




Pain management is one of the methods used in the health sector. Nursing care focuses on non-pharmacological measures, including the provision of aromatherapy using lavender and rose aromatherapy, which aims to understand the effectiveness of lavender and rose aromatherapy on pain intensity of postoperative patients in Laparatomi Hospital in Aisyiyah General Hospital in the surgical inpatient room, Padang in 2019.
MethodThe design of this study is a Quasi Experiment with pre-test and post-test designs with two groups. The sample of this study was Post Laparatomi in RSU with the technique of Accidental Sampling. The sample of this study consisted of 30 people for lavender and rose aromatherapy. Statistical tests used the Independent Test T-test.
ResultBased on the results of the study it was found that lavender and rose aromatherapy can reduce pain scale in postoperative patients. But compared to the two intervention groups, the aroma group of lavender therapy is more effective with mean pain scale before lavender aromatherapy being 5.20 and pre-test is 3.40 with p-value 0.000.
ConclusionThe nurses could provide nursing care in dealing with pain management in postoperative patients in addition to deep breathing techniques. It is recommended to apply aroma lavender therapy, which reduces pain and makes patients more relaxed.
Surgery is the treatment measure that use invasive methods by opening or displaying the parts of the body to handle. It is estimated that more than 400 million people worldwide suffer various etiological injuries.1 Pain is one of the most common problems associated with postoperative injuries but is often ignored by health care providers.
Patients regard pain as the worst part of a surgical wound that contributes to a decrease in their quality of life.2 Empirical evidence and clinical experience show that pain associated with injury is often exacerbated and causes increased chronic stress.3 However, despite what appears to be comparable dangerous stimuli, there are significant individual differences in reporting, behavioral responses, and emotional distress caused by pain.4
Increasing attention has shown how individual's expectation of pain can alter and amplify the experience of pain even when the stimuli are innocuous.5 Further understanding of how anticipation, anxiety, and pain are linked is crucial for developing therapeutic interventions to break the vicious cycle of pain, anticipation, and worsening of pain.
Pain is a subjective experience of multidimensional nature. The ‘pain matrix’ has been coined to theorize the highly intricate network that involves the interplay of various neurophysiological and psychosocial attributes in modulating the perception of pain and individual's responses to interventions.6 Analgesic medications remain the mainstay for management of pain. Various medications produce pain relief by interacting with different receptors in the peripheral and central nervous systems; the selection of appropriate analgesic agents based on the severity and the types of pain (nociceptive versus neuropathic). Over the last few decades, there has been a growing interest in the role of emotion and cognition in pain perception. Neuroimaging studies had identified several cortical and subcortical structures that are activated by the expectation of pain and associated emotional responses.7
Nurses play an important role in managing pain and anxiety in patients.8 As nurses spend more time with patients, they can assess their pain and anxiety, and can use non-pharmacological techniques, if needed.9 Due to a lack of effective symptom management by current methods, attention is paid more to the use of complementary and alternative therapies as non-pharmacological methods for reducing patients’ anxiety.10 Pain management using non-pharmacological methods consists of a wide range of simple, non-invasive, low-cost techniques without side effects. In recent years, the effect of complementary therapies including music, massage, and relaxation have been studied, but due to controversy results, more clinical trials on their effects are needed.11
Aromatherapy refers to the use of essential oils or aromas extracted from aromatic plants for therapeutic purposes. It is used to relieve pain, anxiety, depression, insomnia, fatigue, asthma, and increase self-confidence and creativity.12 The aroma can be applied in various forms, such as skin massage and inhalation, directly and indirectly. In a study of postoperative patients, inhalation of rose scent treatments has shown to reduce pain in postoperative patients. The aroma of roses contains steric compounds, ketones, aldehydes, and terpenes, which reduce pain and anxiety through stimulation of the olfactory center in the brain.13
Many commonly found plant oils are frequently utilized as anxiolytics. These include lavender (Lavandula angustifolia), rose (Rosa damascena), bergamot (Citrus aurantium, subs bergamia), and sandalwood (Santalum album). Aromatherapy refers to the use of drugs or therapies for essential oils absorbed through the skin or olfactory system. Although many claims have made regarding the benefits of aromatherapy, most studies have focused on its use to manage depression, anxiety, muscle tension, sleep disturbances, nausea, and pain. The purpose of this study was to determine the effectiveness of aroma rose therapy with lavender aromatherapy on the reduction in pain scale of postoperative patients.
Materials and methodsThis research is a type of quantitative research with a design used “Quasi Experiments”. Two treatment groups performed namely the Rose Aromatherapy relaxation technique and the aromatherapy lavender therapy group. The experimental group consisted of pretest and post-test after treatment. The intervention was carried out for three consecutive days and once a day for 20min, and each session lasted from 45 to 30min by administering five drops of aromatherapy mixed with 50ccs of water in the humidifier. Sampling was done by accidental sampling of 30 respondents. Data collection observed directly. The dependent variable in this study is the pain scale, and the independent variables are rose and lavender aromatherapy. Data analysis was carried out by Univariate by looking at each variable and bivariate using parametric tests, namely, paired T-test.
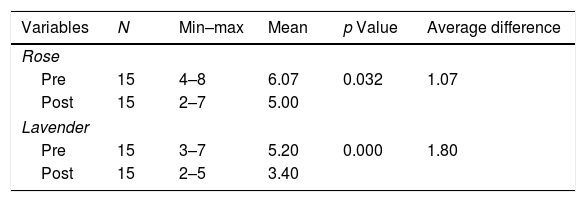
Result and discussionTable 1 shows the average post-Laparatomi pain scale before being given aromatherapy rose is 6.07, and after being given aromatherapy, rose is 5.00 with a p-value of 0.032. The average postoperative pain scale before lavender aromatherapy is 5.20, and after lavender aromatherapy is 3.40 with a p-value of 0.000. The average difference before and after the administration of rose aromatherapy is 1.07, while the average difference before and after the administration of lavender aromatherapy is 1.80.
Based on the results of the study it was found that the aromatherapy of rose and lavender essential oil can reduce the pain scale of postoperative patients. There are differences in the rose aroma therapy p value 0.00 while there is also a difference in lavender aromatherapy more effective p value 0.00 which can reduce the pain scale in postoperative patients.
In the past, pain was assessed as a symptom and as a means for recognizing diseases. Nowadays, it is considered as a separate nursing diagnosis, which requires special attention and treatment in nursing practice and education. American Pain Society (APS) described the importance of pain and defined it as the fifth vital sign. The decade between 2001–2010 was named as the “pain control” decade.14 The importance of pain control is typically considered less because of ignorance of physiological effects, burden of disease, and socio-professional reflections.
Pain is caused by stimulating the sympathetic nervous system that increases blood pressure, heart rate, and respiratory rate; restlessness; insomnia; nutritional problems; and delay in recovery. Pain can be relieved by pharmacological and non-pharmacological methods including complementary therapies. Many drugs are used for relieving pain. But they have limitations and side effects such as lidocaine spray, which can cause allergic reactions, systemic absorption, and potential cardiac dysrhythmia. In contrast, the non-pharmacological methods are low-risk, feasible, and accessible and present a cost-benefit to the field of nursing as well. Complementary therapies include many methods such as distraction, body relaxation, music therapy, and aromatherapy.15
Recent meta-analyses and systematic reviews support the notion that aromatherapy may exert clinical symptom relief when compared with placebo or standard treatment. For example, in a meta-analysis examining different types of pain management, aromatherapy was superior to placebo in treating postoperative, obstetrical, and gynecological pain.16 A systematic review investigating the effects of aromatherapy on dysmenorrhea showed that alleviating the effect of menstrual pain was larger with aromatherapeutic interventions than with placebo interventions.17 In a meta-analysis of randomized controlled trials on stress reduction, aroma inhalation yielded favorable effects compared with no treatment, but this effect mainly showed in subjective self-reports.18
Aromatherapy via massage, inhalation therapies, baths with herbal essential oil and mineral substances is used extensively. Aromatherapy is one of the potential methods of reducing perioperative pain. Aromatherapy uses essential oils to affect a patient's mood and health. In addition to music, relaxation, guided imagery, and massage, aromatherapy has been used by nurses as part of a holistic approach to minimize preoperative anxiety.19
There are additional reasons that may either benefit or harm the evaluation of aromatherapeutic interventions. One critical factor regarding aromatherapy is the lack of accuracy. Working with essential oils is not enough to make a clinical claim in the medical context. In contrast, working with volatile compounds of essential oils by inhalation is also not supported by medical evidences.20
Inhalational aromatherapy may decrease pain, mental stress, and depression, and improve vital signs. The aromatherapy effect starts by absorbing aroma molecules through the nasal mucosa. Then aroma molecules convert to nervous signals in the olfactory bulb, amygdala, and the limbic system and produce therapeutic effects by causing the release of a variety of neurotransmitters such as encephalin, endorphins, and serotonin. According to the results of the current study, in three days, inhaling the aroma of roses alone reduces pain. The smell can stimulate and release neurotransmitters and endorphins in the brain, which creates pleasant feelings. Aroma using rose essence reduces sympathetic reactions, stabilizes vital signs in burn patients and then reduces their anxiety.21
A research22 showed the effect of rose aromatherapy on reducing pain scale in postoperative patients. Based on the results of this study the mean postoperative pain scale before being given rose aromatherapy is 5.87 and after 3.78 with a p-value of 0.000. Thus, rose aromatherapy can reduce the pain scale of postoperative patients.
Lavender used in aromatherapy with anti-bacterial, anti-fungal, anti-bloating, muscle relaxant and analgesic effects. However, aromatherapy with Lavender has pain relief effects but this effect still has not been confirmed completely. Lavender essential oil is used widely in aromatherapy for its antispasmodic, sedative, and anesthetic effects. Linalyl acetate and Linalool of Lavender essence stimulate the parasympathetic system by reducing heart rate, respiratory rate, and blood pressure and consequently acts as a narcotic and sedative. Some studies have shown the effect of aromatherapy with lavender on pain relief, while other studies show that aromatherapy with lavender does not have a pain-relieving effect.
A research23 showed that average score of sleeping among elderly before lavender therapeutic scent application was 15.23 and after application of lavender therapeutic scent was 5.54. Statistical testing result found p=0.000 where it showed that there was an effect of lavender therapeutic scent toward improvement of elderly sleep quality.
Palliative and sedation effects of linalool, which is one of the main compositions in lavender, on the central nervous system, might be one of the causes that make results significant, which leads to a reduction in autonomic response to painful stimuli. Besides, the memory associated with sweet smell can enable a person to review the details of his emotions and events. The sweet smell of lavender can cause a lack of focus on pain and decrease the perception of pain severity. Nurses can use inhalation aromatherapy with lavender essence to reduce pain such as in case of post-surgery and other procedures. Inhaled aromatherapy with lavender essence oil is a cheap, safe, and efficient complementary treatment method is easy to use for nurses and has no interference with medical care.
In conclusion it was seen that rose aromatherapy can reduce pain intensity in postoperative patients. It is hoped that this study can help the nurses in pain management as an intervention in dealing with pain complaints in case of postoperative patients.
Conflict of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Conference on Healthcare and Allied Sciences (2019). Full-text and the content of it is under responsibility of authors of the article.
