




Family satisfaction has become an integral part of quality of care in hospitals. Thus, it is crucial to develop instruments that measure family satisfaction. The purpose of this study was to examine the validity and reliability of a family satisfaction questionnaire. Method: This study used a survey questionnaire consisting of 26 items that identified nurses' constructs of behaviors and communication. The population surveyed were families whose children were hospitalized due to pneumonia.
ResultsThe results revealed that only 16 items of the instrument demonstrated evidence of acceptable constructs of reliability and validity. The study recommends further studies that add other potential constructs related to family satisfaction.
Patient satisfaction is a critical indicator of the quality of health care. In order to stay competitive in the healthcare market, hospitals should maintain high levels of its customer satisfaction1 such as patients or families. Patient satisfaction will not only increase patient loyalty, but also enhance the hospital reputation. An enhanced reputation may lead to greater patient volumes and profits, as well as a decrease in the number of malpractice claims, and better efficiency1. In regard to pediatric patients, measuring children's satisfaction may require strenuous efforts. Children can neither make decisions concerning their own care nor determine the level of satisfaction with the care delivered. Thus, satisfaction can only be measured through the perception of family members and other surrogate decision makers.
Since nurses provide primary service to patients, family satisfaction with nursing care is an essential element of the quality of care delivered by the hospital. Nonetheless, nurses are challenged to use a valid and reliable instrument that considers family members as an important factor in determining the level of satisfaction. In addition, the instrument must take into account all attributes of satisfaction level, comprising: a) art of care; b) technical quality; c) accessibility; d) costs; e) physical environment; f) internal environment; h) healthcare providers and other sources, and i) sustainability of care and its impact1.
Wagner and Bear1 suggest 4 attributes of satisfaction associated with nursing care. These attributes include (1) non-intimidating gestures, (2) information regarding the patient's health status, (3) involvement of patients in decision-making, and (4) nurses' professional competencies. These attributes result in the condition of satisfaction or dissatisfaction. Satisfied patients and families are more likely to be compliant with the care provided by the hospital and will return for continuing care. On the contrary, dis-satisfied patients and families are more likely to be recalcitrant and stop their treatment, thereby reducing the hospital's revenue2.
Takemura et al3 recommended using a questionnaire to assess family satisfaction while receiving health education during discharge planning, or at the time of the patient's cognitive evaluation after discharge planning. Family satisfaction can also be measured after the family receives all information concerning specific treatments required for the child at home4.
MethodThis study examined the reliability and validity of the family satisfaction instrument. Family satisfaction was measured through a survey. The participants were parents whose children were hospitalized due to pneumonia. Data were collected at two district hospitals in the capital city of Indonesia.
The instrument was developed in accordance with professional nursing competencies in the form of behavior and communication constructs. It comprised 21 items focused on behavioral constructs and five items that addressed communication constructs. The reliability and validity of the instrument were assessed using Cronbach's alpha and the corrected item-total correlations (rit). An instrument with Cronbach's alpha coefficient of 0.8 or higher (scale total), and a rit higher than 0.3 we considered adequate.
ResultsA total of 30 subjects were surveyed. Five subjects were excluded due to incomplete data. The data cleaning produced the sample size of 25 for further analysis.
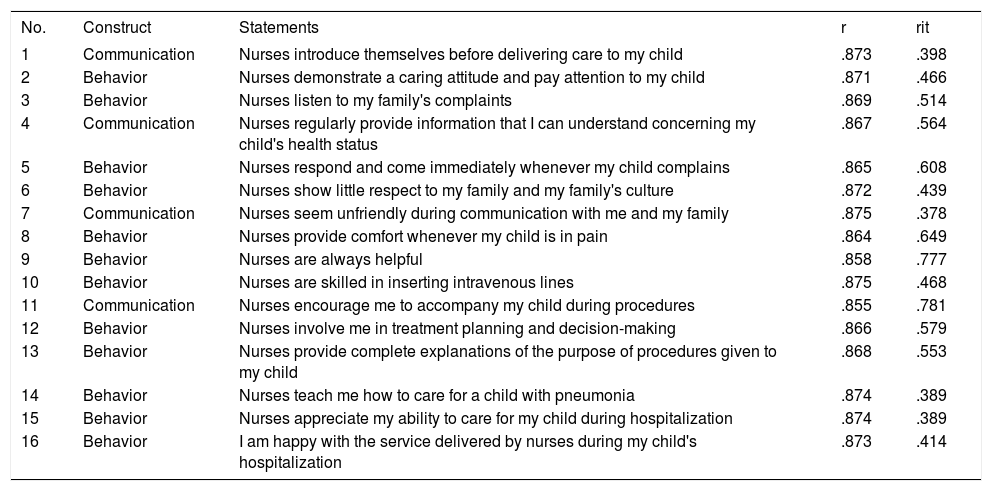
Of the 26 items in the instrument, 16 (items 1, 2, 3, 4, 5, 8, 9, 10, 11, 12, 15, 16, 18, 24, 25, and 26) had a reliability coefficient of higher than 0.8 and validity higher than 0.3. The invalid items comprised item numbers 6, 7, 13, 14, 17, 19, 20, 21, 22, and 23. Results for each item are shown in Table 1.
Validity and reliability analysis of family satisfaction questionnaire at 2 district hospitals, May-June 2014 (n = 25)
| No. | Construct | Statements | r | rit |
|---|---|---|---|---|
| 1 | Communication | Nurses introduce themselves before delivering care to my child | .873 | .398 |
| 2 | Behavior | Nurses demonstrate a caring attitude and pay attention to my child | .871 | .466 |
| 3 | Behavior | Nurses listen to my family's complaints | .869 | .514 |
| 4 | Communication | Nurses regularly provide information that I can understand concerning my child's health status | .867 | .564 |
| 5 | Behavior | Nurses respond and come immediately whenever my child complains | .865 | .608 |
| 6 | Behavior | Nurses show little respect to my family and my family's culture | .872 | .439 |
| 7 | Communication | Nurses seem unfriendly during communication with me and my family | .875 | .378 |
| 8 | Behavior | Nurses provide comfort whenever my child is in pain | .864 | .649 |
| 9 | Behavior | Nurses are always helpful | .858 | .777 |
| 10 | Behavior | Nurses are skilled in inserting intravenous lines | .875 | .468 |
| 11 | Communication | Nurses encourage me to accompany my child during procedures | .855 | .781 |
| 12 | Behavior | Nurses involve me in treatment planning and decision-making | .866 | .579 |
| 13 | Behavior | Nurses provide complete explanations of the purpose of procedures given to my child | .868 | .553 |
| 14 | Behavior | Nurses teach me how to care for a child with pneumonia | .874 | .389 |
| 15 | Behavior | Nurses appreciate my ability to care for my child during hospitalization | .874 | .389 |
| 16 | Behavior | I am happy with the service delivered by nurses during my child's hospitalization | .873 | .414 |
The survey items used to assess family satisfaction were developed based on literature studies and consensus among experts. The perceptions of family toward the quality of nursing care constituted the constructs of family satisfaction. As stated by Roberti and Fitzpatrick5, satisfaction with healthcare services can be measured by knowing family perception of the quality of care delivered. Furthermore, Yagil et al6 explained that the evaluation of nursing care, as part of quality of care, is predicted through evaluation of caring behavior, treatment, instruction, and the patient's environment. Therefore, these aspects also need attention from nurses to achieve better quality of care.
Hong et al7 stated that there were positive trends in increased parent satisfaction ratings of communication from nurses, instruction or explanation, and pain management, but none of these trends were statistically significant per t-test (P = 0.05). This condition may be caused by different interventions given to two intervention groups without a control group. Recommendations include staff education and an informational handout for parents as two interventions that could be conducted by nurses to increase parents' satisfaction.
Prominently, only half of the total items demonstrated evidence of acceptable constructs of reliability and validity. This probably resulted from the limited number of respondents involved. Nevertheless, this final item of the survey showed that the instrument is able to adequately measure essential components of family satisfaction with nurses' behaviors and communication.
Our study used four communication constructs for families. This result was consistent with a study conducted by Heyland et al8. Their study generated a valid and reliable instrument of family satisfaction, including the constructs of communication, along with decision-making, characteristics of healthcare workers, and family involvement. Furthermore, the items of communication comprised the provision of truthful, adequate, and consistent information concerning the patient's latest condition, treatment and procedures, and technology used to sustain the patient's life. The ability of healthcare workers to listen carefully also constituted an item of communication.
Along with the study by Heyland et al8, two other studies showed a close and interesting association between communication and family satisfaction. Henrich et al9 note that information about the patient's health condition, treatment process, and visiting hours encompassed all aspects of communication. Likewise, Berends10 found communication to be the most decisive factor in family satisfaction. He suggested that effective communication performed by nurses would increase family satisfaction. Valentine11 defined effective communication as the capacity of nurses to educate and provide necessary information for patients. Furthermore, Haines and Childs12 found that a high level of parental satisfaction can be affected by many aspects of the service provided, particularly the standard of care, the perceived competency of staff, and the level of support and involvement experienced. The respondents in that study provided suggestions to increase service development, including communication, necessary information, and preparation for the transition from pediatric intensive care to ward environments.
Conversely, Henrich et al9 stated that family complaints were higher for nurses who did not provide information concerning waiting time and the patient's latest condition. Family members often had to spend a great deal of time in the waiting room and remain vigilant to ensure that they received the latest information about the patient's condition. Accordingly, communication about patient information is of fundamental importance to patient satisfaction.
Beside the communication construct, our study derived 12 behavioral constructs. These items included caring attitude, responsiveness, family involvement, and respect. Our findings were consistent with the studies conducted by Mc-Donagh et al13 and Henrich et al9. Both studies showed that family satisfaction increased when nurses showed their genuine concern and respect for family members. Furthermore nurses were expected to be able to meet patient and family needs, involved the patient and family members in decision-making related to the patient's treatment, and provided comfort for the patient and family members. In addition, in the studies conducted by Latour et al4,14 the results of the confirmatory factor analysis showed that family participation, along with the caring and professional attitude of healthcare workers in pediatric intensive care units, were the major domains within family satisfaction.
