





To analyse, from a gender perspective, the characteristics and perception of the effects of leadership of nurses in a hospital of the Andalusian Public Health System.
MethodologyQualitative study with a phenomenological approach. The participants were nurses in care and intermediate positions with a contract of more than 6 months. A qualitative content analysis was carried out. Four phases were established for data analysis, from which 5 categories resulted. NVivo 11 software was used to analyse the dialogues.
ResultsThe participants’ discourses endow the leader with characteristics that define him as a reference person. The contribution of middle management is necessary for the achievement of the objectives of the care units and the cohesion of the group, although this group perceives it only in relation to the management of resources. Access to management positions is not linked to gender.
ConclusionsThe participants’ discourses endow the leader with characteristics that define him as a reference person. The contribution of middle management is necessary for the achievement of the objectives of the care units and the cohesion of the group, although this group perceives it only in relation to the management of resources. Access to management positions is not linked to gender.
Analizar, con perspectiva de género, las características y percepción de los efectos del liderazgo de las enfermeras y enfermeros de un hospital del Sistema Sanitario Público Andaluz.
MetodologíaEstudio cualitativo con enfoque desde la fenomenología. Los/as participantes fueron enfermeras asistenciales y con cargos intermedios con contrato mayor a 6 meses. Se realizó un análisis de contenido cualitativo. Se establecieron 4 fases para el análisis de datos, de donde resultaron 5 categorías. Se utilizó el software NVIVO 11 para el análisis de los diálogos.
ResultadosLos discursos de los participantes dotan al líder de características que lo definen como una persona referente. La contribución de los mandos intermedios es necesaria para la consecución de los objetivos de las unidades asistenciales y cohesión del grupo, aunque este grupo la perciben solo en relación al manejo de los recursos. El acceso a cargos de gestión no tiene vinculación con el género.
ConclusionesEl estilo de liderazgo predominante en los cargos intermedios del Hospital de Lebrija es reconocido como un liderazgo participativo, esencial para el mantenimiento de la gestión eficiente y favorecedor de la promoción y la igualdad entre profesionales; no identificándose sesgos de género en el acceso a dichos cargos.
The question of nursing leadership in management positions has hardly been examined in Spain, given that the majority of scientific studies cover the leadership of care nursing.
What it contributesThis underlines the importance of management professionalization, the need to establish specific programmes for management and the importance of including gender-based criteria for access to management positions.
The current healthcare system is undergoing a profound change. The inversion of the population curve and the increase in chronic disease make it necessary to modify the pattern of healthcare to ensure that it is sustainable over the medium to long term.1–3
This is why it is necessary in the current healthcare context to have unifying leaders of Nursing who function as the nexus connecting different professionals.4,5 There are few studies in this area, as the majority centre on leadership styles rather than the application of leadership itself; thus authors such as Lara et al.6 underline a transformational leadership style as the guiding thread for successful healthcare management.7
Furthermore, in a profession that is as feminized as nursing, it is necessary to underline the importance of a gender-based approach, as women are under-represented in management positions.8 Women have traditionally been considered to have a more maternalistic management style, as opposed to men who stand out for personal domination and impersonality.9,10
On the other hand, the nursing collective working in care has to deal with bureaucratic aspects and complex situations with limited resources, so that there is a need for motivated leaders who are able to bring about an effective improvement in the quality of care.11,12
The nursing profession therefore seeks to obtain its due recognition and legitimacy within the healthcare structure, where it has long experience in the formal leadership by management, as well as in the informal leadership by care teams.9,13 An example of this is the concept of Magnet Hospitals, where the nursing profession is the pillar that supports the organization.14
The objective of this work is to undertake a gender-based analysis of the characteristics and perceptions of the effects of nursing leadership in an Andalusian Public Health Service hospital.
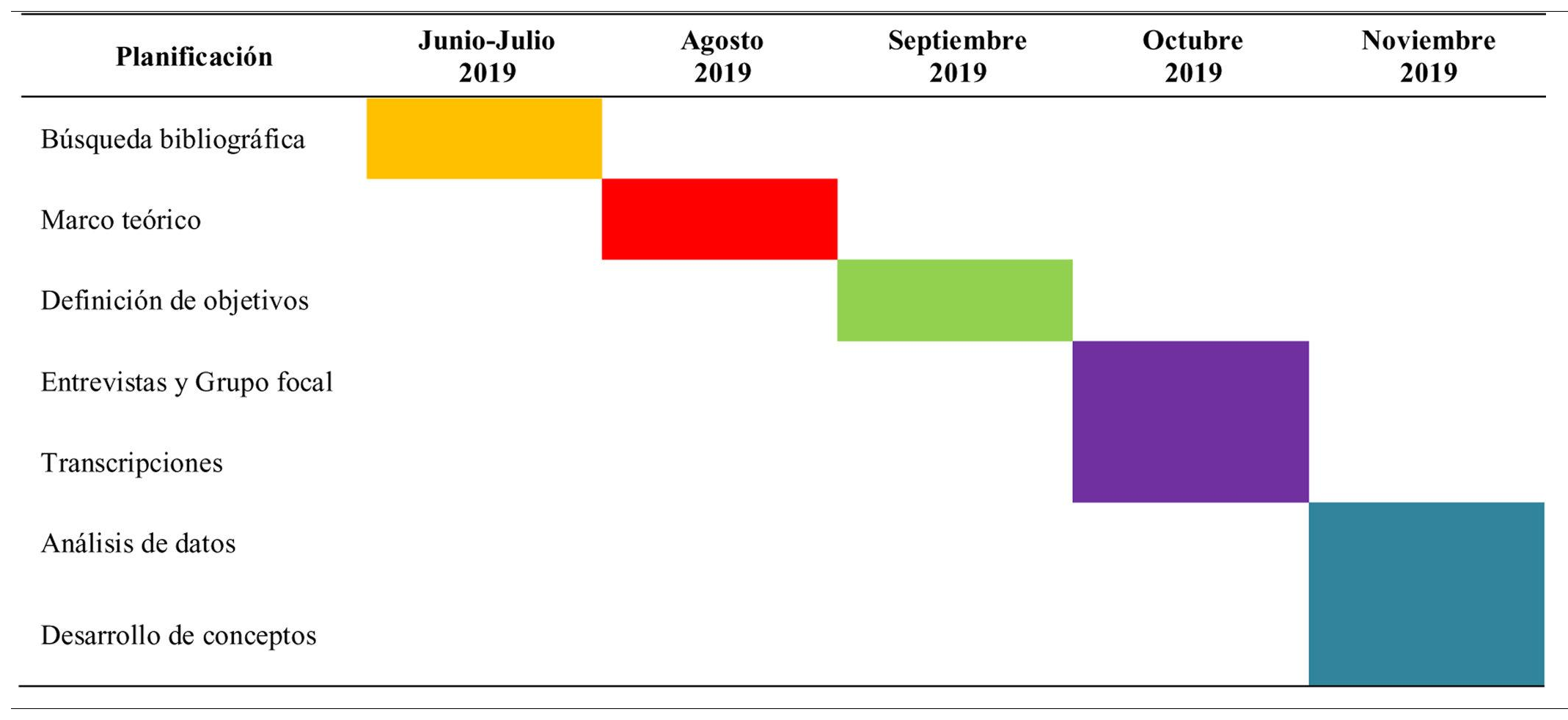
MethodDesignA qualitative study based on a phenomenological approach was prepared, where the opinions and experiences of male and female nurses in management and caring roles were analysed. The study commenced in June 2019 and ended in November 2019. It took place in Lebrija HAR.
ParticipantsIntentional convenience sampling was performed. For leadership analysis it was necessary to include intermediate Nursing management levels as well as nursing staff with care-based tasks.
The inclusion criteria were possession of a diploma and/or degree in nursing together with experience longer than 6 months in any department of Lebrija HAR at the time of the study. The exclusion criterion of having less than 6 months’ experience was specified.
Data gatheringSemi-structured interviews and focus groups were selected to gather information, and they took place in October 2019.
Interviews were conducted with the middle managers, to record their acquired experiences and maintain a coherent and consistent discourse. The nurses involved in care tasks were interviewed in a focus group, to favour their interaction and the richness of their dialogue.
The meeting room of the hospital was used for the interviews as well as for the focus group, to ensure a relaxed atmosphere that was free of interruptions.
The influence of the interviewer was controlled during the data gathering process, and they played the role of a simple moderator.
Before the interview the participants were given a document providing information about the study and an informed consent form.
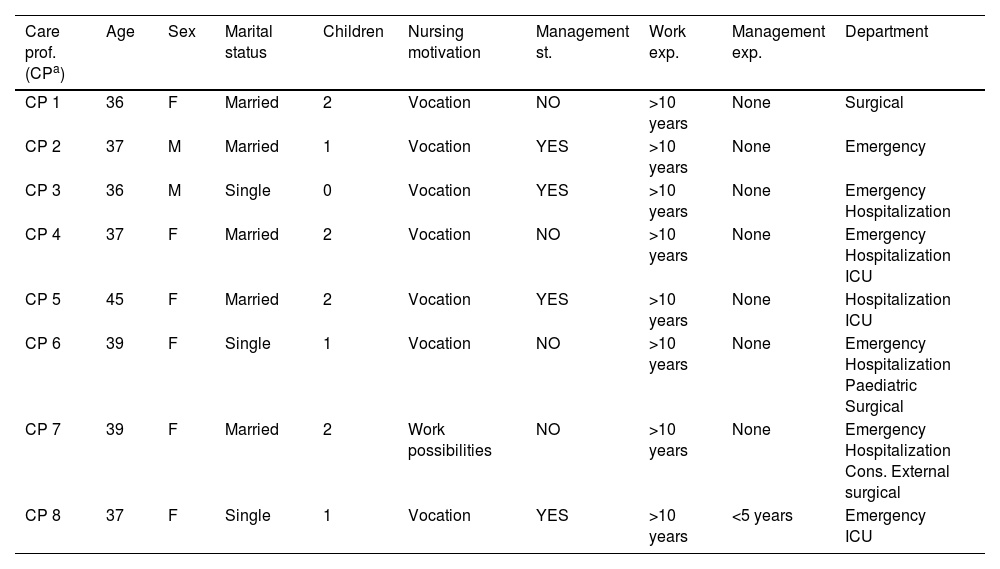
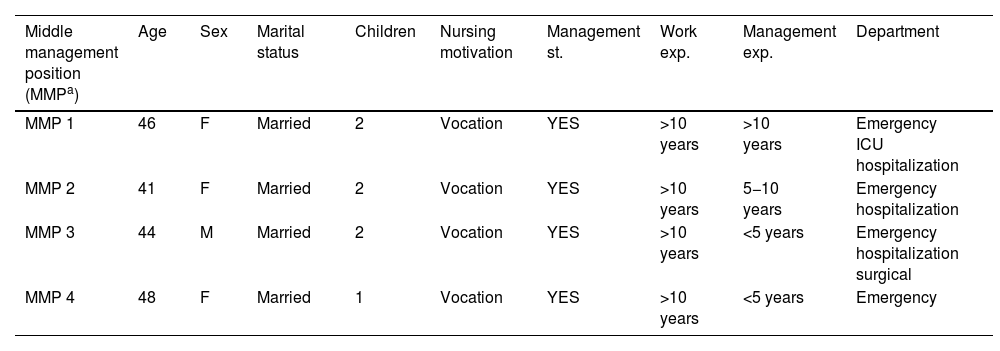
Once they had accepted to take part, their sociodemographic data were recorded to complement the data gathering (Tables 1 and 2).
Sociodemographic data of the focus group.
| Care prof. (CPa) | Age | Sex | Marital status | Children | Nursing motivation | Management st. | Work exp. | Management exp. | Department |
|---|---|---|---|---|---|---|---|---|---|
| CP 1 | 36 | F | Married | 2 | Vocation | NO | >10 years | None | Surgical |
| CP 2 | 37 | M | Married | 1 | Vocation | YES | >10 years | None | Emergency |
| CP 3 | 36 | M | Single | 0 | Vocation | YES | >10 years | None | Emergency Hospitalization |
| CP 4 | 37 | F | Married | 2 | Vocation | NO | >10 years | None | Emergency Hospitalization ICU |
| CP 5 | 45 | F | Married | 2 | Vocation | YES | >10 years | None | Hospitalization ICU |
| CP 6 | 39 | F | Single | 1 | Vocation | NO | >10 years | None | Emergency Hospitalization Paediatric Surgical |
| CP 7 | 39 | F | Married | 2 | Work possibilities | NO | >10 years | None | Emergency Hospitalization Cons. External surgical |
| CP 8 | 37 | F | Single | 1 | Vocation | YES | >10 years | <5 years | Emergency ICU |
Sociodemographic data of the middle management positions.
| Middle management position (MMPa) | Age | Sex | Marital status | Children | Nursing motivation | Management st. | Work exp. | Management exp. | Department |
|---|---|---|---|---|---|---|---|---|---|
| MMP 1 | 46 | F | Married | 2 | Vocation | YES | >10 years | >10 years | Emergency ICU hospitalization |
| MMP 2 | 41 | F | Married | 2 | Vocation | YES | >10 years | 5−10 years | Emergency hospitalization |
| MMP 3 | 44 | M | Married | 2 | Vocation | YES | >10 years | <5 years | Emergency hospitalization surgical |
| MMP 4 | 48 | F | Married | 1 | Vocation | YES | >10 years | <5 years | Emergency |
A chronogram of the activities undertaken during the study was prepared (Table 3).
Data analysis
4 of the 5 middle managers who fulfilled the inclusion criteria were interviewed (80%); of these, two were women and two were men. The average age of this group was 44.75 years, and their average time in their position was 6 years.
Of the 46 professionals working in care (36 women and 10 men) who fulfilled the inclusion criteria, a focus group was held with a total of 8 participants (17.39%), of whom 6 were women (75%) and 2 were men (25%).
The average age of the focus group respondents was 38.25 years; only one respondent was aged over 40 years (45 years). The others were aged from 36 to 39 years.
The recorded discourse was transcribed literally using NVIVO11 Transcription software. The recommendations of Calsamiglia & Tusón15 were followed for the transcriptions, as a measure to analyse phonetic as well as linguistic aspects.
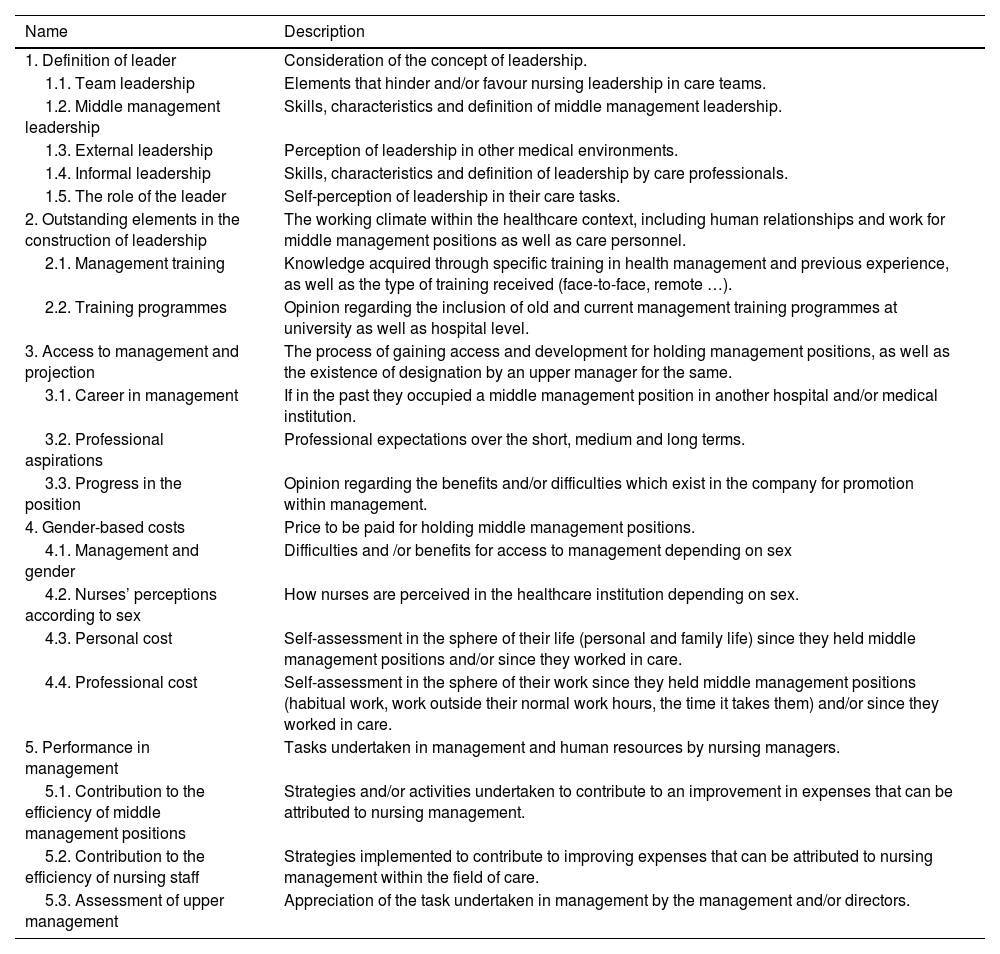
The process of analysis was based on the construction of a table of theoretical categories (Table 4), without ruling out any possible emerging categories that may arise during the reading process. Subsequently the content was analysed following the recommendations of Gil-García.16
Definitive matrix of categories with definitions.
| Name | Description |
|---|---|
| 1. Definition of leader | Consideration of the concept of leadership. |
| 1.1. Team leadership | Elements that hinder and/or favour nursing leadership in care teams. |
| 1.2. Middle management leadership | Skills, characteristics and definition of middle management leadership. |
| 1.3. External leadership | Perception of leadership in other medical environments. |
| 1.4. Informal leadership | Skills, characteristics and definition of leadership by care professionals. |
| 1.5. The role of the leader | Self-perception of leadership in their care tasks. |
| 2. Outstanding elements in the construction of leadership | The working climate within the healthcare context, including human relationships and work for middle management positions as well as care personnel. |
| 2.1. Management training | Knowledge acquired through specific training in health management and previous experience, as well as the type of training received (face-to-face, remote …). |
| 2.2. Training programmes | Opinion regarding the inclusion of old and current management training programmes at university as well as hospital level. |
| 3. Access to management and projection | The process of gaining access and development for holding management positions, as well as the existence of designation by an upper manager for the same. |
| 3.1. Career in management | If in the past they occupied a middle management position in another hospital and/or medical institution. |
| 3.2. Professional aspirations | Professional expectations over the short, medium and long terms. |
| 3.3. Progress in the position | Opinion regarding the benefits and/or difficulties which exist in the company for promotion within management. |
| 4. Gender-based costs | Price to be paid for holding middle management positions. |
| 4.1. Management and gender | Difficulties and /or benefits for access to management depending on sex |
| 4.2. Nurses’ perceptions according to sex | How nurses are perceived in the healthcare institution depending on sex. |
| 4.3. Personal cost | Self-assessment in the sphere of their life (personal and family life) since they held middle management positions and/or since they worked in care. |
| 4.4. Professional cost | Self-assessment in the sphere of their work since they held middle management positions (habitual work, work outside their normal work hours, the time it takes them) and/or since they worked in care. |
| 5. Performance in management | Tasks undertaken in management and human resources by nursing managers. |
| 5.1. Contribution to the efficiency of middle management positions | Strategies and/or activities undertaken to contribute to an improvement in expenses that can be attributed to nursing management. |
| 5.2. Contribution to the efficiency of nursing staff | Strategies implemented to contribute to improving expenses that can be attributed to nursing management within the field of care. |
| 5.3. Assessment of upper management | Appreciation of the task undertaken in management by the management and/or directors. |
Four phases were established; in the first phase a tree of theoretical categories and subcategories agreed by the research team was created; in the second phase the transcribed texts were examined again to identify emerging categories. These categories were then triangulated by the researchers. In the third phase fragments of text were linked and assigned to the established categories as suggested by Seidel and Kelle.17 Finally, in the fourth phase the codification of the texts was reviewed once again, with the aim of unifying criteria in preparing units of meaning, passing from a dissociative stage to another synthetic stage in which grouping took place based on the resulting categories, obtaining the definitive material for the preparation of the report on findings.
NVIVO 11 plus software was used for data analysis. This software was used as a tool for the inclusion of data and the classification and analysis of the information gathered.
Ethical considerationsThis study was carried out under the terms of the Data Protection Regulation (EU) 2016/679 of the European Parliament and Council of 27 April 2016 (RGPD), of Organic Law 3/2018, of 5 December, on the Protection of Personal Data and Guarantee of Digital Rights (LOPD), as well as the Helsinki Declaration.18 This study is the first phase of a broader project which has been approved by Huelva Provincial Ethics Committee of the Andalusian Health Service, the Health and Families Board of the Regional Government of Andalusia, under code 0080-N-23.
Furthermore, given that the study was undertaken with professionals in Lebrija Hospital, the usual process was followed for works in this institution at the time by requesting authorization through an informative and consent document from the management of the hospital (Appendix A). In the same way, prior to the interview all of the respondents were given the informative and informed consent document, This emphasised the voluntary nature of participation, as well as the possibility of refusing to take part in the study at any time, under the terms of ARCOPOL rights (Appendix B).
Finally, Amnesia anonymization software was used for data processing, so that the risk of identifying the participants was eliminated while maintaining their true identity. The head of the Emergency Department held the information in custody, and finally a time limit for the destruction and erasure of the files containing the data was set at 2 years after the end of the study.
ResultsThe results were grouped in 5 sections, each one of which corresponded to one of the study categories (Table 4).
Definition of a leaderThe figure of the leader was considered in all of the discourses to have a series of special characteristics which made them important, positive and able to motivate.
In the focus group the men identified the high workload in care as hindering leadership, while the women only referred to the characteristics of the leaders themselves as they are in charge of team dynamics.
The working relationship was said to be less equal in other hospitals than it is in the Lebrija HAR: “We come from hospitals that aren’t very large, and although their form of management is similar to this one, it will never be the same (SILENCE). Because it is not possible to be close to your middle manager. There is authority there, but not leadership. He isn’t your supervisor, he’s your authority.” PA 4
The majority of the respondents considered organizational climate to be a key factor, and it was said to be good in all cases. On the other hand, all of the respondents identified management training to be an essential element that is hardly taken into account in all of the competent areas. “It’s one of the aspects which is somewhat forgotten, and we all think that we don’t need to do it, but nurses’ work ranges very widely and this aspect is hardly constructed by the professionals themselves, as we think that it’s not our job to organize them. Or management training is delegated to middle managers, and those working in care are somewhat forgotten”. PA 3
All of the respondents with management positions had undergone a selection process for the same Official Bulletin of the Regional Government of Andalusia: “The process was published in the BOJA with the conditions that had to be met, what we had to fulfil and what we had to do. A project, and the project described what we wanted to do and all. The project was awarded a score and we also had to give our curriculum. Then there was a personal interview in which we had to defend the project, and with those scores we were able to gain the position” CI 2
All of the respondents considered that it is possible to rise in management: “In principle there are no problems at all. There may be a number of better or worse possibilities. A greater number of opportunities or a smaller number of opportunities, but I think that the company doesn’t create any hindrances, unlike what happens in the SAS, where the positions seem to be restricted to just a few people”. CI 3
In general management positions are thought to require a high level of personal involvement. The women in the focus group did not believe it was currently possible for them to accept management tasks because of their family commitments. “A higher ranking position would take a lot of time away from my family, so that’s what would restrict me now. That’s why my goal is to work and carry on learning, but always within the limits of what my family allows me to do”. PA 4
Gender-based differences emerged in terms of dedication to management tasks; given that the men believe that it is possible to work outside normal hours, the women said that lack of time due to family needs restricted their possibilities of working in a job that they found satisfying.
Management and informal leadershipThe nurses who performed care tasks consider that the contribution of their middle managers is indispensable for achieving goals and group cohesion: “Currently the bosses are working on achieving goals, so they’re working on that as fully as they can, on training as well as care; but we manage the resources we have correctly, and without us they wouldn’t achieve anything”. PA 3
In their discourse the respondents expressed their belief that leaders have special characteristics which they do not find in other professionals; this agrees with the findings of authors such as Tumbaco-Quimiz et al.,19 who consider that leadership in nursing is due to the human skills that are necessary for conflict resolution and the appropriate management of care. The characteristics expressed by the respondents in their discourse about the definition of a leader are similar to the concept of transformational leadership defined by other authors, who in their respective works consider transformational leaders to have characteristics such as charisma and a capacity for dialogue, among others.6,20
Regarding personal and professional costs, the majority of the women underlined how difficult it is to balance management work with family life. This underlines the fact that when nurses work on additional tasks, this is often due to a question of their vocation and/or professional responsibility, as Morandín-Ahuerma et al.21 show in their work. Therefore, and in agreement with the work by Fuentes-Plough & Ojeda-López,22 one aspect that nurses identified as worrying is the effect on their family, themselves and their circle if they take on a management position. The fact is that placing your family before personal or professional development has been one of the factors where traditionally the greatest inequalities between the sexes have arisen; this is a limiting factor for women, who find themselves in the position of simultaneously having to be good mothers and good professionals.23,24
Regarding promotion in work and gender, the Lebrija HAR differs from the dynamic within current public and private administrations, as in this hospital the highest management positions are occupied by women, and this is not the case in studies by other authors within healthcare.9
Lastly, the group of nurses working in care underlined the need for middle managers to display empathy. In this respect, several authors underline the importance of having charismatic leaders who are motivating and committed, where their leadership style functions as a lever that strengthens professional ties.11,20 The fact is that now the economy, care and health are all inextricably linked because the high incidence of chronic diseases is generating increased demand for nurses. This fact should produce a change in the current situation of the nursing profession, as the traditional hospital model is starting to show a lack of structural capacity to support the exterior demand it receives25,26; it is therefore necessary to take a step forwards and accept the importance that corresponds to this collective in the form of consolidated leadership. This is now more than ever a question of need as well as for the whole group to become aware of the real value of the results we achieve, as well as the capacity to demand recognition for the said outcomes.
The limitations of this study include the number of respondents, as this makes it impossible to establish an analogy with the results obtained in other Andalusian public hospitals. The fact that the interviewer is a healthcare worker and middle manager in Lebrija HAR may create a distortion between the same and the respondents.
To conclude, we underline that the predominant leadership style in the middle management of Lebrija Hospital is defined by nursing staff as participatory leadership. They underline the importance of the work by informal leaders of nursing within care teams. Although training in management may be considered to be important, there is no specific programme for this within the hospital training plans that cover care professionals. All of the middle management positions in Lebrija HAR have been allocated by public competition. Care professionals feel strongly involved in care tasks, teaching and management; they even work on questions in connection with the hospital outside their working hours. The work of intermediate nursing management is considered to be essential for the maintenance of effective control, and its contribution to the organization stands out. No gender-based bias was found in access to middle management positions, although the female nurses consider that it is harder for them to gain promotion due to the family obligations which they accept as their own.
OutlookThis study is an exploratory analysis of a subject of interest for public health, leadership in the Andalusian Public Health Service. Within this context, the ultimate aim of this study could connect with a subsequent analysis of the relationship between Nursing management and the efficiency and sustainability of the healthcare system.25
FinancingThis work was not financed.
We would like to thank the management, care coordination and Nursing care staff for their help in carrying out this study.
The following is Supplementary data to this article:
