


To examine the sociodemographic factors associated with subclinical vitamin A deficiency in a representative sample of Colombian children.
Subjects and methodsA cross-sectional, descriptive study was conducted of data from the 2010 National Nutrition Survey of Colombia (ENSIN 2010) on 4279 children aged 12–59 months. Plasma vitamin A levels were measured using high resolution liquid chromatography (HRLC), and sociodemographic factors (sex, age, ethnicity, SISBEN score, and geographic region) were collected using a structured survey. Prevalence rates and associations were established using a multivariate regression model.
ResultsVitamin A levels ranged from 7.5 to 93.7μg/dL (mean=26.2; 95% CI, 25.9–26.5μg/dL). Vitamin A levels less than 20μg/dL (subclinical deficiency) were found in 24.3% of children. Children belonging to ethnic groups of African ascent, those living in the Orinoquia and Amazonia regions, and those aged 12–23 months had the greatest subclinical vitamin A deficiencies (29.5%, 31.1%, and 27.6%, respectively). Regression models showed that age ranging from 12 to 23 months (OR 1.32; 95% CI, 1.01–1.73), a SISBEN score 1 (OR 1.66; 95% CI, 1.18–2.34), an African ascent (OR 1.35; 95% CI, 1.05–1.74), and living in the Orinoquia and Amazonia regions (OR 2.38; 95% CI, 1.62–3.51) were factors associated to subclinical vitamin A deficiency.
ConclusionsThe study population shows a high prevalence of subclinical vitamin A deficiency, and comprehensive interventions involving nutritional and educational components are therefore recommended.
Examinar los factores sociodemográficos asociados a la deficiencia subclínica de vitamina A en una muestra representativa de niños colombianos.
Materiales y métodosEstudio descriptivo transversal, secundario de la información obtenida en la Encuesta Nacional de la Situación Nutricional 2010 (ENSIN 2010) en 4.394 niños entre 12-59 meses. Los niveles plasmáticos de vitamina A se determinaron por cromatografía líquida de alta resolución (HPLC), y los factores sociodemográficos (sexo, edad, grupo étnico, puntaje de SISBEN, región y área geográfica) se recogieron por encuesta estructurada. Se establecieron prevalencias y relaciones mediante la construcción de modelos de regresión y factores asociados.
ResultadosSe encontró un rango de niveles de vitamina A de 7,5-93,7μg/dL (media=26,2μg/dL; IC95% 25,9-26,5μg/dL). El 24,3% de los evaluados presentaron niveles de vitamina A inferiores a 20μg/dL (deficiencia subclínica). Los niños pertenecientes a la etnia afrodescendiente, los residentes en la zona de Orinoquia y Amazonia, y grupo etario de 12-23 meses de edad, presentaron las mayores deficiencias subclínicas de vitamina A (29,5, 31,1 y 27,6%) respectivamente. Los modelos de regresión muestran que estar entre 12-23 meses de edad (OR 1,32; IC95% 1,01-1,73), pertenecer al SISBEN nivel 1 (OR 1,66; IC95% 1,18-2,34), residir en la zona de Orinoquia y Amazonia (OR 2.38; IC95% 1,62-3,51) y pertenecer al grupo étnico afrodescendiente (OR 1,35; IC95% 1,05-1,74) se asociaron como factores de presentar deficiencia subclínica de vitamina A.
ConclusionesLa población estudiada presenta una alta prevalencia de deficiencia subclínica de vitamina A, por lo que se recomienda intervenciones integrales donde estén involucrados el componente nutricional y educativo.
Subclinical vitamin A deficiency is among the main nutritional problems in many developing countries, mainly because of its inadequate consumption in diet.1 The Micronutrient Initiative (MI)2 and the United Nations Children's Fund (UNICEF) estimated that vitamin A deficiency was endemic in 39 countries worldwide based on retinol levels <10μg/dL. In 1995, an update of the report of the World Health Organization (WHO) showed that this public health problem was significant in 60 countries.3 In 2005, approximately 122 countries had subclinical vitamin A deficiency, with values <20μg/dL, mainly in preschool age children.4 According to the WHO, subclinical vitamin A deficiency increases mortality risk by up to 19% in children with diarrheal disease.5 In addition, it accounts for 6% and 8% of deaths in children younger than 5 years in Africa and Asia respectively.6 In America, the combination of low weight, micronutrient deficiencies (iron, vitamin A, and zinc), and suboptimal breastfeeding in children causes 7% of deaths and 10% of the total morbidity burden.7
In Colombia, subclinical vitamin A deficiency in children under 5 years of age has decreased in the past 5 years. According to data from the National Health Institute (INS) and the National Nutrition Survey in Colombia (ENSIN-2010),8 serum retinol levels <20μg/dL were 24.1, 14.2, and 5.9% for the 1977–1980 period, 1995 and 2005 respectively.
The WHO3–5 and other authors6,9 have postulated that much controversy exists about the definition of reference values or factors associated with vitamin A deficiency in children, especially in Latin American countries like Colombia. The main causes of subclinical vitamin A deficiency may be summarized into 2 categories: inadequate diet, including lower consumption of foods containing vitamin A, and presence of infectious conditions due to decrease in the retinol-binding protein.10
Because of the foregoing, there was a need to ascertain serum vitamin A levels in young children. Moreover, because of age dependency of vitamin A and the scarce information available for Latin American children, there was a need to characterize the factors associated to plasma retinol levels in this age group. The purpose of this study was therefore to examine the factors associated to subclinical vitamin A deficiency in Colombian children aged 12–59 months.
Subjects and methodsStudy design and populationA cross-sectional study using secondary data from the National Nutrition Survey (ENSIN), which was funded by the Colombian Institute for Family Well-being (ICBF) and conducted during the 2008–2010 period.10 A total of 5952 children of both sexes (aged 12–59 months) were eligible.
SampleThe study comprised the Colombian population aged 0–64 years, and indicators are given disaggregated by age group, sex, ethnicity, and socioeconomic level. This survey is a cross-sectional measurement conducted to ascertain the prevalence of nutritional problems and some health conditions in the Colombian population. The study universe consisted of 99% of the population living in private homes from urban and rural areas, in 50,670 homes, distributed into 258 towns or primary sampling units (PSUs) from the 32 departments of the country and Bogotá, DC. Segments were proportional in the municipalities and in the rural area, and were concentrated into 1920 clusters.10
Type of sampleProbabilistic, stratified multistage cluster sampling was used for ENSIN-2010.
Sample sizeSample size was decided based on the requirement of greater accuracy in estimating overall malnutrition at department level, taking as a basis the estimation of this indicator in the prior ENSIN-2005, calculated with the new WHO growth patterns. For this, the simple random sampling formula was used to design clusters for each group of interest as follows:
where N=size of the population group or subgroup for which estimation of a proportion or disaggregation level is desired.
P=minimum proportion expected.
Q=1−P.
deff=effect of sample clustering, defined as estimation of the variance of cluster design and variance of design of a simple random sampling.
rel=relative standard error desired.
Sample selectionIn the population aged less than 59 months, vitamin A markers were tested using a subsample of 5000 segments. To estimate prevalence, the traditional formula of estimation of proportions, adjusted to sample design (strata, stages, and primary sampling units) was used. The coefficient of variation (standard error/estimation×100) was also calculated to assess precision of estimations, considering precision levels of estimations as follows: CVs under 20% indicated high precision, those ranging from 20 to 30% intermediate precision, and CVs over 30%, very low precision. With these calculations, sample representativeness in this age group reaches a disaggregation level for the six Colombian regions. The response rate in the age group defined for this study was 73.8% (n=4394).
ProceduresThe study was approved by the ethics committee of the National Nutrition Survey. For vitamin A measurement, a sample of 5–8mL of blood was drawn after disinfecting the venipuncture area. Samples were centrifuged at between 2500 and 5000rpm for 10min and were subsequently separated in amber vials. They were kept refrigerated at the Nutrition Laboratory of the Colombian INS until tested. Vitamin A levels were measured using high performance liquid chromatography (HPLC). During processing, plasma was diluted to a half with a solution of retinol acetate in ethanol, a solvent that precipitates proteins and releases retinol. Retinol was then extracted with hexane, which was evaporated with gaseous nitrogen and resuspended in methanol. Finally, retinol levels were determined at a wavelength of λ=325nm in a Waters 600® chromatograph with autosampler relating the peak retinol area to the acetate area. Vitamin A blood tests and cut-off points were based on WHO references, and “subclinical vitamin A deficiency” was defined as values ranging from 10 to 20μg/dL.
Sociodemographic factorsThe following sociodemographic variables were defined as associated factors for this analysis: (1) age; (2) area or origin (urban or rural); (3) identification of the ethnic group of home members, who were asked if they recognized themselves in given groups: (a) Indian, (b) African descendants, and (c) other. Although the survey makes it clear that this categorization was not intended to reach a national representativeness of ethnic groups, data were important to have a significant number of African descendants and Indians. Because of this, ethnic classifications in this study were restricted to three ethnic groups: Indians, African descendants, and “other”, the latter group including people who did not identify with any of the two other groups; (4) geographic region; (a) Atlantic, (b) Western, (c) central, (d) Pacific, (e) Bogotá, and (f) Orinoquia and Amazonia. Social or socioeconomic status was determined based on the Identification System of Potential Recipients of Social Programs, SISBEN (1–3, and 4 or more); this is an index developed by the National Planning Department of Colombia which takes into account sociodemographic characteristics, living conditions, and access to home public services.
Statistical analysisAn exploratory analysis was first performed to determine frequency distribution (measures of central tendency and dispersion for quantitative variables) and relative frequencies (for qualitative variables). To estimate the relationship between vitamin A deficiency and sociodemographic variables in children (age, sex, geographic region and area, ethnic group, and socioeconomic level-SISBEN), four binary logistic regression models were used. The first binary logistic regression model was simple (unadjusted OR); the second model was adjusted for age group and sex; the third model was adjusted for ethnic group, region, geographic area, and SISBEN score; and the third group was adjusted for age, sex, ethnic group, region, geographic area and SISBEN score. A factor was considered a confounder if, after addition to the model, the odds ratios displaced in a constant direction and exposure level of proportional change was at least higher than 10%. All analyses were adjusted by sample weights, and sample design and population expansion factors were considered in sample design. Analyses were performed using SPSS version 20, and a value of p<0.05 was considered statistically significant.
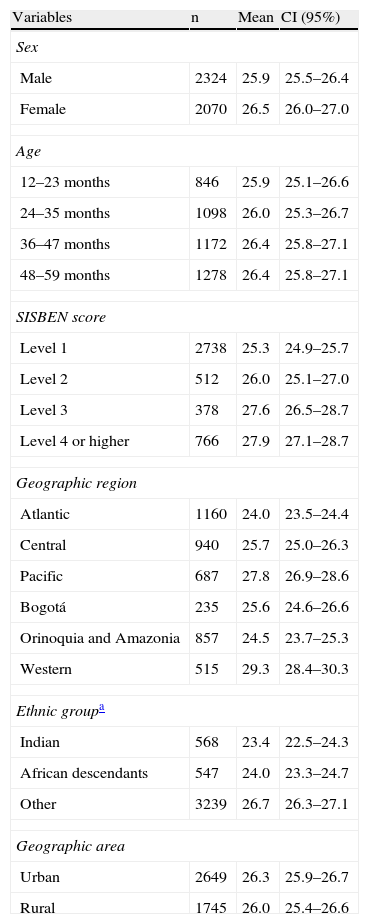
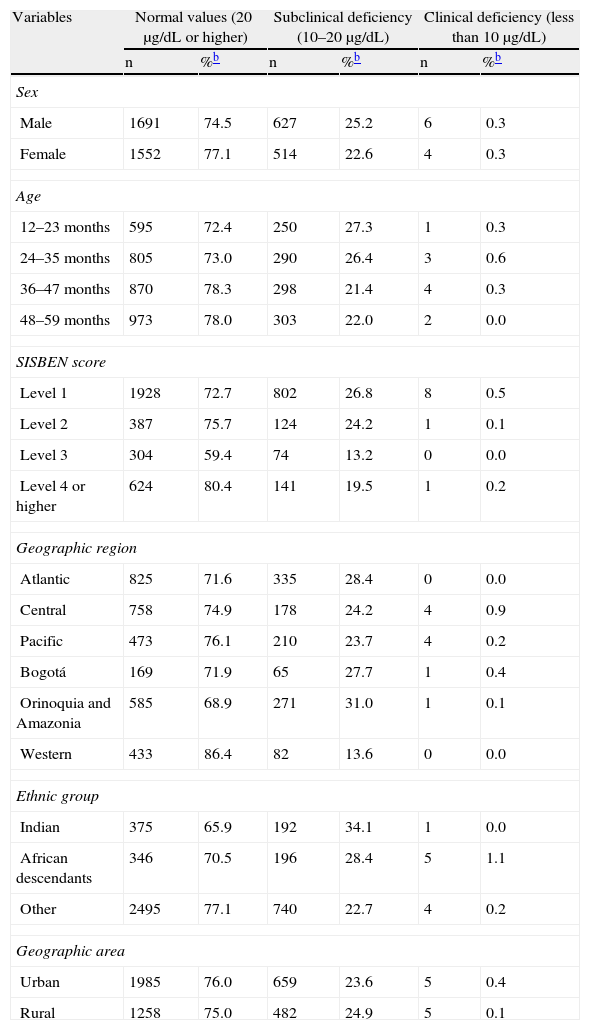
ResultsThe sample consisted of 4394 children aged 12–29 months. Vitamin A levels ranged from 7.5 to 93.7μg/dL (mean=26.2μg/dL, 95% CI 25.9–26.5μg/dL). Vitamin A levels less than 20.0μg/dL (subclinical deficiency) were found in 24.3% (95% CI 23.0–25.4) of children tested. Children of African ascent, those living in Orinoquia and Amazonia, and the group aged 12–23 months had the greatest subclinical vitamin A deficiencies (29.5, 31.1, and 27.6%, respectively). All other characteristics are shown in Tables 1 and 2 by group and sociodemographic variable.
Distribution of vitamin A levels (μg/dL) in children aged 12–59 months by sociodemographic characteristics (n=4394).
| Variables | n | Mean | CI (95%) |
| Sex | |||
| Male | 2324 | 25.9 | 25.5–26.4 |
| Female | 2070 | 26.5 | 26.0–27.0 |
| Age | |||
| 12–23 months | 846 | 25.9 | 25.1–26.6 |
| 24–35 months | 1098 | 26.0 | 25.3–26.7 |
| 36–47 months | 1172 | 26.4 | 25.8–27.1 |
| 48–59 months | 1278 | 26.4 | 25.8–27.1 |
| SISBEN score | |||
| Level 1 | 2738 | 25.3 | 24.9–25.7 |
| Level 2 | 512 | 26.0 | 25.1–27.0 |
| Level 3 | 378 | 27.6 | 26.5–28.7 |
| Level 4 or higher | 766 | 27.9 | 27.1–28.7 |
| Geographic region | |||
| Atlantic | 1160 | 24.0 | 23.5–24.4 |
| Central | 940 | 25.7 | 25.0–26.3 |
| Pacific | 687 | 27.8 | 26.9–28.6 |
| Bogotá | 235 | 25.6 | 24.6–26.6 |
| Orinoquia and Amazonia | 857 | 24.5 | 23.7–25.3 |
| Western | 515 | 29.3 | 28.4–30.3 |
| Ethnic groupa | |||
| Indian | 568 | 23.4 | 22.5–24.3 |
| African descendants | 547 | 24.0 | 23.3–24.7 |
| Other | 3239 | 26.7 | 26.3–27.1 |
| Geographic area | |||
| Urban | 2649 | 26.3 | 25.9–26.7 |
| Rural | 1745 | 26.0 | 25.4–26.6 |
Prevalence of vitamin A deficiency by sociodemographic variables in Colombian children aged 12–69 months.
| Variables | Normal values (20μg/dL or higher) | Subclinical deficiency (10–20μg/dL) | Clinical deficiency (less than 10μg/dL) | |||
| n | %b | n | %b | n | %b | |
| Sex | ||||||
| Male | 1691 | 74.5 | 627 | 25.2 | 6 | 0.3 |
| Female | 1552 | 77.1 | 514 | 22.6 | 4 | 0.3 |
| Age | ||||||
| 12–23 months | 595 | 72.4 | 250 | 27.3 | 1 | 0.3 |
| 24–35 months | 805 | 73.0 | 290 | 26.4 | 3 | 0.6 |
| 36–47 months | 870 | 78.3 | 298 | 21.4 | 4 | 0.3 |
| 48–59 months | 973 | 78.0 | 303 | 22.0 | 2 | 0.0 |
| SISBEN score | ||||||
| Level 1 | 1928 | 72.7 | 802 | 26.8 | 8 | 0.5 |
| Level 2 | 387 | 75.7 | 124 | 24.2 | 1 | 0.1 |
| Level 3 | 304 | 59.4 | 74 | 13.2 | 0 | 0.0 |
| Level 4 or higher | 624 | 80.4 | 141 | 19.5 | 1 | 0.2 |
| Geographic region | ||||||
| Atlantic | 825 | 71.6 | 335 | 28.4 | 0 | 0.0 |
| Central | 758 | 74.9 | 178 | 24.2 | 4 | 0.9 |
| Pacific | 473 | 76.1 | 210 | 23.7 | 4 | 0.2 |
| Bogotá | 169 | 71.9 | 65 | 27.7 | 1 | 0.4 |
| Orinoquia and Amazonia | 585 | 68.9 | 271 | 31.0 | 1 | 0.1 |
| Western | 433 | 86.4 | 82 | 13.6 | 0 | 0.0 |
| Ethnic group | ||||||
| Indian | 375 | 65.9 | 192 | 34.1 | 1 | 0.0 |
| African descendants | 346 | 70.5 | 196 | 28.4 | 5 | 1.1 |
| Other | 2495 | 77.1 | 740 | 22.7 | 4 | 0.2 |
| Geographic area | ||||||
| Urban | 1985 | 76.0 | 659 | 23.6 | 5 | 0.4 |
| Rural | 1258 | 75.0 | 482 | 24.9 | 5 | 0.1 |
aEstimation of vitamin A percentages for gypsies and the San Andrés Archipelago is not accurate because of the size of these groups, and is therefore omitted.
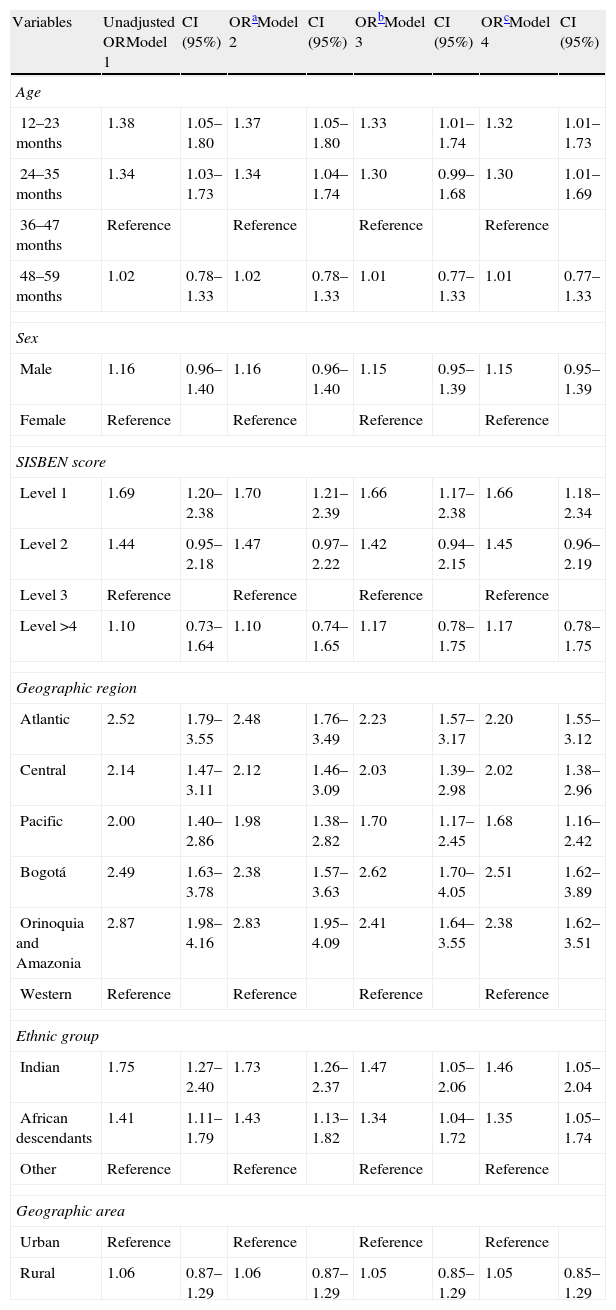
Table 3 shows the results of the simple and multiple logistic regression analyses. This table shows that having an age of 12–23 months (OR 1.38; 95% CI 1.05–1.80); being in SISBEN level 1 (OR 1.69; 95% CI 1.20–2.38); living in Orinoquia and Amazonia (OR 2.87; 95% CI 1.98–4.16), the Pacific (OR 2.00; 95% CI 1.40–2.86) and Atlantic (OR 2.52; 95% CI 1.79–3.55) regions, and Bogotá (OR 2.49; 95%CI 1.63–3.78); and being African descendants (OR 1.41; 95% CI 1.11–1.79) and Indians (OR 1.75; 95% CI 1.27–2.40) were factors predisposing to the presence of vitamin A deficiency in simple analysis.
Subclinical vitamin A deficiency (10–20μg/dL) and associated sociodemographic factors in Colombian children aged 12–59 months.
| Variables | Unadjusted ORModel 1 | CI (95%) | ORaModel 2 | CI (95%) | ORbModel 3 | CI (95%) | ORcModel 4 | CI (95%) |
| Age | ||||||||
| 12–23 months | 1.38 | 1.05–1.80 | 1.37 | 1.05–1.80 | 1.33 | 1.01–1.74 | 1.32 | 1.01–1.73 |
| 24–35 months | 1.34 | 1.03–1.73 | 1.34 | 1.04–1.74 | 1.30 | 0.99–1.68 | 1.30 | 1.01–1.69 |
| 36–47 months | Reference | Reference | Reference | Reference | ||||
| 48–59 months | 1.02 | 0.78–1.33 | 1.02 | 0.78–1.33 | 1.01 | 0.77–1.33 | 1.01 | 0.77–1.33 |
| Sex | ||||||||
| Male | 1.16 | 0.96–1.40 | 1.16 | 0.96–1.40 | 1.15 | 0.95–1.39 | 1.15 | 0.95–1.39 |
| Female | Reference | Reference | Reference | Reference | ||||
| SISBEN score | ||||||||
| Level 1 | 1.69 | 1.20–2.38 | 1.70 | 1.21–2.39 | 1.66 | 1.17–2.38 | 1.66 | 1.18–2.34 |
| Level 2 | 1.44 | 0.95–2.18 | 1.47 | 0.97–2.22 | 1.42 | 0.94–2.15 | 1.45 | 0.96–2.19 |
| Level 3 | Reference | Reference | Reference | Reference | ||||
| Level >4 | 1.10 | 0.73–1.64 | 1.10 | 0.74–1.65 | 1.17 | 0.78–1.75 | 1.17 | 0.78–1.75 |
| Geographic region | ||||||||
| Atlantic | 2.52 | 1.79–3.55 | 2.48 | 1.76–3.49 | 2.23 | 1.57–3.17 | 2.20 | 1.55–3.12 |
| Central | 2.14 | 1.47–3.11 | 2.12 | 1.46–3.09 | 2.03 | 1.39–2.98 | 2.02 | 1.38–2.96 |
| Pacific | 2.00 | 1.40–2.86 | 1.98 | 1.38–2.82 | 1.70 | 1.17–2.45 | 1.68 | 1.16–2.42 |
| Bogotá | 2.49 | 1.63–3.78 | 2.38 | 1.57–3.63 | 2.62 | 1.70–4.05 | 2.51 | 1.62–3.89 |
| Orinoquia and Amazonia | 2.87 | 1.98–4.16 | 2.83 | 1.95–4.09 | 2.41 | 1.64–3.55 | 2.38 | 1.62–3.51 |
| Western | Reference | Reference | Reference | Reference | ||||
| Ethnic group | ||||||||
| Indian | 1.75 | 1.27–2.40 | 1.73 | 1.26–2.37 | 1.47 | 1.05–2.06 | 1.46 | 1.05–2.04 |
| African descendants | 1.41 | 1.11–1.79 | 1.43 | 1.13–1.82 | 1.34 | 1.04–1.72 | 1.35 | 1.05–1.74 |
| Other | Reference | Reference | Reference | Reference | ||||
| Geographic area | ||||||||
| Urban | Reference | Reference | Reference | Reference | ||||
| Rural | 1.06 | 0.87–1.29 | 1.06 | 0.87–1.29 | 1.05 | 0.85–1.29 | 1.05 | 0.85–1.29 |
After adjustments for age, sex, ethnic group, region, geographic area and SISBEN score, the association was maintained in the group aged 12–23 months (OR 1.32 95% CI; 1.01–1.73); in children belonging to SISBEN level 1 (OR 1.66; 95% CI 1.18–2.34) living in the Orinoquia and Amazonia (OR 2.38; 95% CI 1.62–3.51), Pacific (OR 1.68; 95% CI 1.16–2.42), and Atlantic (OR 2.20; 95% CI 1.55–3.12) regions, and being African descendants (OR 1.35 95% CI 1.05–1.74) and Indians (OR 1.46; 95% CI 1.05–2.04) were associated to vitamin A deficiency.
DiscussionThe main finding of this study was that 24.3% of Colombian children had subclinical vitamin A deficiency (levels <20μg/dL). This is higher than the prevalence rates established by the WHO/UNICEF for a public health problem (>20%).2–5 Low vitamin A levels have been shown to be associated to respiratory and diarrheal disease and to increase the frequency, severity, and mortality of almost all infectious diseases.10 Primary deficiency is associated to keratinization of mucosal membranes, skin, and ocular epithelium, decreasing the barrier mechanism against infections. In the long term, this causes night blindness and corneal ulcers, appetite inhibition, taste loss, and growth inhibition.11
Some studies have shown that boys are more prone to subclinical vitamin A deficiency12 In this study, however, deficiency was similarly common in both sexes, as reported by other authors13–15 It should also be noted that prevalence rates of retinol deficiency by age group were similar to those reported by Santo et al.16 in Brazilian children. A comparison of the values reported by Poveda et al.17 in Colombian children aged 2–5 years from Funza-Cundinamarca with data reported in children from Costa Rica and Ecuador showed that the deficiency was less common in this study than reported in Funza (4.6%) and Costa Rica (8.8%),18 and very similar to that found in Ecuador (18%)19 in children with ages similar to those in our study. Such differences in prevalence probably reflect the unique characteristics of each country or region, the methods used to measure vitamin A levels, and social disparities that also cause differences in the probability of occurrence of the nutritional deficiency.
The results of this study also show that social determinants such as lower SISBEN 1 scores (an indicator of low socioeconomic level) (OR 1.66; 95% CI 1.18–2.34) and being of African ascent (OR 1.35; 95% CI 1.05–1.74) were associated as factors that are predisposing to experience vitamin A deficiency; this result agrees with a UNICEF report20 stating that a majority of the 190 million schoolchildren with vitamin A deficiency live in Asia and Africa, in countries with high inequalities including poor access to health services and limited public policies directed to nutritional health, amongst others.21,22
Disaggregation of results by residence area found no associations between living in an urban (OR 1.05; 95% CI 0.85–1.29) vs a rural area for the risk of having subclinical vitamin A deficiency. However, prevalence was higher in the rural area (24.9%) than in the urban area (23.6%), a finding similar to that reported by Castejón et al.23 in Venezuela, where prevalence of subclinical vitamin A deficiency was 35.4%, being higher in the rural area (48.3%). Singh et al.24 reported prevalence rates of vitamin A deficiency close to 10% in India, lower than that found in the current study in Colombian children, with a higher prevalence in non-desert areas. These findings have also been associated to family composition and distribution, geographic location, crowding, and low income.22,25,26 However, other authors have found low vitamin A intake in all socioeconomic groups.27,28
On the other hand, Aguayo et al.29 estimate that approximately 42.4% of African children (43.2millions) are at risk of vitamin A deficiency. It is therefore urgent to undertake multisectorial strategies that allow for counteracting the negative impact related to the burden of infectious and chronic non-transmissible diseases which may be attributed to vitamin A deficiency in children.
Wide evidence (meta-analyses and clinical trials) is available showing marked decreases in mortality (up to 30%) in children aged 6–59 months receiving vitamin A supplementation30,31 Such evidence is however less clear in African countries32 and even in some Latin American countries because, as suggested by the results of this study, the numbers continue to be significant for countries such as Colombia.
Recent data suggest that malnutrition (including vitamin A deficiency) caused approximately 45% of all deaths of children under 5 years of age in 2011.33 In addition, the WHO34 recently issued the scientific guideline for the program to administer vitamin A supplements to infants and children aged 6–59 months. Strengthening of nutritional safety programs for pregnant women and schoolchildren is currently required, and should be associated to a strong reduction in health inequalities in the frame of social determinants of health, in order to achieve significant improvements in the deficiency rates of vitamin A and other micronutrients in the Colombian and international pediatric population.
Overall, this study demonstrates the high prevalence of subclinical vitamin A deficiency as an indicator of health and food safety in the pediatric Colombian population, and discusses some socioeconomic determinants related to this situation. It should be considered that children with a specific deficiency of a micronutrient normally have multiple deficiencies that contribute to an impaired weight and height growth.
As a conclusion, it may be stated that one out of every four children aged 12–59 months had vitamin A deficiency. These results reinforce the strong evidence for the need to strengthen health actions that allow for systematization of prevention and treatment measures to reduce the high prevalence of subclinical vitamin A deficiency in early childhood in Colombia.
Conflicts of interestThe authors state that they have no conflicts of interest.
The authors thank the Colombian Institute for Family Well-being and PROFAMILIA for their support.
Please cite this article as: Martínez-Torres J, Meneses-Echavéz JF, Ramírez-Vélez R. Prevalencia de deficiencia subclínica de vitamina A y factores sociodemográficos asociados en niños de 12-59 meses de edad en Colombia. Endocrinol Nutr. 2014;61:460–466.
