









The surgical electronic logbook (surgical e-logbook) aims to: simplify registration of the training activities of surgical residents, and to obtain reliable and detailed reports about these activities for resident evaluation.
Methods:The surgical e-logbook is a unique and shared database. Residents prospectively record their activities in 3 areas: surgical, scientific and teaching. We can access activity reports that are constantly updated.
ResultsStudy period using the surgical e-logbook: Between June 2011 and May 2013. Number of surgeries reported: 4255. Number of surgical procedures reported: 11,907. Number of surgeries per resident per year reported: 250. Number of surgical procedures per resident per year reported: 700. Surgical activity as a primary surgeon during the first year of residency is primarily in emergency surgery (68.01%) and by laparotomy (97.73%), while during the fifth year of residency 51.27% is performed in elective surgery and laparoscopy is used in 23.10% of cases. During this period, residents participated in a total of 11 scientific publications, 75 conference presentations and 69 continuing education activities.
ConclusionsThe surgical e-logbook is a useful tool that simplifies the recording and analysis of data about surgical and scientific activities of the residents. It is a step forward in the evaluation of the training of surgical residents, however, is only an intermediate step towards the development of a larger Spanish registry.
El libro informático del residente quirúrgico (LIRQ) tiene por objetivos: simplificar el registro de la actividad formativa de los residentes quirúrgicos y permitir obtener informes fiables y detallados sobre la misma, para su evaluación.
Métodos:El LIRQ es una base de datos única y compartida. Los residentes registran de manera prospectiva sus actividades, en 3 bloques: quirúrgico, científico y docente. Permite acceder a informes de la actividad registrada, actualizados al momento.
ResultadosPeriodo de estudio, usando el LIRQ: Entre junio de 2011 y mayo de 2013. Se registraron un total de 4.255 cirugías y 11.907 procedimientos quirúrgicos. Por otro lado, cada residente registró 250 cirugías por año y 700 procedimientos quirúrgicos por año. La actividad quirúrgica como cirujano principal que se desarrolla el primer año de residencia es, principalmente, en cirugía urgente (68,01%) y por vía laparotómica (97,73%), mientras que durante el quinto año de residencia se desarrolla un 51,27% en cirugía programada y se utiliza la vía laparoscópica en un 23,10% de los casos. Durante este periodo, los residentes participaron en un total de 11 publicaciones científicas, 75 presentaciones en congresos y 69 actividades de formación continuada.
ConclusionesEl LIRQ es una herramienta útil que simplifica el registro y análisis de los datos sobre la actividad quirúrgica y científica de los residentes. Constituye un paso adelante en la evaluación de la formación de los residentes quirúrgicos, sin embargo, es solo un paso intermedio en el camino del desarrollo de un registro español de mayor envergadura.
The training programme of the General and Digestive Surgery speciality (2007)1 points out the importance of evaluating resident training. It proposes recording their activities during their residency so that compliance with the set objectives can be analysed and evaluated together with their tutor.
In 2004, the General and Digestive Surgery Department of the Hospital Universitario Parc Taulí (Sabadell) introduced the resident's electronic logbook (REL),2 which was subsequently adopted by the Spanish Association of Surgeons.3 This tool makes it possible to record the activities of training specialists, divided into periods, specialisation units, levels of responsibility and procedural complexity.
The REL was updated halfway through 2011, becoming the surgical resident's electronic logbook (SREL).4
The main aim of the new model is to simplify data recording, to make it possible to achieve a higher level of compliance and increase the reliability of the data recorded.
On the other hand, the SREL makes it possible to obtain a series of reports on scientific and educational surgical activity that may offer extremely valuable information to residents, to compare residents with others in the same hospital or in other centres, for correct monitoring by tutors and department heads, and even, if it comes into general use, it would be able to offer information on the actual situation of training at a national level.
Likewise and thanks to the SREL,4 residents will be able to prepare their curriculum vitae in a few seconds, and given that they are always tutored by a staff surgeon, they will be able to access teaching data for each member of the department with the same speed and efficacy.
The ease with which data can be entered and used with the SREL,4 and the resulting benefit for all of the members of the surgical department, will encourage and feed back into the correct use of the resident's book.
MethodsThe General and Digestive Surgical Department of the Hospital Universitario Parc Taulí (Sabadell) is currently training 10 surgery residents (Medicos internos residentes: MIR) (one MIR per year up to 2008 and 2 MIR per year since 2009).
From June 2011, the MIR record their activity prospectively in the SREL,4 which is a Microsoft Office® Access 2000 data base that is unique, specific and shared, and which is stored in the computer network of the hospital. The activity recorded in the old REL up to May 2011 was transcribed into the updated REL.
The SREL4 allows residents to record their training activities in 3 blocks: skills (surgery), scientific production and training (sessions, courses, seminars and congresses) (Fig. 1).

The record of surgical activity (Fig. 2) specifies whether it took place in emergencies or was scheduled. The surgical procedures carried out are recorded (e.g., right colon resection, intestinal anastomosis, laparotomy closure) rather than surgical operations (such as right laparotomic hemicolectomy), that is, the record of a surgical operation may contain several procedures.

On the other hand, the names of those taking part in each procedure are recorded, specifying the role played by each individual (surgeon, first or second assistant, observer) and year of training (MIR 1-MIR 5, junior assistant, senior assistant, consultant). The degree of complexity of the procedure,1 the level of responsibility of the participants1 and the code of the International Classification of Diseases, 9th Revision, Clinical Modification5 (ICD-9-CM), are assigned automatically.
Scientific activity (Fig. 2) is recorded by showing: the title of the work, date, type (communication, poster, video, research work, thesis, published paper) and the names of the participants, specifying their role in the work (main author or co-author) and year of training. In the case of publications, the name of the journal in which the work was published is shown.
The record of continuous training (Fig. 2) includes: the title of the activity, date, location, type (session, course, day, congress) and the names of the participants, specifying their role (audience, speaker, moderator, organising committee) and year of training.
On the other hand, the SREL4 makes it possible to access reports on recorded activities, updated in real time, individually (for each resident or surgeon in the department) or overall. As an example, we can access reports on surgical activity categorised according to: year of training, level of complexity and level of responsibility, periods of time, emergency or scheduled, laparoscopic or laparotomic. Likewise, it is possible to read detailed reports for each surgeon or the department as a whole, regarding scientific work or continuous training (Fig. 1).
Data entered in the SREL4 are regularly revised by tutors, the head of department and the Teaching Commission of the hospital. Every 6 months, in the general meetings of the department, a summary of the activity of residents is presented, individually and in comparison with their colleagues, with past records and the published aims in the programme of the speciality.1 This has the aim of identifying strong and weak points in the training process, motivating all members of the department and seeking possible solutions to problems.
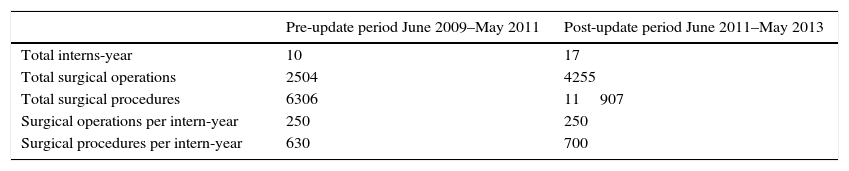
ResultsTable 1 shows a comparison between the period before the update (June 2009–May 2011) and after the update (June 2011–May 2013) of the resident's logbook, comparing the number of residents per year who entered records, the total number of surgical procedures recorded in each period and the average number of operations and surgical procedures recorded for each resident per year.
Surgical Operations and Procedures Recorded in the SREL.
| Pre-update period June 2009–May 2011 | Post-update period June 2011–May 2013 | |
|---|---|---|
| Total interns-year | 10 | 17 |
| Total surgical operations | 2504 | 4255 |
| Total surgical procedures | 6306 | 11907 |
| Surgical operations per intern-year | 250 | 250 |
| Surgical procedures per intern-year | 630 | 700 |
Fig. 3 shows the increasing level of responsibility accepted by residents in operations at different levels of complexity during their residency.

By updating the resident's logbook we are also able to evaluate the degree to which residents participate in emergency and planned surgery, as well as laparoscopic surgery, as is shown in Fig. 4.

Fig. 5 shows all of the scientific publications, congress presentations (as the main authors and co-authors) and continuous training activities in which residents took part in the period June 2011–May 2013 (the post-update period).
. R1/R2/R3/R4/R5 refer to residents in their first, second, third, fourth or fifth year, respectively.")
There is little literature in Spain about recording the activities of surgical residents. The General and Digestive Department of the Hospital Universitario Parc Taulí (Sabadell) has displayed a high level of interest in this field. It presented its first experience with the IEL2 in 2006, and 3 years later it published the report on its experience during the first 4 years,6 and recently (in 2012) it led a multicentre study on the use of the same.7
In Europe the Anglo-Saxon countries have the greatest experience with records of the activities of surgical residents.
The United Kingdom has a centralised electronic record in the website http://www.elogbook.org, and this is accessible for different surgical specialities (online and using mobile devices). It has been obligatory for residents since 2003, and is controlled by the Royal College of Surgeons of Edinburgh.8–10 Unlike the SREL, the eLogbook records complete operations rather than procedures, and this is considered to be a weak point by studies of the eLogbook. Nevertheless, it does record details of the level of participation (e.g., main surgeon, assistant and observer), whether an operation is planned or emergency, as well as academic activities (presentations, posters and research, etc.). The data recorded are used to generate individual and overall reports which are revised and assessed twice a year, in the same way as we do in our department. Currently more than 22,000 surgeons with different surgical specialities in the United Kingdom use the eLogbook, and more than 10 million operations are recorded in it.8–10
In 2011, Lonergan et al.8 undertook a descriptive study of experience with the use of the eLogbook in Ireland during the first 2 years of training of surgical residents, a work with similar characteristics to that of the Spanish multicentre study.7 It showed that in their first years residents’ surgical activity falls below the standards set by the Royal College of Surgeons of Ireland. This is chiefly because they take part in most surgical operations as assistants. This is not the case now in our department, as first and second year residents take part as surgeons in 65% and 40% of first and second degree complexity operations, respectively (Fig. 3).
On the other hand, in North America there are national records such as the ACS Case log System11 (also called the Practice-Based Learning System) or the ACS National Surgical Quality Improvement Programme (NSQIP)12 coordinated by the American College of Surgeons and accessible in Internet and through mobile devices. These records are more highly evolved and make it possible to practice result-based medicine. They are not restricted to recording the activities of residents, but rather all surgical activities before, during and after operations. These include basic demographic data, comorbidities, diagnoses, surgical procedures, complications and long-term results. Taking part in these records is useful as it prolongs certification by the American Board of Surgery, showing surgical experience, results and complications, identifying areas for improvement and applying corrective measures and then checking their efficacy.
In this context, we believe that the SREL4 represent an important improvement in recording the training activities of residents. Nevertheless, they are an intermediate step in the development of a broader Spanish registry like those in the United Kingdom and United States.
We believe that the improvements and advantages of the SREL4 in comparison with the previous intern's electronic logbook are:
- •
It is a unique and public data base, which any member of the department can use to enter data or consult.
- •
Surgical activities are divided into different procedures when they are added to the record (Fig. 2), making it more detailed, as can be seen in Table 1. Although the number of operations recorded per resident and year has not varied before and after updating, 70 surgical procedures more have been recorded for each resident and year after updating the logbook.
- •
It makes it possible to obtain updated, personalised or general reports automatically on surgical activity by all department members: residents and staff surgeons (Fig. 1).
- •
We are able to obtain an overview of the training of the residents in the department. i.e., we can see how residents take part in a higher percentage of more complex surgical procedures as each year of their training passes (Fig. 3). They also take part in a higher percentage of laparoscopic surgical operations (Fig. 4), while emergency and planned activities balance out at approximately 50% each by the end of residency (Fig. 4).
- •
On the other hand, scientific activity and continuous training are also shown in the SREL,4 and reports can be obtained (Fig. 5) which allow residents to obtain their updated curriculum vitae at any time, as well as to see the training and scientific work done by the department.
- •
Lastly, but very importantly, the subjective feeling of residents regarding use of the SREL is highly positive, as it is very intuitive and easy to work with: this is so for entering data, when individual information is used and above all when general data has to be used to prepare the half-yearly report on residents’ activities for the general meeting in the department.
In our opinion the weak points of the SREL4 are:
- •
Data are recorded voluntarily, so that the work of recording data must be accompanied by continuous feedback in favour of the residents to prevent their level of motivation from falling. It is here that tutors and the department head play an important role, at least until it becomes legally obligatory to use this electronic record, as is the case in the United Kingdom.8
- •
No method for verifying the authenticity of records is planned, even though this would be easy to do with audits, such as the one by individual tutors in the case of the British eLogbook.8
- •
The data bases are infinite (Table 1) and therefore there must be enough space on the hard disc when data are being entered, with continuous improvement and updating.
To conclude, SREL4 is a tool which simplifies the recording of residents’ activities while offering greater potential for data use. It is possible to obtain an infinite amount of information on resident training, from which all department members may benefit. Nevertheless, as we remarked at first, prior experience and that of other countries leads us to think that it would be highly useful to have a Spanish surgical record (online and accessible through mobile devices) for all hospitals with residents, with the aim of analysing the actual situation of surgical training in our country. Being able to access individual, hospital, autonomous community and national data would make it possible to set surgical standards for residents, implementing measures to adjust imbalances in training and setting standards to help new residents select a hospital for their training and helping them to design their CV when seeking a position as a specialist. It would be a support for the recertification of specialist qualifications and for multicentre studies at a national level, as well as for many other possibilities that we should not exclude.
Conflict of InterestsThe authors declare that they have no conflict of interests.
We would like to thank all of the residents and ex-residentss who took part: Constanza Corredera Cantarín, Heura Llaquet Bayo, Raúl Guerrero López, Anna Serracant Barrera, Meritxell Labró Ciurans, Noemí Montes Ortega, and Juan Carlos García Pacheco.
Please cite this article as: Gómez Díaz CJ, Luna Aufroy A, Rebasa Cladera P, Serra Pla S, Jurado Ruiz C, Mora López L, et al. Libro informático del residente de cirugía: Un paso adelante. Cir Esp. 2015;93:651–657.
