




The aim of this study was to investigate the correlation between levels of depression symptoms and age, thyroid-stimulating hormone levels, and stressful life events of the participants.
MethodPatients above 18 years old, with any thyroid disorders, and without psychiatric disorders were included in this study. All participants completed the Depression Anxiety Stress Scale 21 (DASS-21). The depression symptom score was calculated and interpreted as follows: less than 9: no depression; between 10 and 13: mild depression; between 14 and 20: moderate depression; between 21 and 27: severe depression, and more than 28: extremely severe depression.
ResultsThe total number of participants in this study was 199. There was no correlation between age, thyroid stimulating hormone, and the DASS score. There was also no significant difference in the DASS-21 score between genders. However, there was a positive correlation between depression symptoms and stressful life events (r=0.201, n=199, p < 0.05).
ConclusionsThese findings would suggest that increased depression symptom scores correlate with increased stressful life events. A larger study should be undertaken to confirm these findings.
Depression symptoms have been described in patients who had thyroid disorders. Studies of Asian countries, such as Nepal and Turkey, have found that about 24% of patients with thyroid disorders also suffer from depression symptoms1,2, but the association between these conditions is unclear3. In Malaysia, a country that situated in the Asian region with a population of 31 million had recorded approximately 1.1 million of thyroid disorder cases4. However, the association between the thyroid disorders and depression symptoms is not known due to the paucity of research in this area.
The association between thyroid-stimulating hormone (TSH) and depression symptoms is deba0 worldwide. Williams et al. reported that, in a study of 2,269 middle-aged men, a high level of TSH and a higher level of free thyroxine (fT4) was associated with a risk of developing depression symptoms5. Similarly, a significant association between high TSH and fT4 levels and depression symptoms, evaluated using the Hamilton Rating Scale for Depression (HDRS), was found in 19 of 80 patients newly diagnosed with thyroid disorders1. In contrast, a large-scale population study by Ittermann et al. showed that there is no significant association between TSH levels and depression on untreated thyroid disorders in patients in Germany, as analyzed using the Beck Depressive Inventory-II (BDI-II)6. These conclusions could be due to the variety of tools used to assess depression symptoms. Sample size and study design also may have affected the results.
Several studies in Europe have found that, certain levels of depression were reported among women with thyroid disorders, and all of these studies showed a significant association between the depression symptoms with TSH and fT4 levels7,8. Branka et al.9 revealed that most depression with thyroid disorders occurred in patients under 40 years of age. In addition, the TSH and fT4 levels significantly correlated with depression among thyroid disorders patients (p < 0.05) in Branka’s study.
Several reports also found that stressful life events experienced by the patient may precipitate lymphocytic infiltration of the skin, cytokine production, and altered immune regulatory functions10,11. These reports also found that stress could then initiate an inflammatory response and production of thyroid peroxidase-antibodies (TPO-Ab), which can decrease neurogenesis activity in the brain, resulting in reduced neuronal migration in the brain and the eventual appearance of depression symptoms10,11.
Despite positive correlations presented by many studies around the world between thyroid hormone levels and depression symptoms, no such correlations have been confirmed in Malaysia due to a lack of research. The aim of this study was to investigate the relationship between the level of depression symptoms with age, gender, TSH levels, and stressful life events of the participants as measured by the DASS-21 scale.
MethodThis was a cross-sectional study design. Two hundred adult patients who have been diagnosed with thyroid disorders were recruited from the Medical Outpatient Department (MOPD) and Surgical Outpatient Department (SOPD) in one of the non-profit hospitals in the Northern region of Peninsular Malaysia. The study duration was three months, from March 1, 2016 to May 31, 2016. Patients with dementia or psychotic disorders were excluded from this study due to cognitive impairment and the inability to participate in the self-report questionnaires used in this study. The sample size was determined by using the Kish formula12. In this study, the expected population of patients with thyroid disorders is based on a previous study of 294,328 patients by Nor Hayati et al.13. From our calculations, the minimum recommended sample size was 150 patients, including a 20% drop rate. Informed consent was obtained from all patients, and the study was approved by the International Islamic University of Malaysia Research Ethics Committee (IREC) and the Malaysian Medical Research Ethics Committee (MREC). The patients completed a questionnaire regarding demographic background, medical history, medications, and family history.
All participants completed the DASS-21 to assess levels of depression symptoms. This tool contains 14 statements in which the patients need to indicate how much the statements applied to him/her over the past week on a Likert scale from 0 to 3 (0=“does not apply to me at all”; 3=“applies to me very much”). Then the scores were summed up and interpreted as follows: 0-9 (normal); 10-13 (mild); 14-20 (moderate); 21-27 (severe), and 28 and above (extremely severe)14. This tool has been translated to the Malay version by Ramli and colleagues with excellent Cronbach’s alpha values of 0.94 and had good factor loadings of 0.4 and more15.
The List of Threatening Experiences (LTE) has 12-items consisting of common life events that tend to be stressful and have occurred over the past six months16. The LTE was used to identify stressful life events experienced by the patients. The tool uses a binary scoring that scores 1 for life events that have happened and scores 0 for life events that have not happened, which are added up. The more life events a patient has experienced, the higher the score, and the greater the impact on the patient16. This tool has been translated to the Malay version by Ng et al.17 and the parallel and test-retest reliability were satisfactory (Kappa=0.67-0.88). Blood samples for TSH levels were collected by a registered nurse and sent to the hospital’s laboratory for analysis. The TSH reference range was from 0.510 to 4.300 mU/L.
All data were presented in means and standard deviations if normally distributed, or in median and range if deviating from the normal distribution. The normality of the data was assessed by the Kolmogorov-Smornoff test. The Pearson correlation was used to identify the correlation between age, TSH levels, stressful life events, and depression symptom levels. Statistical significance was accepted at p < 0.05 for all data analysis procedures.
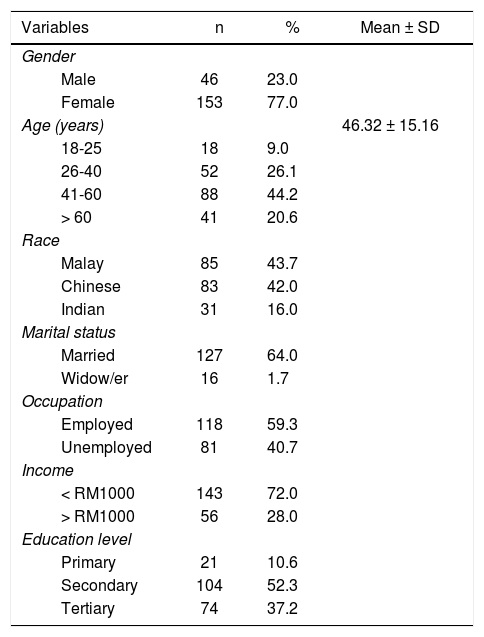
ResultsCharacteristics of the study sampleTable 1 shows the characteristics of the study sample. Participants in this study numbered 199. Of these participants, 46 (23%) were male and 153 (77%) were female. The minimum age was 18, and the maximum age was 83 years old. The mean was 46.32 ± 15.16 years old. The participants consisted of three main races in Malaysia: Eighty-five (43.7%) were Malay; eighty-three (42%) were Chinese; and thirtyone (16%) were Indian. Sixty-four percent (64%) were married (n=127); 56 (28%) were single; and 16 (1.7%) were widows/widowers. Most participants worked in the government and the private sector (59.3%). Most of the respondents (72%) had an income of more than RM1000 (USD 226), and fifty-six of the participants (28%) had income of less than RM 1000 (USD 226). Most of the respondents completed secondary school (52.3%).
The characteristics of study sample (n=199)*
| Variables | n | % | Mean ± SD |
|---|---|---|---|
| Gender | |||
| Male | 46 | 23.0 | |
| Female | 153 | 77.0 | |
| Age (years) | 46.32 ± 15.16 | ||
| 18-25 | 18 | 9.0 | |
| 26-40 | 52 | 26.1 | |
| 41-60 | 88 | 44.2 | |
| > 60 | 41 | 20.6 | |
| Race | |||
| Malay | 85 | 43.7 | |
| Chinese | 83 | 42.0 | |
| Indian | 31 | 16.0 | |
| Marital status | |||
| Married | 127 | 64.0 | |
| Widow/er | 16 | 1.7 | |
| Occupation | |||
| Employed | 118 | 59.3 | |
| Unemployed | 81 | 40.7 | |
| Income | |||
| < RM1000 | 143 | 72.0 | |
| > RM1000 | 56 | 28.0 | |
| Education level | |||
| Primary | 21 | 10.6 | |
| Secondary | 104 | 52.3 | |
| Tertiary | 74 | 37.2 | |
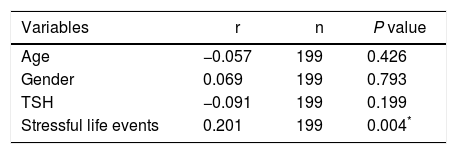
A Pearson product-moment correlation coefficient was computed to assess the relationship between age, gender, TSH, stressful life events, and depression symptoms levels. It is interesting to note that the only positive correlation was between stressful life events and depression symptoms levels, where r=0.201, n=199, and p=0.004. Age, gender, and TSH levels show negative correlations and are not statistically significant (Table 2).
Correlation between gender, age, TSH, and stressful life events and depression symptoms levels.
| Variables | r | n | P value |
|---|---|---|---|
| Age | −0.057 | 199 | 0.426 |
| Gender | 0.069 | 199 | 0.793 |
| TSH | −0.091 | 199 | 0.199 |
| Stressful life events | 0.201 | 199 | 0.004* |
In this study, the majority of the participants are in the middle-aged group (from 40 to 60 years old), most participants are female, and most participants are married and employed.
To identify the severity of depression symptoms, DASS-21 was used in this study. This tool has proven to have good reliability and validity and is widely used in psychiatry and other health care settings15. Moreover, the DASS-21 uses simple words and is convenient to administer in a large study population.
Through statistical analysis, this study found a negative correlation, with no statistical significance between TSH levels and depression symptoms. This finding is supported by Almeida et al. in a study on 3,932 men and the results showed that TSH concentration does not affect incidents of depression18. Another two studies report that there is no relationship between TSH levels and depression symptoms in patients with a variety of thyroid disorders19,20. Synthesis of findings of several previous studies shows that, there are consistent findings between this current study and other studies with regards to the negative correlation between TSH level and depression symptom. However, Panicker et al. have reported contrary findings. Panicker et al. found that, there is a significant interaction between TSH level and depression symptoms21. Therefore, it is assumed that, the reason for the inconsistency of findings between this current study and a study by Panicker et al.21 is probably due to the variety of sample characteristics involved in this current study as opposed to the Panicker et al study. Although both studies (this current study and Panicker et al.) involve thyroid patients as samples, insignificant findings are probably due to the small sample size and the single setting. Therefore, a larger study is needed to clarify the inconsistencies found in the literature.
Interestingly, this current study shows positive correlations and statistical significance between stressful life events and depression symptoms. This finding is similar to the Fukao et al.19, Kahaly et al.22, and Bock et al.23. Fukao et al., for instance, reported that the stress score of life events correlated significantly with the depression score, as evaluated by Natsume’s Stress Inventory tool, on 64 hyperthyroid patients19. Furthermore, in another study by Kahaly et al.22, a stressful life event has been found in 40.2% (n=102) of hyperthyroid patients before developing symptoms of depression. Congruently, a study by Bock et al23. reported that 62.8% (n=301) patients have a history of at least one moderate to severe stressful life event in a six month period prior to the onset of depression symptoms. However, most of the studies present above only provide descriptive findings on the stressful life events. Therefore, the relationship between the stressful life event and depressive symptoms remains unclear.
LimitationsSeveral limitations have been addressed in this study. First, the results could not be generalized because the study was conducted in a single setting only. Second, depression is a multi-factor disorder and should be controlled by several factors, such as family and social history, heredity, and morbidity. Moreover, the DASS-21 is a self-report tool, and the result may be more optimistic than reality. Last, due to the nature of the cross-sectional study design, the sample size is relatively small, and, consequently, the statistical power of the study decreases. Therefore, a larger sample is needed to confirm the study’s findings.
