrictive diet.• Provide moments of pleasure and relaxation.• Allow the performance of religious rituals. |
| Wysham NL, Hua M, Hough CL, Gundel S, Docherty SG, Jones DM, et al. United States, 2017.32 | Study of mixed methods. | Moderate | Addressing the quality gap in ICU-based palliative care is constrained by uncertainty about acceptable expert models in collaboration and generalist care. Therefore, we characterize the attitudes of doctors and nurses toward providing palliative care in an ICU environment. | Integrate specialists in palliative care in the ICU. | Request assessment from the palliative care team.Watch for signs of depression/chronic sadness. |
| Boyle DA, Barbour S, Anderson W, Noort J, Grywalski M, Myer J, Hermann H. United States, 2017.33 | Qualitative, descriptive and exploratory study. | Low | Describe the development, implementation and outcomes of an integration of multidisciplinary palliative care in the ICU, to teach ICU nurses specific communication skills for palliative care. To identify collaboration options between oncology and intensive care nurses when integrating palliation into the planning of nursing care. | • Identify communication gaps and barriers between professional nurses and patients and their families and set goals to improve communication. | • Promote effective communication with patients and families.• Address the needs that are presented by patients.• Watch out for hypoactive delirium. |
| Brabo BCF, Laprano MGG. Brazil, 2018.34 | Qualitative, descriptive and exploratory study. | Moderate | To analyze the professional competences of nurses for palliative care in a Cardiac Intensive Care Unit. | • Implement and anticipate measures to ensure the adequate provision of care to patients who are in palliative care. | • Promote individualized care for each patient in PC. |
| Pedrão TGG, Brunori EHFR, Santos ES, Bezerra A, Simonetti SH. Brazil, 2018.35 | Quantitative and cross-sectional study | Moderate | Characterize the clinical and socio-demographic profile and identify the main nursing diagnoses and interventions. | • Alleviate signs and symptoms and prioritize each patient. | • Communicate to the nurse about symptoms such as nausea and vomiting.• Encourage walking and outdoor activities to relieve symptoms. |
| Agarwal R, Epstein AS. United States, 2018.36 | Literature review. | Low | Highlight the importance, challenges and evolution of advance care planning for cancer patients. | • Carry out early palliative care interventions.• Support patients and families to make informed and consistent decisions regarding end-of-life treatments. | • Educate family members and patients about end-of-life treatments.• Promote patient comfort and quality of life. |
| Cassel JB, Albrecht TA. United States, 2018.37 | Literature review | Low | Describe the integration of palliative care in oncology, including various models that facilitate this integration, important considerations when starting a program, special cancer populations that would benefit from palliative care, and challenges to consider. | • Provide and prescribe early and primary palliative care.• Facilitate relationships with the patient and meet their needs. | • Promote well-being.• Encourage therapeutic listening.• Identify signs of anxiety and try to reduce them. |
| Davies EA. England, 2018.38 | Narrative review. | Low | The aim of this article is to identify the different ways in which poetry has been used in palliative care and to reflect on its future potential for education, practice and research. | • Implement poetry as an important tool to search for meaning, find some pleasure in a situation.• Employing poetry as a mantra in the form of some short poem to help patients control their breathing as part of palliative care to treat symptoms such as shortness of breath. | • Recite poems.Stimulate the reading habit.• Encourage outdoor physical activities.• Encourage outdoor reading and recreation activities.• Situate the patient in time and space. |
| Pegoraro MMO, Paganini MC. Brazil, 2019.39 | Qualitative, descriptive and exploratory study. | Moderate | To investigate the knowledge of the multidisciplinary team about the relationship between palliative care and limited life support and build multidisciplinary actions on the subject for patient care. | • Prescribe nursing care, such as hygiene and body hydration, in addition to oral hygiene, dressing change, in order to maintain the patient's dignity and quality of life.• Respect the privacy and wishes of the conscious patient. | • Assist the spray bath.• Moisturize your skin three times a day.• Guide before performing the procedures.• Avoid unnecessary exam collections.• Daily reassess the use of venous access and invasive devices. |
| Cavalcanti IMC, Oliveira LO, Macêdo LC, Leal MHC, Morimura MCR, Gomes ET. Brazil, 2019.40 | Descriptive and cross-sectional study | Moderate | Objective to assess the perception of intensive care nurses about adherence to the principles of palliative care in their care practice. | • Prescribe care related to pain and symptom relief.• Adequate bathing, change of position, administering opioids, controlling dyspnea, sedation care, nutrition and hydration of the skin and mucous membranes. | • Promote adequate sedation and analgesia.• Assess the skin daily and take measures against skin and mucosal lesions.• Pay attention to delirium.• Perform therapeutic touch twice a day. |
| Lopes LL, Batista PSS, Lima DRA, Oliveira AMM, Costa KC. Brazil, 2019.41 | Qualitative, exploratory study. | Moderate | To investigate the understanding of nurses about palliative care for patients assisted in the hospital environment. | • Continuously educate nurses so that they are able to carry out a NCS that aims at specific care for these patients. | Promote courses and periodic training for the nursing staff. |
| Gaspar RB, Silva MM, Zepeda KGM, Silva IR. Brazil, 2019.42 | Qualitative, exploratory study. | Moderate | Understand how nurses deal with the autonomy of the elderly at the end of life. | • Promote dialog between the health team and family and contribute to patient-focused decision making. | • Guide family members and clarify doubts, including the patient's. |
| Haron Y, Romem A, Greenberger C. Israel, 2019.43 | Cross-sectional study | Moderate | To present the characteristics of nursing professionals in Israel, the extent of their role and practice, activities, role responsibilities and job satisfaction. | • Develop protocols for nurses’ autonomy in relation to complex interventional procedures, including the prescription of narcotic drugs. | Optimize patient analgesia.Avoid futile invasive measures. |
| Collett D, Feder S, Aaron E, Haron Y, Schulman-Green D. United States, 2019.44 | Qualitative descriptive study. | High | Describe the development of advanced practice in palliative care in Israel and support the development of the role of registered nurse of advanced practice in other specialties. | • Increase training paths and solve problems in the practice of nursing functions. | • Encourage nurses’ autonomy in decision-making with the patient. |
| Wolf AT, White KR, Epstein EG, Enfield KB. United States, 2019.45 | Descriptive quantitative study. | Moderate | To examine the knowledge perceived by critical care nurses about palliative care, their recent experiences of moral distress and the possible relationships between these variables. | • Prioritize training in palliative care for intensive care nurses and train them to reduce barriers to palliative care, and provide an appropriate model of care for this audience. | • Conduct periodic training for the nursing staff.• Provide a model of specific interventions for this audience. |
| Frey R, Balmer D, Boyd M, Robinson J, Gott M. United States, 2019.46 | Quali-quantitative analysis | Moderate | Exploring knowledge of palliative nurses in the experiences of the benefits and barriers of implementing an educational intervention in palliative care | • Continuously educate professionals in palliative care and emphasize key palliative care. | • Continuously educate health professionals in the field of palliative care. |
| Santo AM, Narciso AC, Evangelista CB, Filgueiras TF, Costa MML, Cruz RAO. Brazil, 2020.47 | Qualitative, descriptive and exploratory study. | Moderate | Analyze the perception of nurses about their experience in palliative care. | • Promote comfort, which must be done individually according to the needs of each patient.• Provide differentiated care, permeated by the principles of humanization, multidisciplinary work, valuing quality of life, comfort, pain control and family interaction. | • Promote pain relief and reassess every 1h.• Promote moments of comfort and rest during the day.• Promote a peaceful environment conducive to sleep. |
From the selected studies, the demographic data of most participants were as follows: the mean age was 62 years. The patients were mostly women (56.8%) and most participants identified their ethnicity as white or Caucasian (69.3%), in addition, most were cancer patients who were hospitalized in an ICU and terminal phase of life.
DiscussionThe main nursing interventions found were related to factors such as: focus in the patients’ needs and promoting the patient's autonomy, promoting a continuing education program for the nurses’ staff and other professionals involved in caring for patients in PC, promoting the practice of holistic activities and developing beliefs/faith, including family members in care, effective communication, promoting differentiated and individualized care schedules for each patient, maintaining basic nursing care, as well as the involvement of professional PC specialists in care.
The nursing prescription is a private activity of the nurse, where nursing interventions are prescribed aimed at improving and/or solving the nursing problems found. Nursing interventions in PC are intended to promote the relief of suffering and discomfort, in addition to meeting the demands of care presented by these patients who are in PC and even in the terminal phase.19,20 There is an emphasis on respect, privacy, and the wishes of the conscious patient, welcoming and integrating the family into care.37,39
PC interventions provided by the nursing staff have a positive and significant impact on improving quality of life and consequently reducing the distress of the patients.48
Other authors report that nurses should evaluate patients clinically and thus establish individual care priorities35 always aiming to meet their expectations and needs, encouraging and recognizing the patient's autonomy,12 developing, from this, a plan of specific interventions for the resolution of the signs and symptoms presented.40
It is important to direct nurses actions to transform a hostile environment, such as the ICU, into an adequate environment for the provision of care,18 aiming at a practice centered on the person and not just on tasks, it is essential that nurses provide a pleasant environment, provide rest times, respect the bath time according to the patient's preference, and provide flexible visiting hours, release the presence of a companion and encourage the family's participation for as long as possible.14,15,23,47,49
Among results founded, it was emphasized the need to make adjustments in nursing interventions, adapting them according to the physiological changes, age and desires of each patient, seeking to promote measures of comfort and well-being and encourage practices to autonomy of the patient in decision-making.25,30
Studies have shown that hospitalized patients with some type of incurable disease and in an advanced state should receive PC from the beginning of the disease course, concomitantly with curative treatment; thus, early PC interventions can positively integrate care planning to support to the patients and their families, especially in making congruent decisions regarding end-of-life treatments.36,50
It has been shown that many non-pharmacological and holistic interventions are important for these patients, and the nurse should be a supporter of such practices, such as stimulating beliefs, meditation, music therapy, relaxation techniques, flower therapy, art therapy, among others, these measures proved to be effective concerning to controlling symptoms such as pain, dyspnea and providing physical, emotional and mental well-being for these patients.16,18,27,43
Therefore, spiritual symptoms are strictly related to psychosomatic symptoms that involve terminal illnesses and affect the well-being of patients in PC, spiritual coping can help to alleviate this feeling.51 Studies show the link between spirituality and relief of symptoms that affect patients in PC, such as spiritual anguish,52,53 anxiety,54,55 depression32,56 and chronic pain.57
Furthermore, the stimulus of poetry as a nursing intervention to alleviate shortness of breath. He explains that short poems like mantras associated with breathing control exercises help with dyspnea.38
Another non-pharmacological intervention that helps in PC for the patient is communication, among the articles researched, many emphasize its relevance, as it is an essential element in care and decision-making, because through it the nurse can get so close the patient and family, thus promoting dialog between the multidisciplinary team and family members so that decision-making focused on the patient is made.17,24,41 Communication can also be a technique to alleviate the spiritual and existential suffering of patients ‘palliates and assist in the transmission of comfort through active listening and silence.22
It should be noted that essential nursing care such as oral hygiene, position changes, bathing, dressings, skin hydration, oxygen therapy, symptom control (especially pain), and other support to ensure the quality of life, are extremely important and should be maintained29 and the planning of these actions should be developed based on the exchange of information between the multidisciplinary team, taking into account the family dynamics, spiritual and cultural issues, and the patient's wishes.26 It is evident that there is still much to be done regarding the integration between the team, services, family, optimization of resources, interventions, and promotion of specific care that meet the needs of palliative patients.29
Another relevant topic was the need for continuous and constant training focused on this theme, as it was evidenced in 9 articles (25%) that it is extremely important that nurses have adequate skills and knowledge so that they can carry out specific and effective interventions to ensure the quality for the patient in PC.12,33,34,44
A comparative study between a Dutch ICU and an ICU in the United States showed that the nurse in the Dutch ICU, for having more autonomy in the decision-making process, including life decisions, enables a more effective, early, and adequate care plan for each patient, unlike the ICU in the United States, where nurses explained that the most relevant actions for this type of patient are: having self-control, being able to eat, laughing, spending time alone or with the family, measures that can be supplied with an individual care plan.3
Many of the ICU nurses do not feel prepared to provide PC; therefore, training in PC for intensive care nurses is of utmost urgency, in addition to offering and providing an appropriate nursing interventions model for this audience.45 In addition, professional nurses have a deficit in academic training about the prescription of care for patients in PC, a process of continuing education is necessary so that they can provide assistance that aims at specific and humanized care for these patients.41,46
The nurse's role is to ensure and prescribe that nursing interventions are specifically aimed at the patient in PC within the ICU, with an emphasis on ensuring and providing individualized, specific, and humanized nursing care, to allow patients to complete their life cycle with dignity, respect and with as little suffering as possible.
Strengths and limitationsOne strength of this study is that we obtained a wider perspective on the nonpharmacological interventions for patients with PC in ICU compared to previous reviews. It is believed that this study can contribute to better nursing care for patients on PC, but it is necessary to further explore this area of research.
Two independent reviewers coded all studies with is consistent with best practices.
This study had as limitations the scarcity of randomized studies available in the literature, so it was included all types of studies found as reviews, qualitative analysis, among others, which means our results could be biased due to some studies that could have low methodological quality. These biases should be corrected in future randomized or non-randomized trials. Future research for higher quality randomized controlled trials are desirable.
ConclusionThis study highlighted the need for specific nursing interventions aimed at PC patients within an ICU, but factors such as the nurses’ lack of technical-scientific knowledge and concomitant with this, the lack of time and a model of standardized and specific interventions linked to a bureaucratic system, makes it difficult to carry out specialized care for this type of patient, it was observed that it is necessary to provide exceptions in the care provided to patients in PC to increase their quality of life, well-being, comfort, encourage their autonomy and promote a die worthily.
Conflict of interestThe authors declare no conflict of interest.
The authors declare that they have not received any type of incentive in the form of scholarships, scholarships or financial support.

