


The 2012 Consensus Document on “The vaccination of risk groups against the influenza virus”,1 coordinated by Dr. Ramón Cisterna and prepared with the collaboration of the Spanish Influenza Group, the General Board of Nursing, and various medical scientific societies, including the Spanish Society of Endocrinology and Nutrition (SEEN), was recently issued. The consensus sets down the populations which should be vaccinated against influenza because of their greater susceptibility to contagion and/or morbidity and mortality if they experience the disease (Table 1). It is also stated that the World Health Organization and the European Commission have set as an objective for 2015 that at least 75% of the population at risk be vaccinated annually against seasonal influenza. According to the Consensus Document, the current situation in Spain is so far from achieving this target that in hardly any risk group does the vaccination rate even reach 50%.
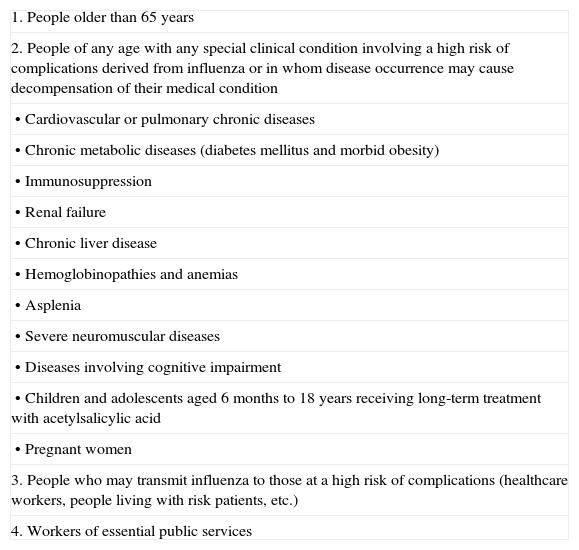
Groups included in influenza vaccination programs in Spain.
| 1. People older than 65 years |
| 2. People of any age with any special clinical condition involving a high risk of complications derived from influenza or in whom disease occurrence may cause decompensation of their medical condition |
| • Cardiovascular or pulmonary chronic diseases |
| • Chronic metabolic diseases (diabetes mellitus and morbid obesity) |
| • Immunosuppression |
| • Renal failure |
| • Chronic liver disease |
| • Hemoglobinopathies and anemias |
| • Asplenia |
| • Severe neuromuscular diseases |
| • Diseases involving cognitive impairment |
| • Children and adolescents aged 6 months to 18 years receiving long-term treatment with acetylsalicylic acid |
| • Pregnant women |
| 3. People who may transmit influenza to those at a high risk of complications (healthcare workers, people living with risk patients, etc.) |
| 4. Workers of essential public services |
The consensus is therefore an action aimed at promoting awareness by healthcare professionals, so that they promote the vaccination of risk groups within their area of influence. In the field of endocrinology, the groups for which vaccination should be recommended include people over 65 years of age, irrespective of disease, diabetic patients, and people with morbid obesity.
Apart from the generic indication in people aged over 65, vaccination has traditionally been recognized to be indicated in diabetic patients because of both the greater morbidity and mortality associated with influenza in these patients and the efficacy shown by the vaccine in them. In this regard, it should be remembered that influenza is the main cause of increased winter mortality in diabetic patients2 and that vaccination has been shown to reduce this increased mortality attributable to influenza infection in Spain.3 In fact, the American Diabetes Association (ADA) recommends in its annual clinical practice guidelines annual vaccination against influenza of all patients with diabetes for longer than 6 months.4
Despite the foregoing, in standard clinical practice endocrinologists are usually more attentive to other aspects of the ADA guidelines such as, for instance, annual eye fundus examination or the measurement of urinary albumin excretion than to influenza vaccination, as shown by data from the 2011 Gripometro project estimating a 47.5% vaccination rate in diabetic patients under 65 years of age.5 We must therefore reconsider our care approach and include, amongst other measures to be considered every year in diabetic patients, prophylaxis for influenza by vaccination.
In addition to this “classical” recommendation for diabetic patients, the consensus also advises vaccination in subjects with morbid obesity. The susceptibility of obese patients to the influenza virus was first shown in 2009 during the influenza A pandemic caused by virus H1N1. In Spain, the Ministry of Health and Social Policy issued from the early stages of infection a number of reports identifying morbid obesity as a risk factor (RF) for morbidity and mortality from the infection, while publications in other countries simultaneously supported these findings. After the end of the pandemic H1N1 infection, a study reporting the complete data concerning the characteristics of the infection in Spain clearly supported the data in the initial reports and confirmed morbid obesity as the main RF for requiring hospital admission for H1N1 infection with an odds ratio (OR) of 14.27 (confidence interval [CI]: 1.67–91.7).6
These data obviously raised the question as to whether susceptibility to H1N1 in obesity could be extended to seasonal influenza or was only a limited association due to some characteristic of the influenza A pandemic. Illustrative results were provided in this regard by Kwong et al.7 who, after examining the body mass index of patients admitted in Ontario (Canada) for 12 influenza seasons, found that type II or III obese patients had an OR of 2.12 (CI: 1.45–3.10), as compared to normal weight subjects, for requiring admission for respiratory reasons during the influenza season. More importantly, this increased risk remained regardless of whether or not obese patients had other RFs. In other words, obesity per se, irrespective of other associated comorbidities (diabetes, cardiovascular disease, sleep apnea, etc.), was a RF for a poorer course of seasonal influenza and for hospital admission.
These findings suggest the need to widen our view of morbidly obese patients and their comorbidities to take into account their greater susceptibility to and/or poorer course after influenza infection.
However, data about the efficacy of vaccination for prophylaxis of influenza in patients with morbid obesity are scant and conflicting. Countries such as the United States have however included morbid obesity in the list of conditions for which empiric antiviral treatment is advised during infection. The consensus approach of recommending empiric prophylaxis for influenza in this group, even in the absence of studies showing its efficacy, therefore appears reasonable. Thus, our clinical practice should include, in addition to the recommendations concerning diet and exercise usually given to patients with morbid obesity, systematic advice about the need for vaccination during the established periods.
In the specific case of morbidly obese patients, apart from an awareness by healthcare professionals of prophylaxis for influenza infection, we face another problem. Unlike diabetic patients, not all subjects with morbid obesity are under medical control. Most of them do not see themselves as “patients”, and do not therefore seek medical care. As admitted by the consensus itself, obese subjects are the risk group least aware of having a disease that makes vaccination advisable (only 44.1% are aware of this need). Only patients who want to lose weight are referred from another medical specialty and may attend endocrinology and nutrition or primary care clinics, provided they do not end up in other “alternative” weight reduction clinics. This restricts our access to many of these patients and, thus, the possibility of implementing vaccination in the greater part of this population group. The only way to approach this situation is to implement health education campaigns to raise awareness in the population of the risks of obesity, the need to rely on a physician and, specifically, the benefits of influenza vaccination in morbidly obese patients.
In conclusion, it may be stated that the 2012 consensus on “The vaccination of risk groups against the influenza virus” identifies both where action is required and how it can be implemented. We, as healthcare professionals, should take note of the message and act accordingly. As endocrinologists, it would be very positive if we assumed the joint responsibility for the achievement of the overall healthcare objective of annually vaccinating at least 75% of the risk population. For this, we should get into the habit of recording in the history of our risk groups (diabetes mellitus and morbid obesity) whether patients have already received seasonal vaccination, much in the same way as the result of an annual eye fundus examination of a diabetic patient is recorded. This would allow us to tabulate, after each campaign, the volume of patients who have followed our recommendations. In addition, it should not be forgotten that, as healthcare professionals who may transmit influenza to patients with a high risk of complications from infection, we must assume our own personal responsibility by vaccinating ourselves.
Please cite this article as: Gargallo Fernández M., Vacunación de la gripe en enfermedades endocrinas. ¿Lo tenemos en mente? Endocrinol Nutr. 2013;60:221–3.
Representative of SEEN in the 2012 Consensus Document on “The vaccination of risk groups against the influenza virus”.
