






Introduction
Plasmacytomas has been reported to be present in a wide variety of organs, but medullary plasmacytomas are the most frequent, followed by other locations in the reticuloendothelial system. Plasmacytomas are not common in the gastrointestinal tract and those located in pancreas are extremely rare.1 We report a case of a woman with known multiple myeloma who presented jaundice and cholangitis due to a pancreas-located plasmacytoma. Patient was not candidate for stem cell transplantation, but immediate relief of obstructive jaundice was achieved with radiotherapy. No recurrence of biliary tract obstruction was noted at a 12-month follow-up.
Case presentation
A 69-years-old female with known multiple myeloma (MM) presented to emergency room with fever, abdominal pain and jaundice. Cholangitis was diagnosed. Laboratory findings were: serum bilirubin of 5 mg/dL, serum alkaline phosphatase of 159 mg/dL, alanine aminotransferase of 41 UI/dL and aspartate aminotransferase of 38 UI/dL. She suffered a plasma-cytoma in the right radius and lumbar spine 5 years ago; she was not candidate for stem cell transplantation, therefore she was treated with radiotherapy and melphalan plus prednisone, achieving complete clinical and biochemical response. Three years later, recurrence of MM was observed and a new scheme of chemotherapy (vincristine, doxorubicin and dexamethasone) was initiated. In current hospitalization, endoscopic biliary canulation was not possible because of total obstruction of choledochal duct. Computed tomography (CT) revealed a 12 x 7 x 8 centimeter lobulated tumor that involves pancreas, superior mesenteric vein and duodenum, with dilation of the biliary tract (Figure 1). A CT-guided biopsy was performed and histological examination showed characteristic findings of plasmacytoma (Figures 2 and 3). At this moment, elevation of gamma globulin in serum protein electrophoresis was noted. Broad-spectrum antibiotics (ceftriaxone plus metronidazole) were given with resolution of cholangitis. Later, radiotherapy (18 Gy divided in 3 sessions) targeted to upper abdomen was also given achieving relief of jaundice and 50% size reduction of the plasmacytoma (Figure 4). At 12 months of follow-up serum levels of bilirubin and alkaline phosphatase are normal and she had no further episodes of cholangitis.
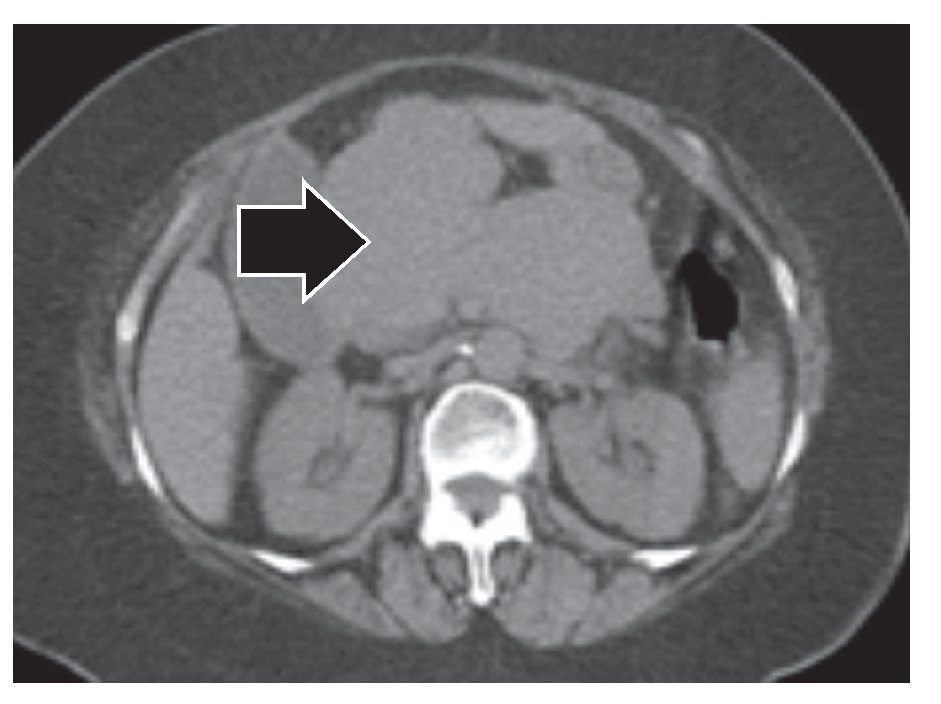
Figure 1. Initial CT image. The CT image shows a diffuse pancreas enlargement of (13 x 7 x 8 cm) (arrow) that causes an external compression of stomach and duodenum.
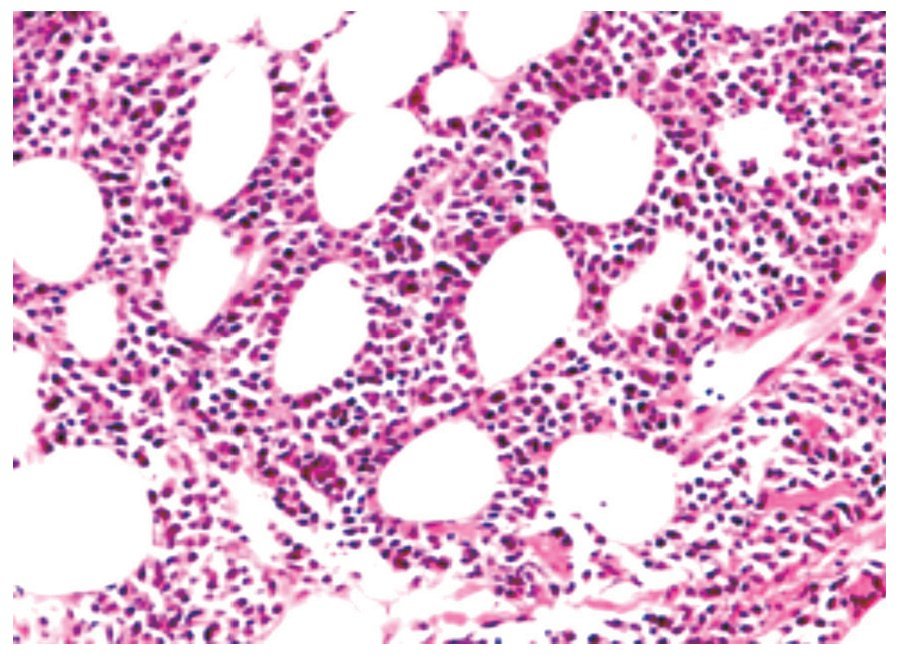
Figure 2.Tissue obtained by CT-guided biopsy. Pleomorphic, bi-nucleated, and mitotic plasmacytoid cells (40X, H&E stain).
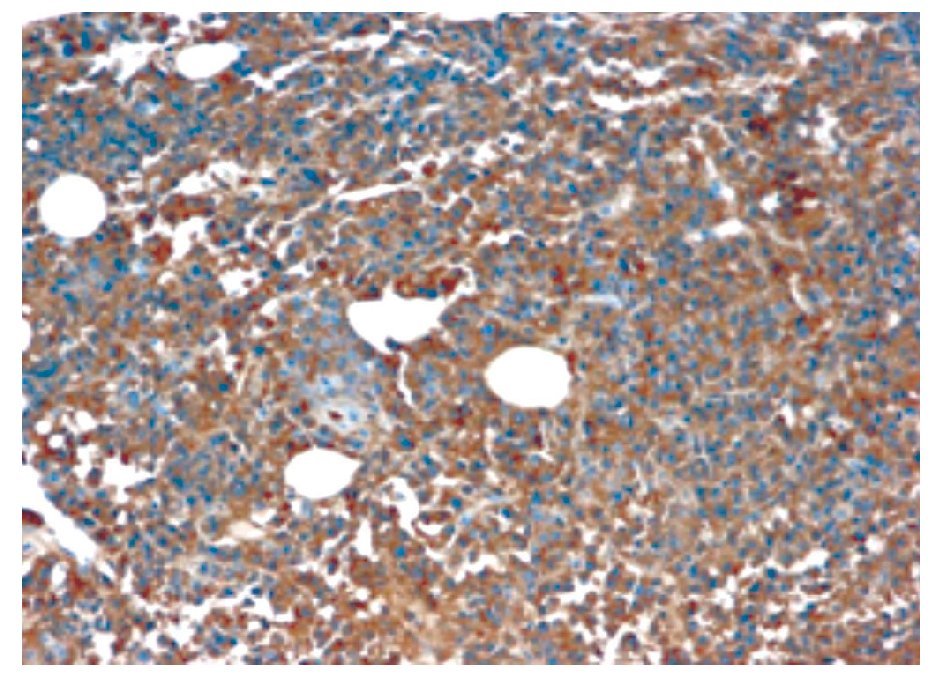
Figure 3. Immuhistochemistry of tissue obtained by CT-guided biopsy. The CD138 immunoreactivity highlights plasmocytoid cells (40X).
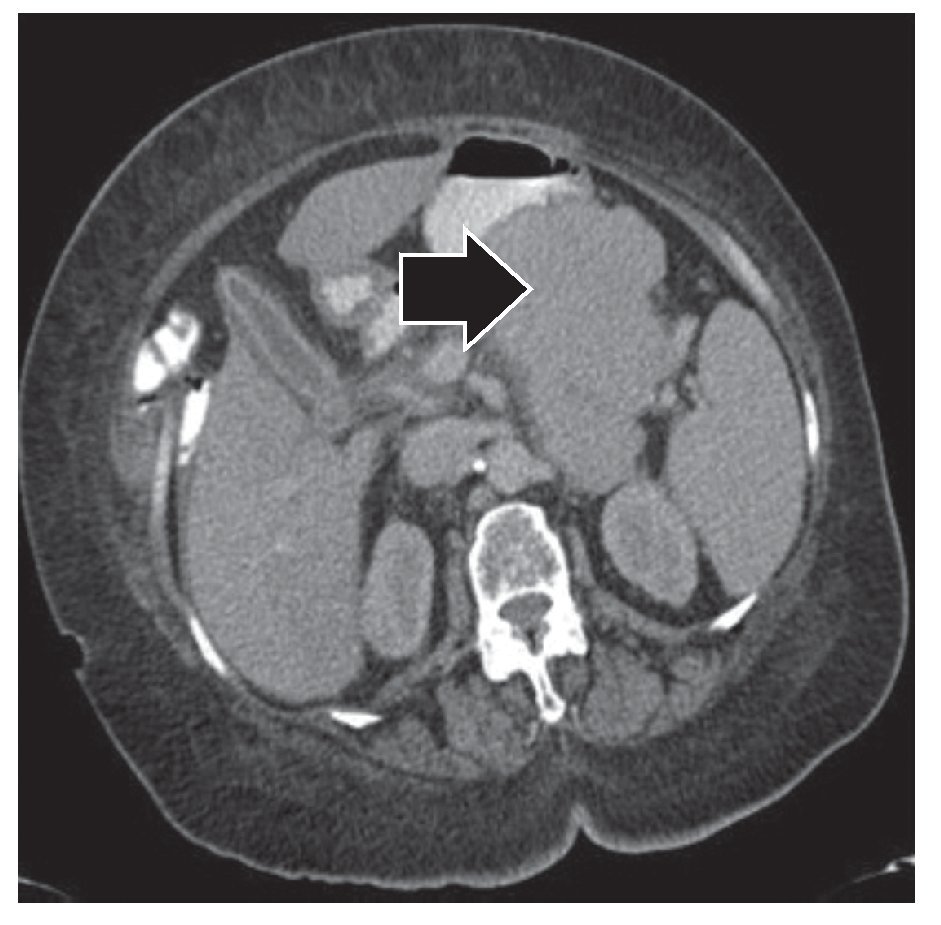
Figure 4. Post-radiotherapy CT image. A 50% size-reduction of pancreatic mass is noted (arrow).
Discussion
We present an unusual case of a 69-years-old female with MM and a plasmacytoma in pancreas that caused obstructive jaundice and cholangitis. In cases of MM and a pancreatic mass differential diagnosis includes primary pancreatic neoplasm, amyloid infiltration and plasmacytoma.1,2 Clinical presentation of pancreatic plasmacytomas may occur as result of direct plasmatic cell invasion or adjacent structures compression. Reticuloendothelial system is the most frequent localization of extramedullary plasmacytomas.3 However, plasma cell infiltration of pancreas may be found in about 2% of all autopsies of patients with known MM.4-7 One of the largest series of MM in the gastrointestinal tract reported a prevalence of 0.9%, in which the liver was the most affected organ. In the group of patients with pancreatic disease (n = 8), 3 (37.5%) patients presented cholangitis, and 2 (25%) were diagnosed incidentally, suggesting that pancreatic infiltration is more common than it is known and may be asymptomatic in some cases.8 Treatment of biliary obstruction secondary to plasmocytoma is not well defined but endoscopic stent placement followed by chemoradiotherapy has been successful for size reduction of the pancreatic mass in small number of patients.3,9 In our patient, as in other cases, radiotherapy resulted in tumor size reduction and resolution of cholangitis.10-12 Surgical options, such as choledochojejunal diversion, have been reported,13 but current patient was not candidate for it. Despite cholangitis is potentially fatal, antibiotic therapy followed by radiotherapy was successful. This case supports opinions about that radiotherapy could be an option for biliary obstruction secondary to pancreatic plasmocytomas.14
Correspondence: Dr. Josué Barahona Garrido.
10 calle 2-45 zona 14,
Oficina 204. Guatemala City 01014, Guatemala.
Phone: (502) 23854913, 23854915, 23854916 Fax: (502) 23854913.
Email: gastromedic@gmail.com