





Stroke is a primary neurological disorder that exists in the world and causes both physical and mental disability. Based on WHO data, among 17 million new stroke cases, 7 million of them died from strokes. Indonesia's Sample Registration System (SRS) in 2014 showed that stroke was the main cause of death, which is 21.1% of all causes of death for all age groups. The purpose of this study is to obtain more comprehensive information regarding the development of mobile health application for primary prevention of stroke.
MethodsThe design used is Literature review. Articles were collected through Cochrane, Science Direct, Pubmed, Elseiver, Proquest (Links are from the library of unhas.ac.id) Pubmed, WHO, CDC, Google Scholar. The keywords used were stroke, primary prevention, risk factor, smartphone. After collecting the article then article synthesis was made.
ResultsBased on the reading results of the article, it shows that the incidence of stroke increased from year to year and became the main cause of disability and death. So it needs prevention from upstream sector, in this case primary prevention, through the development of mhealth applications using smartphones that can calculate the risk of strokes in 5 and 10 years. By using the application, it can provide information about the dangers of stroke, risk factors and how to overcome them.
ConclusionThe development of digital technology, application of stroke can effectively reduce the incidence of stroke.
Stroke is a primary neurological problem in the world. Stroke cases are growing from year to year. Obviously, a cause of death and incapacity throughout the world. Stroke has a boundless emotional and socio-economic impact on patients, families, and health services.1,2
Although primary prevention efforts have been made, stroke has remained a devastating disease in recent times. At the beginning of the 21st century, the incidence of age-standardized strokes in Europe ranges from 95 to 290/100,000 per year, with fatality rates for one month ranging from 13 to 35%. Around 1.1 million Europeans suffer strokes every year, and ischemic strokes cause around 80% of cases. Even though global strokes are declining, the level observed as a result of research suggests strategies for increasing prevention. In addition, due to an aging population, the total number of strokes is likely to rise dramatically in the coming years: by 2025, 1.5 million Europeans will suffer.3,4
Stroke prevention is a top significance for public health to reduce the growing global problem of stroke. According to Inter-stroke studies show that there are 10 risk factors that recorded 88.1% all originated from stroke. Many risk factors can be modified, therefore need avoidance strategies. Both the individual and community level.5–7
Stroke happens because it is caused by a risk factor which is known to be a risk factor for stroke i.e. there is something that can be controlled and cannot be controlled. Risk factors for stroke are more for the risk of lifestyle behavior.8,9 Risk factors for stroke involve hypertension, diabetes mellitus, hypercholesterolemia, carotid stenosis, and atrial fibrillation known as risk factors for stroke because clinical trials have shown that treatment of this condition reduces the frequency of stroke.9,10
Hypertension and diabetes mellitus are risk factors along with non-communicable diseases including stroke.7–10 INTERSTROKE (International Case–Control Study of the Risk Factors for Ischemic and Hemorrhagic Stroke) which evaluates the contribution of numerous risk factors to the burden of stroke worldwide, concluded that hypertension provides 34.6% PAF (Population Attributable Fractions) for stroke.9–11
Along with the times, entering the digital era 4.0, technological advances provide the latest revolutions for stroke prevention through applications on smartphones. Smartphone users in the world are growing day by day, statistical data states the number of smartphone or smartphone users around the world from 2014 to 2020 increased. In 2016, the number of smartphone users is estimated to reach 2.1 billion. While the number of cellphone users worldwide is expected to exceed five billion in 2019.
The successful application for stroke prevention, the stroke riskometer application, was unconventional based on data obtained from epidemiological studies. This application permits prediction of a stroke of 5–10 years.12,13
MethodLiterature search procedureLiterature search was collected through Cochrane, Science Direct, Pubmed, Elseiver, Proquest (Link from Unhas.ac.id Library) Pubmed, WHO, CDC, Google Scholar. The keywords used are stroke, primary prevention, risk factor, smartphone. Later collecting the articles, an article is synthesized. Articles used are from 2011 to 2019.
Based on the Preliminary Review, the incidence of stroke is swelling and is a most important reason of disability and henceforth to answer the problem Scientifically a literature review is carried out with the procedures performed in the preparation of this review literature, namely by
- 1.
Gather information from various sources:
- a.
Journal; Articles found were related to the theme, namely 2011–2019. Accessing international journals through Cochrane Central Science Direct, Pubmed, Elseiver, Proquest (Link from the Library of Unhas.ac.id) Pubmed, WHO, CDC, Google Scholar and National Journal used as reference in accordance with the theme, namely 2011–2019. Access the journal through (Google Scholar) by entering Keywords:
- 1.
Stroke: Articles that appear 72,516 selected 39 articles
- 2.
Stroke Risk Factor (hypertension, diabetes mellitus, cholesterol stress, smoking, physical activity, dietary habits): Articles that Appear 9780 selected 52 articles
- 3.
Stroke, Intervention Primary prevention, risk factor: Articles that appear 91 selected 48 articles
- 4.
Stroke, apps: Articles that appear 67 and are selected 22
- 5.
Stroke, culture: Articles that appear 606 and selected 14
- 1.
- b.
Report Online (Riskesdas) and access the Ministry of Health's web; References found 5 articles
- c.
Book; For theory there are some that are quoted from books, and books used from 1980 to 2008 with 15 books.
- a.
- 2.
Gather the material that has been obtained into Mendeley's software
- 3.
Making research synthesis from journals and other materials that have been obtained.
- 4.
Conduct a review of the material obtained to ensure that the Literature Review is carried out can improve information about the research variables.
The search results in the selective database gave a overall of 72,516 study articles written in English 2011–2019 about stroke, matching the keywords that required to be analyzed. Next, the articles are filtered by title, abstract, and keywords; the remaining 175 articles were then revised founded on their full text. A total of 47 articles were removed because (most of them did not discuss the riskometer stroke application and its implementation). Finally, a overall of 22 articles were selected in the review without other articles resulting from scanning the reference list. We can see Fig. 1, prisma flow diagram.
Study characteristics
This section defines demographic data items from the 22 particular articles. The results of this study indicate that 22 studies recognized the use of the Smart Phone Applications as aorigin of Information on prevention primer Stroke, especially to application is Stroke Riskometer Application.
Based on the reading results of the article, it shows that the incidence of stroke increased from year to year and became the main cause of disability and death. So it needs prevention from upstream sector, in this case primary prevention, through the development of mhealth applications using smartphones that can calculate the risk of strokes in 5 and 10 years. By using the application, it can provide information about the dangers of stroke, risk factors and how to overcome them.14
DiscussionStroke cases are increasing from year to year and become a major concern for the government. Stroke requires primary prevention namely risk factors for stroke.6 Stroke prevention consists of two focuses on individuals and society. For primary stroke prevention a recently developed application called the Stroke Riskometer15 has the potential to suggestively increase stroke and CVD prevention at the separate level. Based on the Framingham Heart Study stroke prediction algorithm16,17 and improved to include seven additional key risk factors that are very important for stroke (diet, physical activity, waist-to-hip ratio, alcohol, psycho-social stress, family history of heart attack, race/ethnicity), this accessible Stroke Riskometer is able to provide an estimate of the absolute risk of an individual stroke within the next 5 and 10 years for anyone from ages 20 to 90+ years.12,14
The Stroke Riskometer™ Lite version has been approved by the World Stroke Organization and the World Heart Federation. Both kinds of the application are accepted by the World Federation of Neurology, the International Association of Neurology and Epidemiology, and by the Russian National Association for Fighting Stroke. This application has spread in 70 countries so far, and this list is growing day by day. Given that around 1.75 billion people in the world have their own smartphone-based stage, this smartphone has high possible accessibility and gives people around the world personified data about stroke risk factors. The risk of stroke can be assessed for numerous family members, as well as elderly parents who sometimes do not use smartphones. To give as many people as possible application accessibility, the application has been interpreted into 20 languages. The Russian version of this application was edited by Prof. Varakin, Dr. Kravchenko, Prof. Piradov and Dr. Gnedovskaya from the Research Center of Neurology (Moscow).18,19
Recent advances in smartphone technology, including high processing power, storage, constant internet connection, modified notification methods, increased absorption across the globe, and closeness to users, offer unique opportunities to use this technology to improve health and improve research capabilities. An easily accessible and cost-effective risk valuation system is suitable for developing countries and other regions where access to medical facilities is limited, together with the elderly population where smartphones are increasingly being used. The latest systematic review shows that mobile-based technology in LMICs positively influences chronic disease management and clinical outcomes.17
The National Institute for Stroke and Applied Neurosciences at AUT University in association with AUT Enterprise Limited and the New Zealand Stroke Education (charity) Trust recently advanced the Stroke Riskometer™ App.2 The Stroke Riskometer application is an application to improve stroke prevention. In the application there are advanced features that users can easily use.12 For example, people can change the facts they put in the Stroke Riskometer to visually perceive the effects of changes in their risk of stroke. Stroke Riskometer can also be used to approximation the risk of recurrent stroke by people who have had a stroke or TIA and to calculate their risk of having a heart attack in the next 5 and 10 years. This can be used to monitor the development of strokes and prevent heart attacks. Application (version 1) is available free of charge.14,16
Stroke riskometer application conceptThe concepts in the Stroke Riskometer™ App namely; part 4 20:
- 1.
Translated into the 12 most used languages in the world. The application translation into Mandarin has been done in association with and under the direction of Prof. Wenzhi Wang (Beijing Neurosurgery Institute) and Prof. Hua Fu (Health Communication Institute, Fudan University). App calculates the risk of stroke 5 years and 10 years in individuals aged 20–90 years and over. This is a personalized assessment where individuals identify their own risk factors linked with stroke.17
- 2.
There are 19 risk factors involved in the application: age, sex, race/ethnicity, weight and height to calculate body mass index, smoking, alcohol and fruit/vegetable consumption, physical activity, stress, family history of stroke or heart attack, systolic blood pressure, blood pressure-lowering drugs, and the presence of diabetes mellitus, heart or peripheral arterial disease, a history of left ventricular hypertrophy, atrial fibrillation, dementia or cognitive problems, traumatic brain injury, and previous strokes or transient ischemic attacks.
Risk factors are incorporated into applications that calculate the risk of suffering a stroke using an algorithm advanced from the world-famous Framingham Heart Study using risk factors used by leading experts around the world.
- 3.
Answering all questions on the App only takes about 2min and does not involve any laboratory tests.
- 4.
The App provides estimates of not only complete but also relative risk of stroke; therefore, it allows users to compare their risk of having a stroke against someone of their age and gender without additional separate risk factors, thus representing a new paradigm in primary prevention of stroke.14,15,17,21
- 5.
In addition, because this application is available on iOS platforms (iPhone, iPad) and Android, this application has the potential to be used by around 700million Chinese smartphone users, together with rural people who may have limited access to health care facilities.15
The Stroke Riskometer App is anvery important tool in spreading awareness about stroke, its risk factors and how to overcome them, and, if used properly, can also signify a significant breakthrough as a method of conducting epidemiological research on NCDs internationally.17
Using applications, people can be motivated to control their risk factors and decrease their risk of stroke. Because many stroke risk factors also increase the risk of other health problems, this has additional potential to reduce the risk of heart attack, dementia, and diabetes mellitus.22,23 The Stroke Riskometer application has been validated10 against two usually used stroke prediction algorithms (Framingham and QStroke) and is endorsed by the World Stroke Organization, the World Neurology Federation, and the International Association on Neurology and Epidemiology. To be accessible to as many people as possible, the Stroke Riskometer application has been translated into 11 of the most commonly used languages (Mandarin, Hindi, Spanish, Russian, Arabic, Bengali, Portuguese, Malay, French, German, Japanese) covering more than 160 countries (5.6 billion people). The smartphone-based platform means that the potential reach of this application is huge. With around 1.75 billion people in the world who have smartphones, 11 people worldwide will have easy access to stroke risk and risk factors in their own language.15,17
Preliminary evidence shows that the application seems attractive to the individual concerned, because it empowers them to know and manage their own risks and risk factors. Regular and extensive custom of this application can be as efficient as conventional population-based approaches, because it allows identification and involvement in the prevention of all individuals which even slightly increases the risk of stroke and cardiovascular disease.15
Advantages and disadvantages of stroke riskometer applicationsEach application has advantages and disadvantages, the following are advantages and disadvantages of a stroke riskometer application (Table 1), some articles which research using the stroke riskometer application can be seen in the Synthesis Journal (Table 2).
Advantages and disadvantages of stroke riskometer app.
| Advantages | Disadvantages |
|---|---|
| User friendly | Scroll ruler to choose age, weight, height, etc. is not user friendly |
| Risk factors are separated into lifestyle factors that you can change such as diet, exercise, and risk factors that you cannot change such as age | A reasonable level of personal health knowledge is needed to enter risk factor information |
| Gives a stroke risk compared to someone without contributing risk factors | Unable to access education and videos in the free version. |
| Useful pictures to explain the signs and symptoms of a stroke | |
| User can click on the information icon that explains terms such as what is the presentation of fresh fruits and/or vegetables, the definition of regular exercise, etc. |
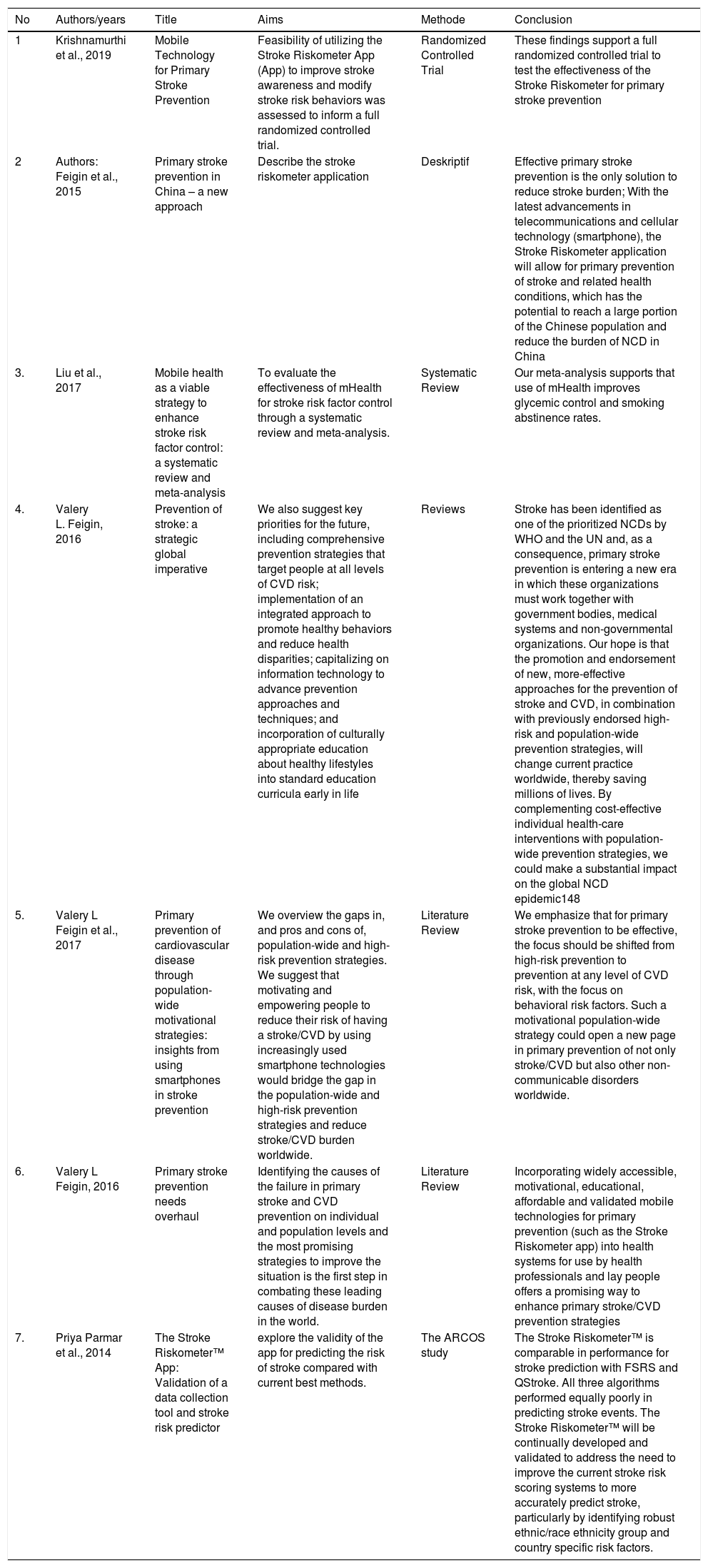
Synthesis of Journal of Stroke Prevention Interventions using stroke riskometer apps.
| No | Authors/years | Title | Aims | Methode | Conclusion |
|---|---|---|---|---|---|
| 1 | Krishnamurthi et al., 2019 | Mobile Technology for Primary Stroke Prevention | Feasibility of utilizing the Stroke Riskometer App (App) to improve stroke awareness and modify stroke risk behaviors was assessed to inform a full randomized controlled trial. | Randomized Controlled Trial | These findings support a full randomized controlled trial to test the effectiveness of the Stroke Riskometer for primary stroke prevention |
| 2 | Authors: Feigin et al., 2015 | Primary stroke prevention in China – a new approach | Describe the stroke riskometer application | Deskriptif | Effective primary stroke prevention is the only solution to reduce stroke burden; With the latest advancements in telecommunications and cellular technology (smartphone), the Stroke Riskometer application will allow for primary prevention of stroke and related health conditions, which has the potential to reach a large portion of the Chinese population and reduce the burden of NCD in China |
| 3. | Liu et al., 2017 | Mobile health as a viable strategy to enhance stroke risk factor control: a systematic review and meta-analysis | To evaluate the effectiveness of mHealth for stroke risk factor control through a systematic review and meta-analysis. | Systematic Review | Our meta-analysis supports that use of mHealth improves glycemic control and smoking abstinence rates. |
| 4. | Valery L. Feigin, 2016 | Prevention of stroke: a strategic global imperative | We also suggest key priorities for the future, including comprehensive prevention strategies that target people at all levels of CVD risk; implementation of an integrated approach to promote healthy behaviors and reduce health disparities; capitalizing on information technology to advance prevention approaches and techniques; and incorporation of culturally appropriate education about healthy lifestyles into standard education curricula early in life | Reviews | Stroke has been identified as one of the prioritized NCDs by WHO and the UN and, as a consequence, primary stroke prevention is entering a new era in which these organizations must work together with government bodies, medical systems and non-governmental organizations. Our hope is that the promotion and endorsement of new, more-effective approaches for the prevention of stroke and CVD, in combination with previously endorsed high-risk and population-wide prevention strategies, will change current practice worldwide, thereby saving millions of lives. By complementing cost-effective individual health-care interventions with population-wide prevention strategies, we could make a substantial impact on the global NCD epidemic148 |
| 5. | Valery L Feigin et al., 2017 | Primary prevention of cardiovascular disease through population-wide motivational strategies: insights from using smartphones in stroke prevention | We overview the gaps in, and pros and cons of, population-wide and high-risk prevention strategies. We suggest that motivating and empowering people to reduce their risk of having a stroke/CVD by using increasingly used smartphone technologies would bridge the gap in the population-wide and high-risk prevention strategies and reduce stroke/CVD burden worldwide. | Literature Review | We emphasize that for primary stroke prevention to be effective, the focus should be shifted from high-risk prevention to prevention at any level of CVD risk, with the focus on behavioral risk factors. Such a motivational population-wide strategy could open a new page in primary prevention of not only stroke/CVD but also other non-communicable disorders worldwide. |
| 6. | Valery L Feigin, 2016 | Primary stroke prevention needs overhaul | Identifying the causes of the failure in primary stroke and CVD prevention on individual and population levels and the most promising strategies to improve the situation is the first step in combating these leading causes of disease burden in the world. | Literature Review | Incorporating widely accessible, motivational, educational, affordable and validated mobile technologies for primary prevention (such as the Stroke Riskometer app) into health systems for use by health professionals and lay people offers a promising way to enhance primary stroke/CVD prevention strategies |
| 7. | Priya Parmar et al., 2014 | The Stroke Riskometer™ App: Validation of a data collection tool and stroke risk predictor | explore the validity of the app for predicting the risk of stroke compared with current best methods. | The ARCOS study | The Stroke Riskometer™ is comparable in performance for stroke prediction with FSRS and QStroke. All three algorithms performed equally poorly in predicting stroke events. The Stroke Riskometer™ will be continually developed and validated to address the need to improve the current stroke risk scoring systems to more accurately predict stroke, particularly by identifying robust ethnic/race ethnicity group and country specific risk factors. |
The stroke riskometer application is an intervention medium, with overall positive feedback. The stroke riskometer application can prevent strokes because this application has a section to educate people about the symptoms and warning signs of a stroke and what to do if there are symptoms/signs of this. This section uses faces, arms, speech, time messages, strategies that have proven effective in reducing time for hospitalization. In addition, users have the choice to email their stroke risk assessment results to people of they choose, and they also have the choice to share their experiences using the application through social media. Preliminary evidence shows that this application is interesting to the individual concerned because it permits them to know and manage their own risks and risk factors.24–27 The use of this application on a regular and extensive basis can be as efficient as a conventional population-based approach because it allows identification and involvement in prevention of all individuals who even have a slightly improved risk of stroke and CVD. We also encourage health professionals to use the application in their daily practice.14,17 The development of the digital technology, the application about stroke using can effectively reduce the incidence of stroke.
Conflict of interestThe authors declare no conflict of interest.
The work was supported by Faculty of Public Health, Hasanuddin University.
Peer-review under responsibility of the scientific committee of the 3rd International Conference on Healthcare and Allied Sciences (2019). Full-text and the content of it is under responsibility of authors of the article.
