





The aim of this study is to analyze the impact of anxiety and psychological well-being of couples in the transition to parenthood. A sample of 256 participants was divided into five groups: 54 “not seeking pregnancy”, two groups seeking pregnancy, 50 “infertile that did not get pregnant” and 50 “infertile that achieves pregnancy”, 50 “natural pregnancy”, and 52 “fertile with children”. State-Trait Anxiety Inventory (STAI) and Psychological Well-being in Couple Scale (EBP in Spanish) were used. The “infertile group that achieves pregnancy” gets the highest state-anxiety levels, even though regarding the anxiety-trait the group that is “not seeking pregnancy” shows the highest levels. Regarding psychological wellbeing in couples, the “natural pregnancy” group shows the lowest scores. These results demonstrate the possible functional role that anxiety-state in non-clinical levels can play in getting pregnant and confirm that psychological well-being in couple's relationship decreases only during pregnancy.
El objetivo de este estudio es analizar el impacto de la ansiedad y el bienestar psicológico de la pareja en la transición a la paternidad. Una muestra de 256 participantes se dividió en cinco grupos: 54 “no buscan embarazo”, dos grupos que buscan el embarazo, 50 “infértil que no consiguen embarazo” y 50 “infértil que logra el embarazo”, 50 “embarazo natural” y 52 “fértil con niños”. Se utilizó el Inventario de Ansiedad Estado-Rasgo (STAI) y la Escala de Bienestar Psicológico de la pareja (EBP). El “grupo infértil que logra el embarazo” es el que tiene más altos niveles de ansiedad estado, aunque, en relación con la ansiedad rasgo, es el grupo que “no busca embarazo” el que muestra los niveles más altos. En cuanto al bienestar psicológico en la pareja, el grupo “embarazo natural” es el que muestra las puntuaciones más bajas. Estos resultados demuestran el posible papel funcional que la ansiedad estado en los niveles no clínicos puede jugar en el embarazo y confirma que el bienestar psicológico en la relación de pareja disminuye sólo durante el embarazo.
The transition to parenthood may be perceived as a positive life event but it can also be one of the most stressful and challenging changes in life (Deave, Johnson, & Ingram, 2008; Fillo, Simpson, Rholes, & Kohn, 2015). Parenthood can be regarded as a mental state, a stage of life, a personal choice, a psychological and biological transition, and a great need for the evolution of the species (Swain, 2011). Undoubtedly, the birth of the first child transforms the lifestyle of couples and forces them to make significant changes in their dynamics and functioning in order to adapt to their new roles as parents (Ohashi & Asano, 2012). The transition from pregnancy to parenting involves periods of adjustment, modifying the lifestyle from one stage to another. These periods have important implications for parents, for the parent-child relationship, and for infant development.
But parenting is not a single event but a process. Typically, it begins with pregnancy (or for some couples even before pregnancy, with planning, fertility tests, or by taking prenatal vitamins) and ends a few months after birth. During the transition to parenthood, the couple undergoes a profound transformation, differentiating their relationship into two subsystems: the conjugal dynamics and the co-parenting dynamics (Bouchard, 2014). Some authors suggest that couples become more dissatisfied with their relationship after having children, because the arrival of a new member requires the reorganization of the family dynamics, which can be experienced as a “crisis” (Twenge, Campbell, & Foster, 2003). According to Cowan and Cowan (1995), on average the satisfaction with the relationship usually decreases after the birth of the first child. Thus, for some people it means changes in their life role, the development of chronic fatigue, increased financial burdens, and greater work-family conflict, all of which can increase stress levels. Frequently there is a decrease in marital satisfaction, couple's activities, a reduction in sexual and intimate activities, a reorganization of work and leisure time, and increased conflict (Adamsons, 2013; Cowan & Cowan, 1995; Fillo et al., 2015; Lawrence, Rothman, Cobb, & Bradbury, 2012). The adjustment that occurs during the transition to parenthood differs significantly by sex. Thus, women tend to report higher levels of stress and greater decrease in marital satisfaction than their partners (Bouchard, 2014; Gameiro, Moura-Ramos, Canavarro, Almeida-Santos, & Dattilio, 2011), as well as greater changes in lifestyles and routines (Deave et al., 2008). Nevertheless, in some cases the transition to parenthood may not lead to negative effects (Twenge et al., 2003). Some parents maintain the same levels of satisfaction they had before the birth of the baby and some relationships even improve (Cowan & Cowan, 1995; Fillo et al., 2015; Lawrence et al., 2012; Twenge et al., 2003).
The transition to parenthood is by nature multidimensional and complex, encompassing cultural aspects (de Montigny & de Montigny, 2013) and biological, psychological, dyadic, and social dimensions (Testa, 2010) and so, deciding to have children is one of the most important issues many couples face in their lifes. Unlike earlier times, thanks to contraception, couples today are free to decide when to have children and how many they are going to have. When deciding on this issue, they can also consider whether having a child will affect their relationship (Mortensen, Torsheim, Melkevik, & Thuen, 2012).
Many pregnancies are unplanned, babies are born earlier than young couples might want, some are parents without having planned to stay together long term and others unexpectedly become parents as older adults. Even for those that have planned, it may take some time to achieve pregnancy (Redshaw & Martin, 2009). In the field of fertility, the goal is a child, the act is giving birth, the context is the couple, and all this in a short period of time, which can make the intention to have children be more realistic (Testa, Cavalli, & Rosina, 2012). However, many couples decide to postpone parenthood, waiting for the right time (job, economic, emotional security, etc.) thinking that when the time arrives they will have children. On occasions, the right time comes but desires and nature do not come together and then couples must face making complicated decisions such as deciding to not be parents, to adopt or undergo infertility testing and/or treatment (Redshaw & Martin, 2009).
In this last case, in addition to the transition from being a couple to a family, the couple must also make the transition from infertility to medically assisted fertility. If we consider the experience of infertility as a stressful life event, it follows that the stress associated with infertility will affect the quality of subsequent interactions in families who have conceived by assisted reproduction (Cairo et al., 2012). For some, the word paternity and/or maternity evokes memories, for others a desire, and for many an idealization (Swain, 2011), since for people in infertility treatment, this fact is preceded by many years of efforts, dreams, and desires. However, according to Gameiro et al. (2011) couples who conceive through ART report higher levels of marital satisfaction in the transition to parenthood. According to these authors, this increase is due to the experience of infertility, because during this time the relationship can become stronger. In fact, many couples think that infertility has strengthened their marriage, enabling them to face other difficulties.
However, the decision to delay parenthood is not without consequences. In addition to reduced fertility, it can lead to the need for more prenatal tests in the first months of pregnancy, more interventions during labor and higher rates of caesarean section, and, more commonly in older women, poorer physical health after birth. Therefore, postponing parenthood may seem appropriate at a given time but can be regretted (Redshaw & Martin, 2009). Moreover, successful treatment does not guarantee that women will adapt easily to their new lifestyle. Difficulties in adapting to pregnancy are particularly common among infertile women.
In general terms, the pregnancy itself is a state in which the physical, psychological, and social changes can disrupt the couple because it is not only a complex psychological process but it is also an important event in the life of the woman, her partner, and their families (Lepecka-Klusek & Jakiel, 2007). Many studies describe pregnancy as a time which is a challenge for some couples, often characterized by changes in the dynamics of the relationship (Martin & Redshaw, 2010) and/or lowering of the quality (Dulude, Bélanger, Wright, & Sabourin, 2002). Acording to Henriksen, Torsheim, and Thuen (2015) the level of relationship satisfaction predicts the risk of infectious diseases in pregnancy. These results are especially important because infectious diseases have the potential to harm the mother and the developing fetus when they occur during pregnancy. Moreover, stress during pregnancy has adverse effects on emotional health. Thus, pregnant women who have stress have a higher risk of substance abuse, developing preeclampsia and premature delivery (Flanagan, Gordon, Moore, & Stuart, 2015), such that high anxiety symptoms may affect fetal growth (Field et al., 2003). That is why some studies have focused on the search for interventions that promote the wellbeing of pregnant women. So, it has been found that relaxation causes a significant decrease in negative emotional states such as anxiety during pregnancy (Guszkowska, Lagwald, & Sempolska, 2013), since it favors states of wellbeing and positive emotionality, promotes bonding of the pregnant mother with the fetus and helps them face and manage stress, and this favors the mother and the unborn child (Nereu-Bjorn, Neves de Jesus, & Casado-Morales, 2013).
Thus, taken as a whole, the transition to parenthood encompasses different moments, ranging from a decision not to have children, to then trying, then waiting, and finally parenting. At each stage the relationship is different, and stressful situations can bring out anxiety symptoms. Although stress and/or anxiety are an adaptive response that can be beneficial to increasing and maintaining performance and health, its excess or deficiency, quantitatively or qualitatively, can be harmful. Thus, the optimal level of activation is one that, in each case, favors the best physical and psychological functioning and, therefore, maximum performance within the real possibilities of each person. Activation levels below or above the optimal level lead to faulty functioning, which impairs performance (Buceta-Fernández, Mas-García, & Bueno-Palomino, 2012). Anxiety and stress are multifaceted concepts and their measurement requires specific cognitive, behavioral, and physiological measures (Koster, 2012).
This research is a continuation of a preliminary study that evaluated symptoms of depression and anxiety and psychological well-being in men and women in their third trimester of pregnancy, compared with two control groups of men and non-pregnant women, both with children and without children (Arnal-Remón, Moreno-Rosset, Ramírez-Uclés, & Antequera-Jurado, 2015). This study seeks to extend our understanding of the role of anxiety and satisfaction in couples’ relationships through more transition to parenthood stages, ranging from couples not seeking pregnancy, two groups seeking pregnancy (one infertile group that does not get pregnant and one that finally gets pregnant with assisted reproduction techniques), those who are naturally pregnant and those with children.
MethodParticipantsThe total sample used in this study consisted of 256 heterosexual participants, 126 men (mean age=35.45, SD=4.11) and 130 women (mean age=33.85, SD=4.02). The sample was divided into five groups depending on the different stages in the transition to parenthood: “not seeking pregnancy” group, 54 participants (mean age 31.63, SD=4.60), two groups seeking pregnancy, “infertile that did not get pregnant”, 50 participants (mean age 35.74, SD=1.78), “infertile that achieves pregnancy”, 50 participants (mean age 34.10, SD=4.11), “natural pregnancy” group, 50 participants in their third trimester of pregnancy (mean age 34.48, SD=3.08) and “fertile with children” group, 52 participants (mean age 37.38, SD=4.35). All couples invited to participate accepted.
ProcedureTotal sample assessment was carried out in a local community health center in Zaragoza (Spain). Evaluation of couples’ anxiety and psychological well-being was done in the “natural pregnancy” group approximately in the middle of the third trimester at birth school classes. The group that is “not seeking pregnancy” and the “fertile with children” group were assessed when they went to the same center for health consultations which were neither major medical nor psychological problems. Both infertile groups turned to the medical center after at least one year of unprotected sexual relations with no positive results, and were assessed before starting assisted reproduction treatment (ART). After the ART, we selected two groups depending on whether or not they had achieved pregnancy. The psychologist explained the aims of the study to get informed consent from all participants. The questionnaires were presented by one of the study authors (B. A-R). Each participant completed a sociodemographic, medical, and psychological questionnaire in order to assess compliance with the general inclusion criteria (being of legal age, not having suffered serious psychological disorders or mood disorder and/or anxiety disorders, and not taking drugs that could destabilize mood) and with specific criteria depending on the group they would be part of. Specific criteria for “not seeking pregnancy” group were not trying to conceive and not having tried it previously, even with another couple. Specific criteria for both “infertile” groups were having an infertility diagnosis being at least one year having unprotected sexual relations without pregnancy success, not having yet begun any ART, not having suffered any previous miscarriage, and not having children from any previous relationships. Specific criteria for the “natural pregnancy” group were having conceived naturally without undergoing any ART, with gestational development free from medical and/or psychological complications. Finally, specific criteria for “fertile with children” group were not being pregnant and not trying to conceive, and having given birth after a natural pregnancy. The entire sample was matched in terms of socioeconomic and educational levels. All participants signed the necessary agreements. The study was approved by both Health Center Ethics’ boards and by the Research Ethics Committee of the Universidad Nacional de Educación a Distancia (UNED).
MeasuresAnxiety was measured using the Spanish version of the State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch, & Lushene 2008), which comprises two scales of 20 items, each one assessing current (state) and general (trait) symptoms of anxiety. The internal consistency of studies in the Spanish population has a Cronbach alpha .90 for trait-anxiety and .94 for state-anxiety. The STAI is appropriate in the general population and recent years have seen a growing number of publications utilizing the inventory in pregnant populations (Gunning et al., 2010).
Marital relationships were evaluated with the Psychological Well-being in the couple Scale (EBP in Spanish; Sánchez-Cánovas, 2007). Created and validated in Spain, it consists of 15 items with different formats for both men and women, and describes personal attitudes in relation to sexuality and other relations in the couple. The internal consistency coefficient is .88.
DesignA bifactorial intergroup design 3 x 2 was used, considering group and sex as independent variables, and the scores obtained in the above-described questionnaires/subscales as dependent variables.
Data AnalysisThe following data analyses were conducted: a bifactorial intergroup 3 x 2 MANOVA, taking group and sex as independent variables and the scores obtained in STAI as dependent variables, and a bifactorial intergroup 3 x 2 ANOVA, taking the same independent variables as before and the scores obtained in the EBP as dependent variable.
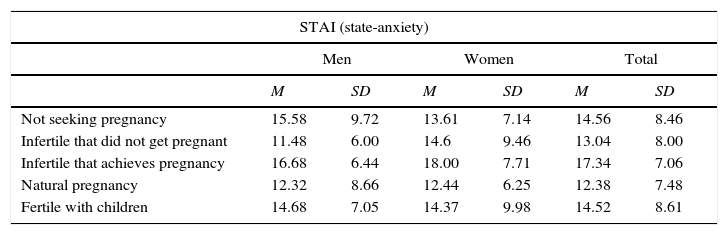
ResultsTable 1 shows the mean values and standard deviations of the scores obtained in the different questionnaires. In what follows we provide the mean values obtained in each questionnaire as a function of groups and sex (see Figures 1, 2 and 3).
Mean and Standard Deviations of the Scores obtained in the Different Questionnaires
| STAI (state-anxiety) | ||||||
|---|---|---|---|---|---|---|
| Men | Women | Total | ||||
| M | SD | M | SD | M | SD | |
| Not seeking pregnancy | 15.58 | 9.72 | 13.61 | 7.14 | 14.56 | 8.46 |
| Infertile that did not get pregnant | 11.48 | 6.00 | 14.6 | 9.46 | 13.04 | 8.00 |
| Infertile that achieves pregnancy | 16.68 | 6.44 | 18.00 | 7.71 | 17.34 | 7.06 |
| Natural pregnancy | 12.32 | 8.66 | 12.44 | 6.25 | 12.38 | 7.48 |
| Fertile with children | 14.68 | 7.05 | 14.37 | 9.98 | 14.52 | 8.61 |
| STAI (trait-anxiety) | ||||||
|---|---|---|---|---|---|---|
| Men | Women | Total | ||||
| M | SD | M | SD | M | SD | |
| Not seeking pregnancy | 19.73 | 8.67 | 18.96 | 6.48 | 19.33 | 7.55 |
| Infertile that did not get pregnant | 12.76 | 6.27 | 17.72 | 8.28 | 15.24 | 7.69 |
| Infertile that achieves pregnancy | 16.00 | 6.91 | 19.88 | 6.61 | 17.94 | 6.97 |
| Natural pregnancy | 12.76 | 5.15 | 16.40 | 7.38 | 14.58 | 6.55 |
| Fertile with children | 13.36 | 8.58 | 16.15 | 7.86 | 14.81 | 8.25 |
| Psychological well-being in couples (EBP) | ||||||
|---|---|---|---|---|---|---|
| Men | Women | Total | ||||
| M | SD | M | SD | M | SD | |
| Not seeking pregnancy | 64.31 | 5.66 | 64.30 | 7.63 | 64.30 | 6.67 |
| Infertile that did not get pregnant | 64.56 | 7.01 | 63.64 | 5.73 | 64.10 | 6.36 |
| Infertile that achieves pregnancy | 63.48 | 7.43 | 64.88 | 5.15 | 64.18 | 6.36 |
| Natural pregnancy | 55.12 | 8.87 | 56.64 | 7.75 | 55.88 | 8.28 |
| Fertile with children | 62.20 | 5.66 | 62.27 | 7.44 | 62.24 | 6.56 |
.")
.")
.")
The MANOVA group x sex results for the anxiety variable illustrate a significant effect of the group variable (Wilks’ Lambda=.88, F(8, 490)=4.00, p=.00, η2p=.06, β=.99) and of the sex variable, Wilks’ Lambda=.94, F(2, 245)=7.53, p=.00, η2p=.05, β=.33 (see Table 2).
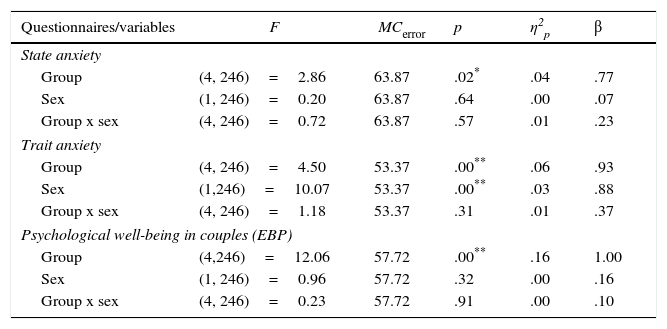
The ANOVA results for dependent variables state and trait-anxiety (see Table 3) illustrate a significant effect of group on the state-anxiety, F(4, 246)=2.86, MCe=63.87, p=.02, η2p=.04, β=.77, and trait-anxiety, F(4, 246)=4.50, MCe=53.37, p=.00, η2p=.06, β=.93; and of sex on the trait-anxiety, F(1, 246)=10.07, MCe=53.37, p=.00, η2p=.03, β=.88, with women showing in general higher scores than men (see Figure 2).
ANOVA Group x Sex Results for the Different Scales and Subscales of the Questionnaires
| Questionnaires/variables | F | MCerror | p | η2p | β |
|---|---|---|---|---|---|
| State anxiety | |||||
| Group | (4, 246)=2.86 | 63.87 | .02* | .04 | .77 |
| Sex | (1, 246)=0.20 | 63.87 | .64 | .00 | .07 |
| Group x sex | (4, 246)=0.72 | 63.87 | .57 | .01 | .23 |
| Trait anxiety | |||||
| Group | (4, 246)=4.50 | 53.37 | .00** | .06 | .93 |
| Sex | (1,246)=10.07 | 53.37 | .00** | .03 | .88 |
| Group x sex | (4, 246)=1.18 | 53.37 | .31 | .01 | .37 |
| Psychological well-being in couples (EBP) | |||||
| Group | (4,246)=12.06 | 57.72 | .00** | .16 | 1.00 |
| Sex | (1, 246)=0.96 | 57.72 | .32 | .00 | .16 |
| Group x sex | (4, 246)=0.23 | 57.72 | .91 | .00 | .10 |
*p<.05, **p<.01.
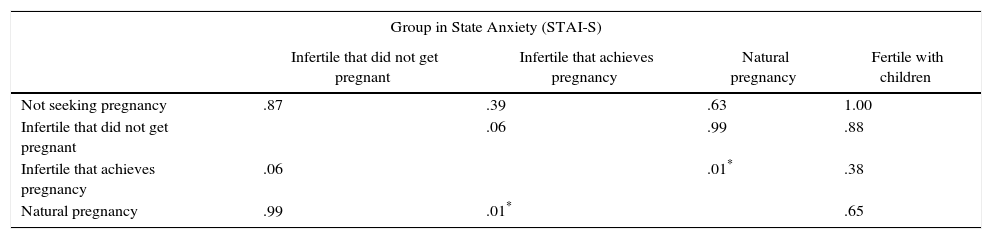
In order to illustrate the differences in scores obtained by the different groups in state and trait-anxiety, a posteriori Tukey comparisons were performed (see Table 4). Regarding state-anxiety, significant differences were found between “infertile that achieves pregnancy” group and “natural pregnancy” group (p=.01), being “infertile that achieves pregnancy” the group with highest scores. Regarding the results of group on trait-anxiety, significant differences were obtained between “not seeking pregnancy” group and “infertile that did not get pregnant” (p=.03), “natural pregnancy” (p=.00), and “fertile with children” (p=.01) groups, being ‘not seeking pregnancy’ the group with highest scores of trait-anxiety.
Post-hoc Tukey in Anxiety and Psychological Well-being in Couples
| Group in State Anxiety (STAI-S) | ||||
|---|---|---|---|---|
| Infertile that did not get pregnant | Infertile that achieves pregnancy | Natural pregnancy | Fertile with children | |
| Not seeking pregnancy | .87 | .39 | .63 | 1.00 |
| Infertile that did not get pregnant | .06 | .99 | .88 | |
| Infertile that achieves pregnancy | .06 | .01* | .38 | |
| Natural pregnancy | .99 | .01* | .65 | |
| Group in Trait Anxiety (STAI-T) | ||||
|---|---|---|---|---|
| Infertile that did not get pregnant | Infertile that achieves pregnancy | Natural pregnancy | Fertile with children | |
| Not seeking pregnancy | .03* | .86 | .00** | .01* |
| Infertile that did not get pregnant | .34 | .99 | .99 | |
| Infertile that achieves pregnancy | .34 | .14 | .19 | |
| Natural pregnancy | .99 | .14 | 1.00 | |
| Group in psychological well-being in the couple (EBP) | ||||
|---|---|---|---|---|
| Infertile that did not get pregnant | Infertile that achieves pregnancy | Natural pregnancy | Fertile with children | |
| Not seeking pregnancy | .98 | .98 | .00** | .65 |
| Infertile that did not get pregnant | 1.00 | .00** | .93 | |
| Infertile that achieves pregnancy | 1.00 | .00** | .92 | |
| Natural pregnancy | .00** | .00** | .00** | |
*p<.05, **p<.01.
The ANOVA results taking group and sex as independent variables and the scores obtained in the psychological wellbeing in the couple (EBP) as dependent variable show a significant effect of group variable, F(4, 246)=12.06, MCe=57.72, p=.00, η2p=.16, β=1.00 (see Table 3).
A posteriori Tukey comparisons, performed (see Table 4) to illustrate the differences in EBP between the different groups, show significant differences between “natural pregnancy” group and the rest of the groups: “fertile with children” (p=.00), “not seeking pregnancy” (p=.00), “infertile that did not get pregnant” (p=.00), and “infertile that achieves pregnancy” (p=.00), being “natural pregnancy” the group with lowest scores (see Table 1, Figure 3).
DiscussionThe present study has shown that psychological wellbeing in couples changes throughout the different stages of parenthood. These results are consistent with those found by Adamsons (2013), Cowan and Cowan (1995), Fillo et al. (2015), and Lawrence et al. (2012). These changes are usually negative but transient, and can vary throughout the different stages of the transition and after the first year or year and a half after the birth of new child they stabilize (Lawrence, Rothman, Cobb, Rothman, & Bradbury, 2008), though they do not affect both partners equally. Our results at least partially confirm these data, as we found differences in satisfaction with the relationship between groups with a greater decline among those who are expecting a child (Dulude et al., 2002; Lawrence et al., 2008). Undoubtedly, women experience the physical, hormonal, and emotional changes more intensely during pregnancy and this difference in impact on both partners can contribute to the decline in the quality of their relationship. We must also consider that all participants in this group were in their third trimester and intimate and sexual relations may decline due to their own discomforts in this period, influencing a decline in overall marital satisfaction.
Our results also show that experiences prior to infertility play an important role in the levels of satisfaction with the relationship (Lawrence et al., 2008), since the infertile group that achieves pregnancy shows higher levels of couple wellbeing than the natural pregnancy group, with no significant differences in the other groups. This result reinforces the idea that couples that conceived through ART have a more satisfactory prenatal functioning (Cairo et al., 2012), since the experience of infertility strengthens the marital relationship (Gameiro et al., 2011). This also justifies that there are no significant differences between the infertile group that did not get pregnant and those that finally become pregnant because, regardless of having or not having success, both have undergone infertility treatment.
There are several studies that provide evidence that, with the arrival of the child, there is a decline in the quality of the relationship (Adamsons, 2013; Cowan & Cowan, 1995; Fillo et al., 2015; Lawrence et al., 2012). However, in our study, although the group that is not seeking pregnancy shows higher levels of satisfaction in the couple, this result does not have statistical significance with fertile couples with children. So, we cannot say that a decrease in marital satisfaction occurs when one is already a parent, which can be explained by intrapersonal factors (such as strategies for coping with stressful situations or previous expectations of parenthood), or by dyadic factors (such as prenatal marital satisfaction and/or degree of pregnancy planning) or, finally, by factors of a contextual character (such as interference between work and family, the existence of other stressful life events or social support) that may be predictors of well-being in a couple with children (Lawrence et al., 2012). The transversal nature of our study does not allow us to provide information on this question, and so it should be contrasted with a prospective longitudinal study.
The results in state-anxiety draw attention because we observed a significant group effect, with the infertile group that achieved pregnancy obtaining higher scores compared to natural pregnancy group, which shows the functional role that state-anxiety can play relative to achieving pregnancy. Our results are aligned with studies that show that non-clinical levels of state-anxiety may be beneficial for becoming pregnant (Cooper, Gerber, McGettrick, & Johnson, 2007; de Klerck et al., 2008; Li, Newell-Price, Jones, Ledger, & Li, 2012). Thus, reaching an optimal level of activation would be functional to the success of these treatments as both a deficit of activation and/or excessive levels of stress may not be adaptive in achieving pregnancy. And this may have an interesting application in clinical practice where by following Anderheim, Holter, Bergh, and Möller (2005) we could guide interventions for couples undergoing ART that are focused on achieving an optimal and functional level of state anxiety that would help achieve pregnancy. However, other works showing that high levels of state-anxiety during the different ART stages predict adverse pregnancy outcomes and increase the probability of treatment abandonment (Demyttenaere et al., 1998; Smeenk et al., 2001) and those which show that state-anxiety levels of women who do not get pregnant are higher than those who get pregnant (Csemiczky, Landgren, & Collins, 2000).
On the other hand, women in the natural pregnancy group have the lowest scores on state-anxiety. The fact that this group was attending childbirth preparation classes reveals the importance these group sessions have for the psychological well-being, not only for pregnant women, but also for their partners; hence, there are no sex differences. In these classes, participants have the opportunity to share experiences, discuss the changes and concerns that they experience, and benefit from techniques such as relaxation, which has proved a useful tool for reducing anxiety levels and promote positive emotionality (Guszkowska et al., 2013; Nereu-Bjorn et al., 2013).
Contrary to what might be expected, the group of participants with children shows no difference in state-anxiety compared with the group of participants without children. As Ohashi and Asano (2012) note, stress levels increase after childbirth because of the demands of parenting and the difficulties in harmonizing with other roles, including marital. Our results are in line with those of Bouchard (2014) indicating that despite how stressful parenting can be, anxiety levels may depend on personal and partner's resources and capacity to tackle these changes.
The data on trait-anxiety are interesting because we did not expect to obtain significant differences between groups. However, the group not seeking pregnancy got the highest scores, and, if we understand the trait-anxiety as a personality factor that would include relatively stable individual differences that respond to situations perceived as threatening (Guillén-Riquelme & Buela-Casal, 2011), we can think that perhaps these people, in spite of obtaining non-clinical values in trait-anxiety, may be more likely to perceive being parents as threatening because of the changes in different areas of life (relationship, job, social, etc.) that it entails.
As regards sex differences, the results only show significant differences in levels of trait-anxiety, which is well known and referenced in the literature, regardless of the area in which we focus (McLean, Asnaani, Litz, & Hoffman, 2011). Although women have a greater tendency to trait-anxiety, they have similar levels of state-anxiety as men, so it seems that rather than individual characteristics, the level of anxiety presented by subjects at a particular time can be modulated by contextual (similar life events), relationship, and partner dynamics variables (Bouchard, 2014; Buceta-Fernández et al., 2012). As regards the welfare of the couple we found no differences by sex. Thus, the greater involvement of women during the transition to parenthood and their tendency to focus more on the role of mother than wife (Fox, 2009) does not necessarily affect their assessment of the relationship nor their partner's assessment. So, the increase in the changes that arise from the process of paterenting may be affecting other vital areas, but couples have the personal or dyadic resources needed to maintain the same levels of marital satisfaction.
The research presented in this article has some limitations. First, the groups, though homogeneous, consist of a small number of participants, so obtaining larger samples is necessary. Second, the transversal nature of the study does not allow us to detect or predict factors influencing each of the moments of this transition, including the full process of assisted reproduction treatment, the three trimesters of gestation, and the evolution as parents with children at different ages. However, we want to highlight some important contributions of our work. First, the use of five groups, each at a different stage of the transition to parenthood and all of them with equal male and female participation, in particular the use of a group of couples without children. Secondly, we were able to verify the importance of the functional role that anxiety may play in the goal of transition to parenthood, which is being parents.
ConclusionOur study aims to assess anxiety and psychological well-being through five different stages in the transition to parenthood: when couples are not seeking pregnancy, with an infertility diagnosis achieving pregnancy and not achieving pregnancy after ART, during pregnancy, particularly in the third trimester having conceived naturally, and when you are already a father/mother. Results indicate the importance of considering the time of transition to parenthood in relation to the psychological well-being, given that a reduction thereof may occur during pregnancy, thus leading to the development of potential emotional disorders, while an increase may appear in couples with infertility diagnosis that are strengthened to deal with assisted reproductive treatments.
It should be noted the importance of studying anxiety as a state in couples with infertility diagnosis because of the fact that, in contrast with common beliefs shared by some patients when going to their gynecologist by which nervousness and anxiety will hinder their goal of conception, we noted that non-clinical state-anxiety levels can contribute or at least not harm getting pregnant.
Financial SupportThis article was funded as part of the actions to aid the dissemination of the UNED Research Promotion Plan.
Conflict of InterestThe authors of this article declare no conflict of interest.
