





4th International Conference for Global Health (ICGH) in conjunction with the 7th Asian International Conference in Humanized Health Care (AIC-HHC)
Más datosFamilies experience various kinds of problems and problems in caring for family members whose families experience various obstacles in treating a patient with mental disorders. One condition that is felt is anxiety. Anxiety is related to ignorance regarding the patient's condition; earn a living; demands to divide time. The role of the family becomes very important because the patient lives in the middle of the family. Families need knowledge in managing patients both when treated at the hospital and when returning home. The purpose of this study was to determine the effect of family psychoeducation (FPE) therapy on family anxiety in treating a patient with mental disorders. The design used a quasi-experiment with the pre-test and post-test with control group methods. The sample was 100 respondents (50 experimental groups and 50 control groups). The results of the study showed a significant effect of FPE on family anxiety with a p-value of 0.00 (p<0.05). It was concluded that FPE therapy effectively reduced family anxiety in treating a patient with mental disorders.
Mental health is a condition of subjective well-being, trusting in one's abilities, autonomy, competence, feelings of interdependence, and self-actualization of one's intellectual strength and emotional state. Prosperous conditions include the ability to handle life's problems, be able to work productively, and provide support to the community.1 According to the Mental Health Act No. 18 of 2014, people with mental disorders (ODGJ) are a term for people who are disturbed in their way of thinking, disturbed in their behavior and feelings as indicated by some significant behavioral changes, and cause suffering and obstacles in carrying out their role as a human. Someone who has offspring with schizophrenia will feel the inner conflict within him. This is a consideration for someone to get therapy.2 Previous research that has been done has proven that psychoeducation therapy can improve general symptoms and reduce family rejection and burden.3 Research on FPE on the family burden and ability shows evidence that with a p-value of 0.00, FPE reduces the burden and increases the ability of the family. According to research regarding FPE on the ability of families to care for patients with social isolation, it showed an increase in cognitive abilities of 30 and psychomotor abilities of 27.08.4 According to another study, FPE on family abilities shows that FPE effectively improves family cognitive abilities by 15.64 and increases psychomotor abilities by 9.44.5 Herminsih research on FPE on family anxiety and burden proved that with a p-value of 0.00, FPE reduced anxiety and family burden.6
MethodDesign, population, and study settingsThe research design was a Quasi Experiment Pre-Post Test With Control Group by providing Family Psychoeducation (FPE) therapy to the intervention group. The study was conducted in 2018 in Semarang. Respondents are families who own and provide care for family members who have mental disorders. There is a population of 100 respondents, were selected through a sampling technique included in this study. Respondents were in general characteristics such as age, education level, and occupation. Respondents were divided into the intervention group (50 patients) and the control group (50 patients).
VariablesThe anxiety level of the respondents was measured using a Lovibind and Crawford Depression, Anxiety, Stress Scale questionnaire that had been developed by Nugroho and Rochmawati.7 The questionnaire consisted of 42 questions, which included statements for depression, anxiety, stress. Researchers used the FPE module to provide interventions, which contains the procedure of implementing therapy, starting from session 1 to session 5.
Data collectionData collection is a process of approaching the subject and the process of gathering the characteristics of the subjects needed in a study. Data collection was carried out by researchers visiting health service places as research sites, taking care of licensing for research purposes. Select subjects for respondents, inform the purpose and purpose of data collection, and explain how to fill in giving a questionnaire. Researchers collect and check completeness after respondents fill out the questionnaire. Request the questionnaire sheet that has been filled out by the respondent in accordance with the specified time. After a time agreement was reached with respondents, the researchers gave FPE therapy from session 1 to session 5. Therapy was given in 2 meetings for each session. The final stage of this study is to re-measure the level of family anxiety using a questionnaire and compile reports on research results. In collecting this data, the researcher was assisted by several enumerators who had a role in distributing questionnaires and re-collection. Enumerators come from students and mental health cadres in the local area.
Data analysisAnalysis of research data was using the Homogeneity Marginal Test. Marginal Homogeneity was chosen because it suits the needs of the data to be processed or analyzed.8,9 There are more than 2 choices of data, namely anxiety consisting of 4 choices, no worries, mild anxiety, moderate anxiety, and severe anxiety. Frantically entered the category of severe anxiety.
Ethical aspectsAll respondents were given an explanation of the objectives and research process and their rights as respondents. Respondents signed informed consent as a sign of agreement becoming part of the research process. Names and personal information about respondents are stored securely and confidentially.
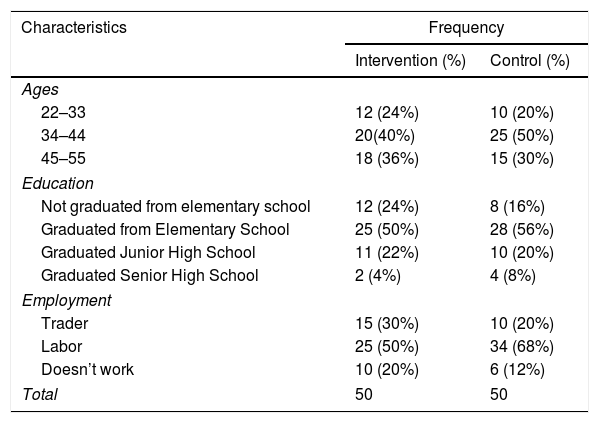
ResultsCharacteristics (Table 1).
Frequency distribution of respondent characteristics (N=100).
| Characteristics | Frequency | |
|---|---|---|
| Intervention (%) | Control (%) | |
| Ages | ||
| 22–33 | 12 (24%) | 10 (20%) |
| 34–44 | 20(40%) | 25 (50%) |
| 45–55 | 18 (36%) | 15 (30%) |
| Education | ||
| Not graduated from elementary school | 12 (24%) | 8 (16%) |
| Graduated from Elementary School | 25 (50%) | 28 (56%) |
| Graduated Junior High School | 11 (22%) | 10 (20%) |
| Graduated Senior High School | 2 (4%) | 4 (8%) |
| Employment | ||
| Trader | 15 (30%) | 10 (20%) |
| Labor | 25 (50%) | 34 (68%) |
| Doesn’t work | 10 (20%) | 6 (12%) |
| Total | 50 | 50 |
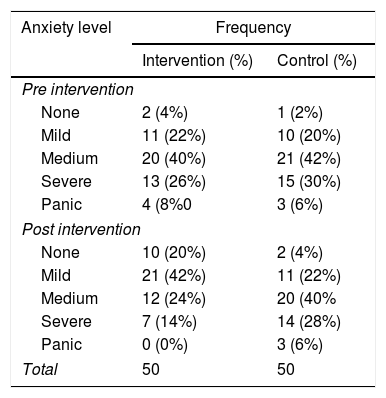
The level of family anxiety (Table 2).
Frequency distribution of family anxiety levels (N=100).
| Anxiety level | Frequency | |
|---|---|---|
| Intervention (%) | Control (%) | |
| Pre intervention | ||
| None | 2 (4%) | 1 (2%) |
| Mild | 11 (22%) | 10 (20%) |
| Medium | 20 (40%) | 21 (42%) |
| Severe | 13 (26%) | 15 (30%) |
| Panic | 4 (8%0 | 3 (6%) |
| Post intervention | ||
| None | 10 (20%) | 2 (4%) |
| Mild | 21 (42%) | 11 (22%) |
| Medium | 12 (24%) | 20 (40% |
| Severe | 7 (14%) | 14 (28%) |
| Panic | 0 (0%) | 3 (6%) |
| Total | 50 | 50 |
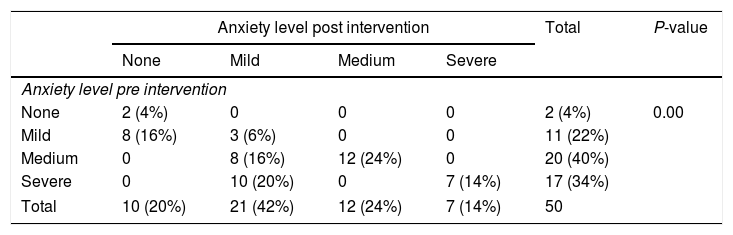
Effect of family psychoeducation therapy.
Results of marginal homogeneity tests on anxiety level before and after the psychoeducation in the intervention group (n=50).
| Anxiety level post intervention | Total | P-value | ||||
|---|---|---|---|---|---|---|
| None | Mild | Medium | Severe | |||
| Anxiety level pre intervention | ||||||
| None | 2 (4%) | 0 | 0 | 0 | 2 (4%) | 0.00 |
| Mild | 8 (16%) | 3 (6%) | 0 | 0 | 11 (22%) | |
| Medium | 0 | 8 (16%) | 12 (24%) | 0 | 20 (40%) | |
| Severe | 0 | 10 (20%) | 0 | 7 (14%) | 17 (34%) | |
| Total | 10 (20%) | 21 (42%) | 12 (24%) | 7 (14%) | 50 | |
Table 3 shows the results that of the 50 respondents were mostly at the medium anxiety level of 20 people (40%), and after the intervention, the majority were at the level of mild anxiety at 21 people (42%). Based on statistical calculations, a significant p-value of 0.00 (p<0.05) can be concluded that the alternative hypothesis (Ha) is accepted, and the null hypothesis (Ho) is rejected, meaning that there is a significant difference between pre-intervention family anxiety and post-intervention family anxiety.
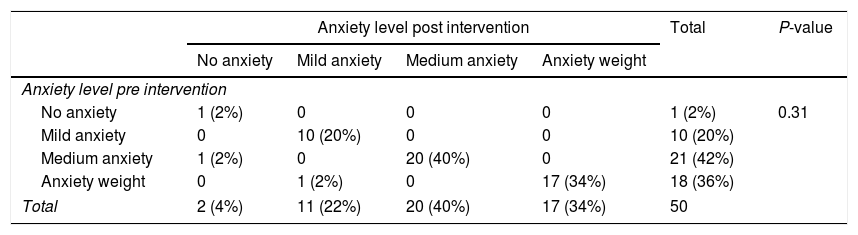
Table 4 shows the results of the measurement in the control group of 50 respondents. In the first measurement, the control group was mostly in the medium anxiety level of 21 people (42%), and after the intervention, the majority were in the medium anxiety level of 20 people (40%). Based on statistical calculations in the control group, p-value=0.317 (p>0.05) is concluded that the alternative hypothesis (Ha) is rejected, and the null hypothesis (Ho) is accepted, meaning that there is no significant difference between pre-test and post-test anxiety.
Homogeneity Marginal Test Results on the Anxiety Level Before and After the Psychoeducation in the Control Group (n = 50).
| Anxiety level post intervention | Total | P-value | ||||
|---|---|---|---|---|---|---|
| No anxiety | Mild anxiety | Medium anxiety | Anxiety weight | |||
| Anxiety level pre intervention | ||||||
| No anxiety | 1 (2%) | 0 | 0 | 0 | 1 (2%) | 0.31 |
| Mild anxiety | 0 | 10 (20%) | 0 | 0 | 10 (20%) | |
| Medium anxiety | 1 (2%) | 0 | 20 (40%) | 0 | 21 (42%) | |
| Anxiety weight | 0 | 1 (2%) | 0 | 17 (34%) | 18 (36%) | |
| Total | 2 (4%) | 11 (22%) | 20 (40%) | 17 (34%) | 50 | |
Most respondents experienced medium anxiety, as many as 20 respondents (40%). The anxiety that is felt is caused by the worried about the fate and future of their child. Also worried about the continuity of family life, respondents had to care for patients, while other children also needed care and attention. Anxiety needs to be direction or support so that it can prevent the occurrence of maladaptive conditions, which can cause responses that are not good for health.10,11
Based on statistical calculations in the intervention group, a significant p-value of 0.00 (p<0.05) was obtained, and it was concluded that the effect of therapy was given on family anxiety. Family psychoeducation therapy is an educational and pragmatic approach. Designed primarily to increase family knowledge about the illness, teach techniques that can help families to identify symptoms of behavioral disorders, and increase support for family members themselves. Family psychoeducation therapy is done to reduce the intensity of emotions in the family to a low level.
Psychoeducation was carried out in 5 sessions; session 1 identified the problems experienced by the family and changes that occurred in the family related to the patient's condition; session 2 taught how to treat patient with mental disorders (causes of mental disorders, recognition of signs and symptoms, how to seek treatment); session 3 taught stress management and recurrence (overcoming recurrence of patient with mental disorders, family stress management); session 4 teaches family burden management (obstacles in treating patient with mental disorders); session 5 optimizes community empowerment in helping families.12,13 The five sessions were conducted in the intervention group in 2 meetings for each session.
After the implementation, respondents who did not experience anxiety from 2 people (4%) became 10 people (20%). Respondents who experienced mild anxiety from 11 people (22%) became 21 people (42%). Respondents with moderate anxiety as many as 20 people (40%) dropped to 12 people. Furthermore, respondents who experienced severe anxiety and panic from the number of 17 people (34%) down to 7 people.
Family psychoeducation therapy is given by teaching the family to identify the problems experienced when providing care to patients and the personal problems of the respondent when caring for, problems that are felt both stress and burdens that arise.14 After the problem is identified, education is carried out on treating patients according to the patient's problems. Also taught about stress management and family burdens so that there are no difficulties or obstacles in caring for patients. Families are also assisted in using available resources and utilizing existing health care facilities around their neighborhood to help keep patients stable and not relapse.
Statistical calculations in the control group obtained a significant p-value of 0.31 (p>0.05) and concluded that no effect of therapy was given on family anxiety. Then to fulfill the principle of fairness, the control group was given therapy, but the results of implementing the therapy were not reported in the study. There was a change in family anxiety level, but it was not significant in the control group.
In the first measurement, respondents who did not experience anxiety 1 person (2%) became 2 people (4%) in the second measurement, 8 people previously experienced moderate anxiety. Respondents who experienced mild anxiety from 10 people (20%) became 11 people (22%). Respondents with medium anxiety from 21 people (42%) decrease to 20 people. Moreover, respondents who experienced severe anxiety and panic from 18 people (36%) dropped to 17 people. The increase and decrease in the level of anxiety of the control group respondents did not have significant value because they were not influenced by the research activities being carried out. The level of anxiety that is different at the two measurements made is due to factors that affect anxiety itself.
ConclusionSome things that can be concluded from this study are the majority of respondents aged 34–44 years in the intervention group (40%) and the control group (50%). Most respondents’ education was elementary school graduation, 50% in the intervention group, and 56% in the control group. Most respondents’ occupations were laborers, 50% in the intervention group, and 68% in the control group. In the pre-test measurement, the most anxiety level of respondents was in the medium anxiety, 40% in the intervention group, and 42% in the control group. Whereas in the post-test measurement, the most anxiety level of respondents in the intervention group were 42% mild anxiety, and 20% were medium anxiety control group. There is an effect of family psychoeducation therapy on family anxiety in the intervention group with a p-value of 0.00 (< 0.05).
Conflict of interestThe authors declare no conflict of interest.
Researchers would like to thank Prof. Dr. Ocky Karna Radjasa-DIKTI, Rector Unissula, LPPM Unissula, Dean-FIK Unissula, and all parties involved in the study.
Peer-review under responsibility of the scientific committee of the 4th International Conference for Global Health (ICGH) in conjunction with the 7th Asian International Conference in Humanized Health Care (AIC-HHC). Full-text and the content of it is under responsibility of authors of the article.
