





To evaluate the long-term effectiveness of different therapies applied in the past 30 years, both medical and surgical, and results, with the ultimate aim of determining which are the most appropriate criteria to indicate when and how to perform medical and surgical treatment in these patients.
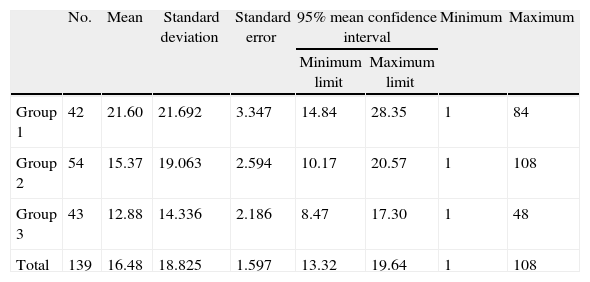
MethodA retrospective randomized study was conducted on 198 patients with primary divergent strabismus first seen in our clinic (IOC) in the last 36 years (1976–2012), with a mean follow-up of 8.38 years. Demographic and clinical characteristics, as well as the various treatments performed, and motor and sensory outcome were collected. They were finally divided into 3 groups of 70, 71 and 56 patients, respectively, according to their first visit, in order to compare the therapies applied.
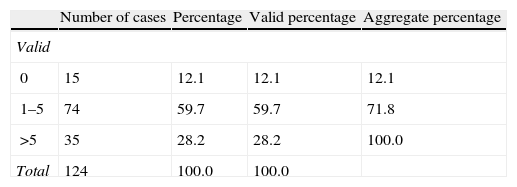
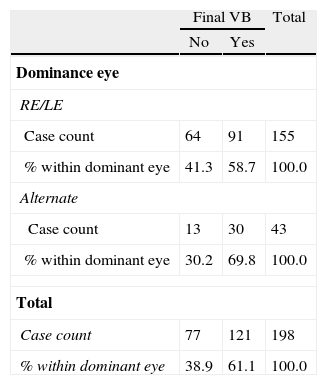
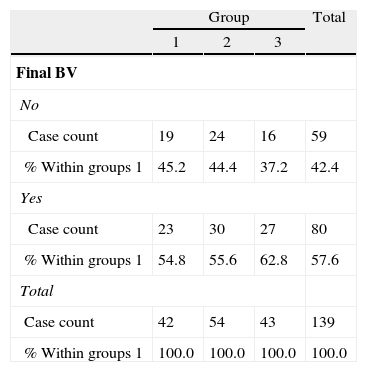
ResultsHalf (50%) of our patients debuted before 2 years of age (P50=24 months), and 26.3% had optimal binocular vision at the beginning of the study. Medical treatment was used as exclusive therapy in 29.3% of cases (occlusion therapy, applying negative lenses, botulinum toxin), and 70.7% required surgery (61.2% by double retro-insertion of lateral rectus, and 38.8% monolateral retro-resection). There was a recurrence in 26.7% of patients, and 40 re-interventions were performed (70% due to recurrence of divergent strabismus, 12.5% due to surgical over-correction, and 17.5% for other reasons). In the end, 61.1% of patients had perfect binocular vision (TNO=60″), and the proportion was higher in patients who showed proper control of their strabismus at the beginning (p=0.003). However, no differences were found in the other variables studied. When the patients were divided into 3 groups (which are demographically comparable), an increased number of patients in Group 3 were found to be treated using negative lenses and botulinum toxin (p<0.001 and p=0.003). This group was found to have had a higher proportion of bilateral surgery (p=0.032), seeking greater immediate postoperative over-correction, thus reducing the number of re-interventions from 40.5 to 19%, although it did not reach statistical significance (p=0.093). It was also found that there was a significantly increased number of injections of botulinum toxin in the middle rectum for treatment of excessive postoperative overcorrection (p=0.028). No other differences in final binocular vision were found between the 3 groups (p=0.703).
ConclusionsIn cases of clear ocular dominance, occlusion therapy must be applied twice daily on the dominating eye, in order to encourage divergent strabismus control and improve sensoriality. An attempt should be made to wait until patients reach four years of age before indicating surgical treatment, except in cases of a significant worsening of motor or sensory component. Bilateral surgery on both lateral rectus should be attempted, provided that patient characteristics allow this. A slight post-surgical overcorrection should be looked for in the immediate postoperative period, as this, in our experience, reduces the total amount of re-operations. When working on the middle rectus, remember that the elasticity of this muscle is the key factor for obtaining a proper post-surgical outcome, but a reliable measurement of this still cannot be made. In cases of excessive post-surgical over-correction, an injection of botulinum toxin should be applied to these poor elasticity muscles, in order to reduce the number of re-operations.
Evaluar a largo plazo la efectividad de las distintas terapias aplicadas en los últimos 30 años a estos pacientes, tanto médicas como quirúrgicas, y los resultados obtenidos, con el fin último de determinar qué criterios son los más adecuados a la hora de indicar y realizar tratamiento médico y quirúrgico sobre estos pacientes.
MétodoSe ha realizado un estudio retrospectivo aleatorizado de 198 pacientes con estrabismo divergente primario vistos por primera vez en nuestra consulta (IOC) en los últimos 36 años (1976-2012), con un seguimiento medio de 8,38 años. Se han recogido sus características demográficas y clínicas, así como los diversos tratamientos realizados y su resultado motor y sensorial. Por último, se han dividido en 3 grupos de 70, 71 y 56 pacientes respectivamente según la fecha en la que realizaron la primera consulta, para poder comparar las distintas terapias aplicadas.
ResultadosEn el 50% de nuestros pacientes empezó antes de los 2 años de edad (P50=24 meses). El 26,3% presentó una visión binocular óptima al inicio de la exploración. El tratamiento médico funcionó como medida exclusiva en el 29,3% de los casos (oclusiones horarias, aplicación de lentes negativas, toxina botulínica), y un 70,7% precisaron cirugía (61,2% mediante doble retroinserción de rectos laterales y 38,8% de retrorresecciones monolaterales). El 26,7% de los pacientes experimentaron recidivas, con 40 reintervenciones (70% por recidiva del estrabismo divergente, 12,5% por hipercorrección quirúrgica excesiva y el 17,5% por otras causas). Al final del seguimiento, el 61,1% de los pacientes presentaban una visión binocular perfecta (TNO=60″), cuya proporción fue mayor en pacientes en ortotropía espontánea antes de disociarles (p=0,003), pero sin diferencias en otras variables estudiadas. Al estudiar a los pacientes divididos en 3 grupos, que son demográficamente comparables entre sí, se ha visto mayor utilización de toxina y lentes negativas en el grupo 3 (p<0,001 y p=0,003). Se ha intervenido a los pacientes más frecuentemente con cirugía bilateral en el tercer grupo (p=0,032), buscando una mayor hipercorrección en el postoperatorio inmediato, logrando así disminuir el número de reintervenciones del 40,5 al 19%, aunque no pudo demostrarse su significación estadística (p=0,093). También aumentó significativamente el número de inyecciones de toxina botulínica en el recto medio como tratamiento de la hipercorrección posquirúrgica excesiva (p=0,028). No hemos encontrado diferencias en la visión binocular final entre los 3 grupos (p=0,703).
ConclusionesEn casos de dominancia ocular clara debemos aplicar oclusión horaria 2 veces al día sobre el ojo dominado para fomentar el control del estrabismo divergente y así obtener un mejor resultado desde el punto de vista sensorial. Procuraremos esperar a los 4 años para intervenir quirúrgicamente, salvo en los casos en los que detectemos un empeoramiento significativo del componente sensorial o motor. A la hora de operar, y siempre que las características del paciente lo permitan, intentaremos realizar cirugía bilateral sobre ambos rectos laterales, buscando una ligera hipercorrección posquirúrgica en el postoperatorio inmediato, ya que en estos pacientes hemos disminuido el número total de reintervenciones. A la hora de actuar sobre un recto medio, conviene recordar que la elasticidad del mismo parece ser el factor clave para el resultado posquirúrgico, aunque por el momento no nos sea posible medirlo de forma fiable. La aplicación de toxina botulínica sobre rectos medios poco elásticos en caso de excesiva corrección posquirúrgica nos ha permitido disminuir el número de reintervenciones.
