




This study identified the association of the preexisting anxiety problem in women diagnosed with cervical cancer with their demographic characteristics.
MethodThis was a cross sectional study with 100 participants selected by purposive sampling method. Data were collected through Hamilton Anxiety Rating Scale (HARS) questionnaire and the medical records of participants.
ResultsWork status was the only demographic characteristic which was found to be statistically significantly related to the anxiety level of the participants before they were diagnosed with cervical cancer. Participants who worked at home as housewives were found to have higher anxiety level than those worked at the institutions or industry.
ConclusionsWorking women in this study were more likely to have the preexisting anxiety problem prior their cervical cancer diagnosis. This study implies the importance of promoting healthy lifestyle to manage daily stressors, considering various interrelated factors that may eventually contribute to cervical cancer development in women.
Psychological stress might contribute to the processes of illness, including cancer. The hypothesis of the psychological factor to influence the development of the cancer through the psycho neuroimmunological pathway has long been studied1–3. Evidences showed that psychological stress is able to interrupt the chemical messengers which connect the nerve, endocrine, and immune cells, and also to inhibit the anti-tumor immune responses of the body2,4. Furthermore, the interactions of emotion and immune functions might increase an individual's proneness to malignancy5.
The psycho neuroimmunological interactions work in both directions. They might heighten the cancer pathogenesis and, on the other hand, to predispose the psychopathological manifestations in patients having cancer1,2. This is the plausible explanation of why psychological issues are not uncommon among cancer patients.
Many studies addressed this phenomenon and developed various interventions to deal with the psychological stress in cancer patient's population, especially those with cervical cancer6–8. In the developing countries such as Indonesia, even though psychological problems of the cancer patients are mostly overlooked, previous studies in Indonesia examined this subject along with its intervention strategies9,10.
Nevertheless, evidence regarding the psychological stress that may precede cancer among Indonesian population is still limited. In fact, most of the cancer patients in Indonesia have lower socio-economic background, which may serve as an environmental stressor10,11. Women, in particular, are more vulnerable to psychological problems including anxiety and depression that were found to be linked with the women's reproductive milestone12. Therefore, it is of high importance to raise this issue among women having cancer in Indonesia. This study attempted to capture the association of the preexisting anxiety problem in women diagnosed with cervical cancer with their demographic characteristics.
MethodA cross-sectional study was conducted at one of the biggest general hospitals in Jakarta, the capital of Indonesia. We recruited 100 cervical cancer patients attending the outpatient unit of the study setting, using purposive sampling technique, in May-June 2016. The inclusion criteria were: being diagnosed with cervical cancer, having compos mentis mental status, being able to read and write in Bahasa Indonesia.
The demographic profile of the participants was collated through questionnaire set by the researchers. Moreover, we used Hamilton Anxiety Rating Scale (HARS) originally developed by Hamilton in 1959 to measure the preexisting anxiety problem among participants13. This tool contains 14 items of anxiety symptoms, in which each symptom item is rated on a five-point scale (0 = none, 1 = mild, 2 = moderate, 3 = severe, 4 = very severe). The total score of anxiety symptom spans from 0 to 56; higher score indicates heavier anxiety problem. The reliability test result of this tool, as piloted prior our data collection, yielded Cronbach's alpha of 0.953 which showed its reliability.
Data were analyzed with univariate and bivariate analysis. Except for age variable which was a numeric data, we calculated the proportion of other demographic variables, including educational level, occupation, marriage status, and income level. Chi-square test was carried out to identify the difference in the characteristics of the participants with the HARS score. P value of less than 0.05 was considered to have a statistical significance.
As we involved patients in our study, we were bound to the ethical conduct of the study with the human subjects. Apart from the ethical principles we applied in designing the study, we provided thorough explanation to all the approached patients before they stated and signed their consents to voluntarily join the study. We kept the privacy and confidentiality of the data of our participants until the completion of the study.
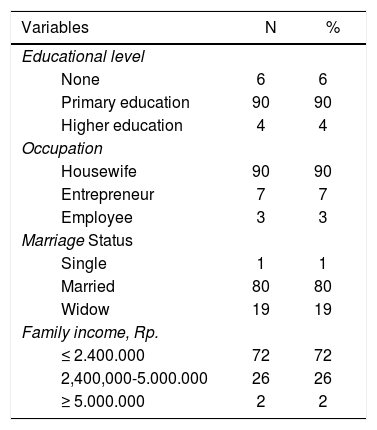
ResultsThe mean age of the participants was 51.89 years (SD= 8.596), ranging from 29-70 years old. Table 1 provides the summarized details of the demographic profile in this study. Most participants finished their basic education (90%). High school graduates slightly dominated the total sample of 100 cancer patients (41%), while the patients with elementary school background ranked second (30%). The majority of the participants worked as housewives (90%), were married (80%), with lower family income, roughly 185 US dollars per month, lower than the average minimum regional wage (72%).
Characteristics of the participants (n = 100).
| Variables | N | % |
|---|---|---|
| Educational level | ||
| None | 6 | 6 |
| Primary education | 90 | 90 |
| Higher education | 4 | 4 |
| Occupation | ||
| Housewife | 90 | 90 |
| Entrepreneur | 7 | 7 |
| Employee | 3 | 3 |
| Marriage Status | ||
| Single | 1 | 1 |
| Married | 80 | 80 |
| Widow | 19 | 19 |
| Family income, Rp. | ||
| ≤ 2.400.000 | 72 | 72 |
| 2,400,000-5.000.000 | 26 | 26 |
| ≥ 5.000.000 | 2 | 2 |
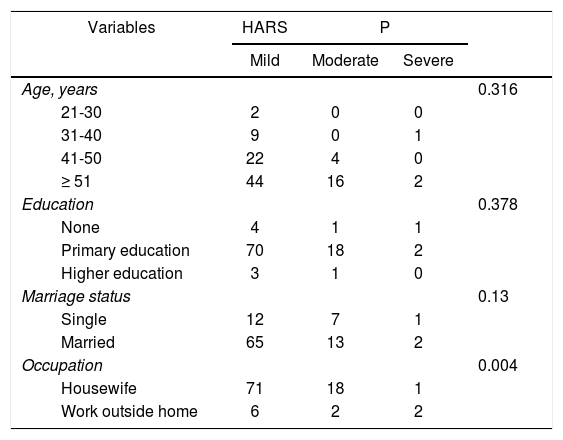
We analyzed the characteristics of the respondents against the HARS score with the following results (table 2). Table 2 shows that the participants aged more than 51 years old, had primary education background, and were married had higher anxiety level before they had cervical cancer diagnosis compared with the rest of the participants. However, no statistically significant relationships were found between these characteristics and the anxiety status prior the cervical cancer diagnosis. On the other side, participants who worked at home as housewives were found to have higher anxiety level than those worked at the institutions or industry. The occupation was also found to be statistically significantly related to the anxiety level of the participants before they were diagnosed with cervical cancer.
The relationship of the characteristics of the cancer patients with the Hamilton Anxiety Rating Scale (HARS) score (n = 100).
| Variables | HARS | P | ||
|---|---|---|---|---|
| Mild | Moderate | Severe | ||
| Age, years | 0.316 | |||
| 21-30 | 2 | 0 | 0 | |
| 31-40 | 9 | 0 | 1 | |
| 41-50 | 22 | 4 | 0 | |
| ≥ 51 | 44 | 16 | 2 | |
| Education | 0.378 | |||
| None | 4 | 1 | 1 | |
| Primary education | 70 | 18 | 2 | |
| Higher education | 3 | 1 | 0 | |
| Marriage status | 0.13 | |||
| Single | 12 | 7 | 1 | |
| Married | 65 | 13 | 2 | |
| Occupation | 0.004 | |||
| Housewife | 71 | 18 | 1 | |
| Work outside home | 6 | 2 | 2 | |
The demographic profile of the women with cervical cancer in this study is consistent with the profiling of the similar population in previous studies. That the participants were in their early fifty in average in this study was fairly in line with the characteristics of participants in a study in Indonesia14. This is close to the average age for menopause, which is 51 years old15. In terms of age-specific cervical cancer prevalence, the pattern of peak prevalence at ages 50-65 was found in many Asian and African Countries16. Few other studies found that the HPV prevalence pattern remains high across the age groups in low-resource countries17,18. The age-specific cervical cancer prevalence pattern, however, could not be concluded from these reports nor from prior studies in Indonesia. This present study, too, did not assess the link of age with cervical cancer occurrence.
Age was not found to be related with the preexisting anxiety problem among women with cervical cancer in this study. Nevertheless, more women aged 51 or older were found to have preexisting anxiety problem symptoms; two of them were considered to have severe anxiety. Psychological issues tend to markedly surge in women during the transition to menopause and decrease after menopause19. This is mainly due to complex interactions of reproductive hormones with the neural functioning, sociocultural, and biological factors12.
HARS tool used in this study indicates the symptoms of anxiety, but not a clinical diagnosis of it13. When the clinically-diagnosed anxiety disorder in women was studied, the results showed that the risk of cervical cancer was significantly lower among women diagnosed with anxiety disorder20. A contrasting result was found in previous metaanalysis which mentioned a significantly higher overall risk of cancer in population having psychological distress3. These rather intriguing findings might be resulted from various factors, particularly those pertinent to cervical cancer screening.
Most of the women in this study were housewives, had lower educational and socioeconomic background, and were married, similar to the results of the world health survey analysis21. Our finding did not reach statistically significant relationship of the educational background and marriage status with the past problem of anxiety among cancer patients, yet it had practical implication. With regards to characteristics in cervical cancer population, previous studies showed many associating variables. Case-control studies found that following variables were associated with CC: age, education, parity22 illiteracy, age at menarche, parity, poor genital hygiene, long duration of married life; social economic status, current smoking habit, years of contraceptive use and number of sexual partners23.
Unlike the other patient characteristics, work status was found to be associated with the preexisting anxiety problem among cervical cancer patients in this study. Interestingly, the majority of participants who were housewives and did not have formal work had higher anxiety level. The plausible explanation is that housewives tend to have limited social circle to share information and feelings with, or to gain support from. This is contradictory with previous studies which indicated working women have more probability to experience higher anxiety level24,25. Many women in developing countries have narrow access to health care services to perform early detection or treatment, due to their work responsibilities26. Meanwhile, further investigation done in a meta-analyses of 12 European cohort studies suggested that the work-related stress is unlikely to be a risk factor for cancer. It is important to note, however, that stressed women are more likely to have less healthy lifestyles, eat excessively and less healthily, which are evident risk factors for cancer.
Conflicts of interestDirectorate of Research and Community Service, Universitas Indonesia, for the financial support. Director of the Persahabatan Hospital and the staffs in the gynecology outpatient unit, for technical and other supports.
