

The present study aimed to analyze the stability of the memory of a stressful event (medical examination within a hospital setting) over time in young people (age range 12 to 21, Mage = 15.11 years old, SD = 3.047) with mild or moderate intellectual disability (IQ = 54.32, SD = 13.47). The results show a stability of the memory of what happened an hour and a week after the event in relation to the people involved, the apparatus used, and the parts of the body explored. No interaction effects were found between the stability of memory over time and the level of intellectual disability. The level of disability (mild or moderate) only affected the description of the doctor who performed the exploration and the explored parts of the body, showing better results for people with mild disability. In addition, the results highlight the relationship between memory and IQ, especially verbal IQ.
En el presente trabajo se analiza la estabilidad a lo largo del tiempo de la memoria sobre un acontecimiento estresante (exploración médica en el ámbito hospitalario) en jóvenes (rango de edad 12 a 21, Medad = 15.11 años, DT = 3.047) con discapacidad intelectual leve y moderada (CI = 54.32, DT = 13.47). Los resultados muestran la estabilidad del recuerdo de lo sucedido a la hora y a la semana de la exploración respecto al recuerdo de personas, la instrumentación y las partes del cuerpo exploradas. No se encontraron efectos de interacción entre la estabilidad del recuerdo a lo largo del tiempo y el nivel de discapacidad intelectual. El nivel de discapacidad (leve o moderado) sólo afectó a la descripción de la doctora que hizo la exploración y a las partes del cuerpo exploradas, siendo mejor en las personas con discapacidad leve. Además, los resultados ponen de manifiesto la relación entre el recuerdo y el CI, especialmente verbal.
There is a great deal of stereotyping regarding the memory abilities of people with intellectual disability (ID), partly due to the social representation of the person with intellectual disability and the scarcity of well-controlled studies on this subject (Henry, Ridley, Perry, & Crane, 2011; Kebbell & Hatton, 1999; Manzanero, Alemany, Recio, Vallet, & Aróztegui, 2015; Manzanero, Quintana, & Contreras, 2015; Peled, Iarocci, & Connolly, 2004; Sobsey & Doe, 1991; Spellman & Tenney, 2010; Stobbs & Kebbell, 2003; Tharinger, Horton, & Millea, 1990; Valenti-Hein & Schwartz, 1993). In fact, quite often, the testimonies of people with ID are not believed, probably due to these different stereotypes. This lack of credibility increases their vulnerability and limits their participation in the justice system, which could explain the few police reports in which these collectives appear as victims, despite being more likely to become victims of crimes than people who do not present any ID (González, Cendra, & Manzanero, 2013). When society is confronted with the task of comparing testimonies of people without disabilities and people with ID, differences are not perceived until the intellectual ability of each group is known. However, when testimonies are compared knowing the intellectual ability of the victims, society determines that people with ID are less credible (Peled et al., 2004). Moreover, people with ID are often not believed within judicial settings, even when those who assess their statement are experts in crime investigation (Manzanero, Quintana et al., 2015). There are no specific protocols adapted to the characteristics of this collective (Manzanero, Alemany et al., 2015), in spite of the fact that any procedure that evaluates testimonies should always take into account the specific abilities of the victims (Köhnken, Manzanero, & Scott, 2015; Manzanero & González, 2015). When memory has been assessed through interviews with children who have been separated into groups according to the severity of their intellectual disability, including children with normal development, no significant differences have been observed in the recall of details of the events (Bettenay, Ridley, Henry, & Crane, 2014). Therefore, a specific assessment of the ability to testify is required (Contreras, Silva, & Manzanero, 2015; Silva, Manzanero, & Contreras, 2016), with the main objective of adapting the testimony assessment protocols.
It is possible that this situation of discrimination is influenced by certain circumstances that are detailed below. Firstly, the overgeneralization of cognitive deficits to all people with ID, based on a lack of knowledge of their true abilities, would be the main erroneous stereotype that explains this reality. Although the variability among collectives of people with ID is high, some people with intellectual limitations may present difficulties in certain psychological processes such as language, comprehension, generalization of concepts, or slower processing in general. However, the severity of the difficulties will depend on the degree of impairment of the intellectual performance and whether adequate supports are in place (Manzanero, Contreras, Recio, Alemany, & Martorell, 2012; González, Muñoz, Sotoca, & Manzanero, 2013).
In relation to the support they need, some studies show that children with ID have a lower performance than their chronological age peers with typical development when giving testimony (Michel, Gordon, Ornstein, & Simpson, 2000). However, other studies show that people with ID can give accurate testimonies, provided they are not asked closed-ended, complex questions, and the appropriate adaptations are in place (Darwinkel, Powell, & Sharman, 2014; Kebbell & Hatton, 1999; Mattison, Dando, & Ormerod, 2015). Thus, the errors would not be associated with the disability itself, but with the way the interrogation is carried out.
Secondly, it is observed that people with ID often develop feelings of insecurity and frustration (García Eligio de La Puente & Arias Beatón, 2007) that manifest themselves in all aspects of their lives. These feelings are especially observed when these individuals feel evaluated, as often intellectual disability is expressed as school failure, which is a usual field of assessment. In establishing this relationship of failure when being evaluated, this collective appears insecure in their answers and the slightest suggestion can cause them to change their answers in an interrogation. Faced with the dilemma of conveying what they believe, as opposed to what they consider to be “correct” according to what the evaluator expects, it is likely that they will distrust their own judgment. For this reason, specific interview procedures have been developed for this collective and for other especially vulnerable individuals, such as children, people with mental illnesses, or elderly people (Lamb, Orbach, Hershkowitz, Esplin, & Horowitz, 2007; Manzanero, Recio, Alemany, & Cendra, 2013; Muñoz et al., 2016), with the objective of minimizing this problem.
Thirdly, it should be noted that the ID label itself can lead to imprecise conclusions. A ID is only the end result of multiple deficient processes of neurodevelopment, each of which may have its own cognitive pattern. Therefore, the ability to reproduce a lived event is different depending on the origin of the disability (Brock & Jarrold, 2005; Edgin, Pennington, & Mervis, 2010; Jarrold, Baddeley, & Hewes, 1999) and on the type of cognitive process being evaluated, whether it is working memory, perception or long-term memory (Bartlet, Ansari, Vaessen, & Blomert, 2014). For example, ironically, some types of ID, such as Williams Syndrome, entail a demonstrated ability to recognize faces, a fundamental process in eyewitness testimony. Thus, it has been observed that people with Williams Syndrome have an enlarged fusiform face area compared to people with typical development, which may explain their efficiency in this task (Golarai et al., 2010). However, on the other hand, there are difficulties in facial recognition in disabilities such as Fragile X Syndrome, influenced by dysfunctions in the prefrontal neural networks of social cognition (Holsen, Dalton, Johnstone, & Davidson, 2008). For this reason, it is advisable to take into account the characteristics of the pathology that causes the intellectual disability (Manzanero et al., 2013) and the associated specific cognitive deficits. In any case, over-generalizations should always be avoided and the specific deficits of each person should be individually assessed (Contreras et al., 2015).
Finally, it should be noted that the evaluation of memory ability among these collectives is carried out with non-specific tests that involve acontextual and sometimes meaningless materials. Thus, it is not possible to extrapolate the results of recall tasks and recognition of lists of words or digits to the memory of complex, meaningful, and emotional facts. A poor performance in the first type of tasks does not necessarily imply an identical performance in the latter. Memory is fundamentally emotional and the meaning of events plays a very important role in the processes of coding, retention, and retrieval (LaBar & Cabeza, 2006). Perhaps, this problem is much greater in the case of people with ID, explaining why the memory of complex and emotional facts does not present as many deficits as we might expect for their intellectual characteristics. In any case, the memory ability may not be the same for all types of information or over time, thus warranting further study in this aspect, overcoming the lack of experimental data in this regard. Studies carried out with children (Baker-Ward, Gordon, Ornstein, Larus, & Clubb, 1993; Ornstein, Baker-Ward, Gordon, & Merritt, 1997) show that their recollection of complex facts (e.g., a pediatric exploration), would yield differences according to the information provided on the actions that took place and the description of the persons involved, with only slight differences across short intervals of time. The objective of the present work is to study how the memory of a complex and emotional event behaves in young people with ID across time and the effect that the degree of disability would have, according to the level of efficiency in concrete cognitive abilities of intelligence, both verbal and performance IQ. Considering the results of the aforementioned research, the present study expects to find differences according to the type of information being recalled, as well as over time and according to the intellectual disability.
MethodParticipantsThe study involved 27 individuals with an intellectual disability disorder of unspecified etiology, 12 women and 15 men. The mean age was 15.11 years (SD = 3.047, range = 12-17). The mean IQ was 54.32 (SD = 13.472), the mean verbal IQ was 55.14 (SD = 11.41) and the mean performance IQ was 62.40 (SD = 17.77). Fifteen participants had a moderate intellectual disability (total IQ between 35-55, MIQ = 44.26, SD = 4.30) and 12 participants had a mild intellectual disability (total IQ between 55-70, MIQ = 67.66, SD = 9.04). In all cases, the parents/guardians signed an informed consent form with the consent of the participants.
InstrumentsSpanish version of Weschler Intelligence Scale for Children, WISC-R (Weschler, 1981), or WAIS-III (Weschler, 1997), according to the age of the participant.
Both tests aim to explore the cognitive abilities and evaluate intelligence, offering an IQ score, using different tests that explore both verbal and performance aspects. Their application time is around 60-90minutes.
ProcedureEach participant was exposed to a medical examination within a hospital setting. This is a type of event used (see, for example, Baker-Ward et al., 1993; Bruck, Ceci, Francouer, & Renick, 1995; Ornstein et al., 1997; Pezdek et al., 2004; Quas et al., 1999) as an event comparable to sexual abuse due to its negative emotional connotations and having actions in common (undressing and being touched by another person). This experimental situation entails an exposure to a stress-generating event within the ethical standards of this type of research. Furthermore, it is a standardized situation, thus the results obtained by each participant depend on the characteristics of such participant and not on variations of the situation. Therefore, as this event serves as a golden rule of comparison, not only the memory of what happened can be explored, but it can also be compared with the cognitive characteristics of each case.
The exploration was carried out in a doctor's surgery within a health institution in Havana, Cuba. The person responsible for the examination was a doctor specialized in Neurology. During the examination, the mother or guardian responsible for the participant was present.
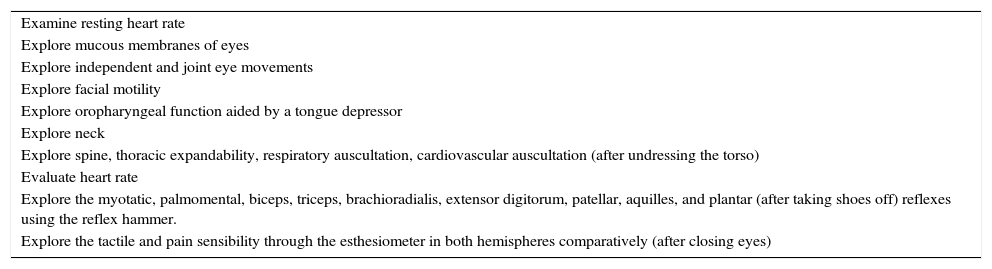
A protocol (see Table 1) was designed for the medical examination, which indicated the order of application of each test and the procedure. In addition, the instructions for each of the tests were indicated in a standardized way.
Medical Examination Protocol.
| Examine resting heart rate |
| Explore mucous membranes of eyes |
| Explore independent and joint eye movements |
| Explore facial motility |
| Explore oropharyngeal function aided by a tongue depressor |
| Explore neck |
| Explore spine, thoracic expandability, respiratory auscultation, cardiovascular auscultation (after undressing the torso) |
| Evaluate heart rate |
| Explore the myotatic, palmomental, biceps, triceps, brachioradialis, extensor digitorum, patellar, aquilles, and plantar (after taking shoes off) reflexes using the reflex hammer. |
| Explore the tactile and pain sensibility through the esthesiometer in both hemispheres comparatively (after closing eyes) |
An interview was carried out an hour and a week after the medical examination, which was composed of 19 questions that assessed memory of people, memory of actions, memory of objects, identifying the source, touch and feelings. The interviews were carried out by a psychologist trained for this purpose.
ResultsMemory Ability as a Function of TimeFirstly, the memory ability for each type of information an hour and a week after the event was analyzed.
Recalling people. The analysis of the participants’ answers to the questions related to the memory of the doctor who performed the medical examination shows that after an hour only 3 participants (11.11%) were able to remember the doctor's name, increasing to 6 participants (22.22%) at the interview performed one week later, without yielding any significant difference between them, χ2(1, N = 54) = 1.200, p > .05. Furthermore, no differences were found in the description of the doctor over time, where an average of 2.29 correct traits (SD = 1.18) were recalled after an hour and 2.37 (SD = 1.39) were recalled after a week had elapsed, t(26) = -.451, p > .05, Cohen's d = 0.062.
The only significant difference found was in the participants’ recall of how the doctor was dressed. The mean of correctly described garments was 2.07 (SD = 1.36) after an hour had elapsed and 1.52 (SD = 1.22) after a week had elapsed, t(26) = 2.500, p < .05, Cohen's d = 0.425.
Recalling actions. Memory of actions and procedures was not affected by time in any of the questions raised. In general, the percentage of correct answers was very high. After an hour had elapsed, 13 participants (48.14%) correctly answered the question of where they had been touched first. After a week had elapsed, the same number of participants answered the question correctly, although 4 participants that had recalled correctly at the 1-hour interview forgot where they had been touched first at the 1-week interview and 4 new participants remembered correctly at the 1-week interview and not at the 1-hour interview. At the 1-hour interview, 26 participants (96.29%) responded correctly to the question of whether they had been instructed to stand up, in comparison to the 25 participants (92.59%) that responded correctly at the 1-week interview, χ2(1, N = 54) = 0.353, p > .05. Regarding the question of what happened next, 22 participants (81.48%) answered correctly at the 1-hour interview, compared to the 18 participants (66.66%) that correctly answered at the 1-week interview, χ2(1, N = 54) = 1.543, p > .05. In relation to the question about what they had done with their clothes, 20 participants (74.07%) answered correctly at the 1-hour interview and 19 participants (70.37%) at the 1-week interview, χ2(1, N = 54) = 0.092, p > .05. All participants (100%) correctly answered the question of whether they had been ordered to remove their shoes, in both interviews. Finally, to the question of what the doctor had done with each apparatus, at the 1-hour interview, the participants correctly remembered 2.11 (SD = 0.943) actions, and recalled a similar number of actions (M = 2.07, DT = 0.99) at the 1-week interview, t(26) = .196, p > .05, Cohen's d = 0.041.
Recalling objects. No differences were found for the recall and description of the objects used in the exploration as a function of time. All participants (100%) recalled that apparatus were used. At the 1-hour interview, a mean of 2.15 (SD = 1.08) objects were correctly described, in comparison to the 1.96 (SD = 1.02) objects recalled at the 1-week interview, t(26) = .961, p > .05, Cohen's d = 0.180.
Identifying roles. The participants’ ability to discriminate whether the doctor had performed various actions or they had perfomed these actions themselves was assessed. To the question of whether it was the doctor or the participant who had arranged the clothes, 17 participants (62.96%) answered correctly at the 1-hour interview, compared to the 15 participants (55.55%) that answered correctly at the 1-week interview, χ2(1, N = 54) = 0.307, p > .05. When asked who took off their shoes, 26 participants (96.29%) answered correctly at the 1-hour interview and 23 participants (85.18%) at the 1-week interview, χ2(1, N = 54) = 1.984, p > .05.
Touching. No significant differences were found over time regarding the parts of the body that had been explored, yielding mean scores of correctly identified body parts of 5.07 (SD = 1.75) at the 1-hour interview and of 4.48 (SD = 1.22) at the 1-week interview, t(26) = 1.897, p > .05, Cohen's d = 0.391, with 10 being the total number of body parts explored. To the specific question about whether their mouths had been examined, 26 participants (96.29%) answered correctly at the 1-hour interview and 25 participants (92.59%) at the 1-week interview, χ2(1, N = 54) = 0.353, p > .05. On the other hand, to the question of whether their clothes had been touched, significantly 24 participants (88.88%) answered affirmatively at the 1-hour interview in comparison to only 18 particpants (66.66%) at the 1-week interview, χ2(1, N = 54) = 3.857, p < .05; Ф = 0.267, p < .05.
Feelings. In general, the associated feelings were negative and stable over time. At the 1-hour interview, 19 participants (70.37%) indicated they had felt upset, compared to the 23 participants (85.18%) that stated the same at the 1-week interview, χ2(1, N = 54) = 1.714, p > .05. Twenty-five participants (92.59%) indicated having felt uncomfortable at the 1-hour interview, with 23 participants (85.18%) stating the same discomfort at the 1-week interview, χ2(1, N = 54) = 0.750, p > .05. At the 1-hour interview, 23 participants (85.18%) reported having felt fear in comparison to the 24 participants (88.88%) reporting fear at the 1-week interview, χ2(1, N = 54) = 0.164, p > .05.
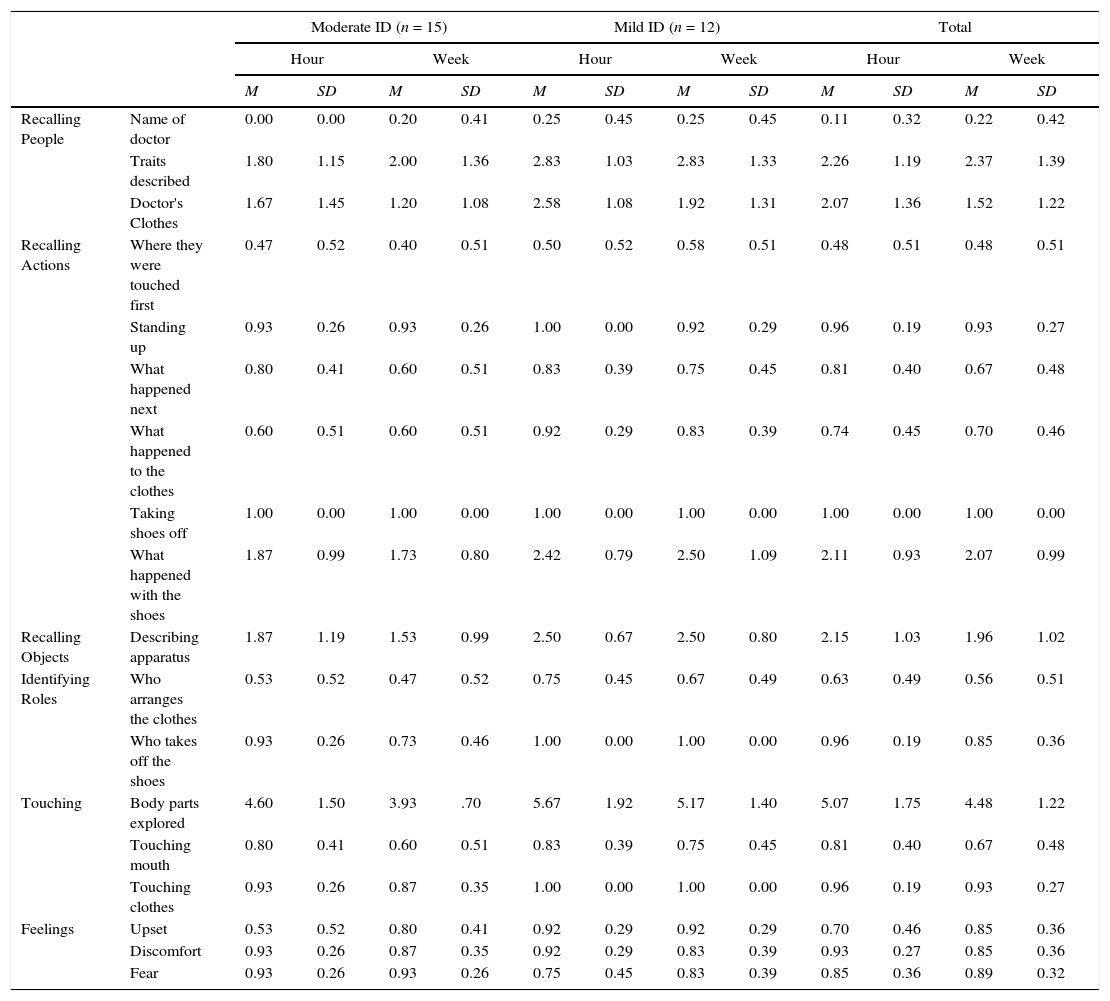
Relationship between IQ and MemoryRegarding the effects of the level of intellectual disability on memory ability, the analyses took into account whether the participants suffered from moderate or mild disability. The results showed that there was no interaction effect between level of disability and time elapsed (see Table 2). With regard to the main effects of the level of disability, significant effects were only found regarding the number of traits described correctly with respect to the doctor, F(1, 25) = 5.325, p < .05, η2 = .18; and the number of body parts explored, F(1, 25) = 6.609, p < .05, η2 = .21. Young people with moderate disabilities recalled significantly fewer traits regarding the doctor's description and correctly noted fewer explored body parts than young people with mild disabilities.
Mean Scores and Standard Deviations for the Analyzed Dimensions according to the Level of Intellectual Disability.
| Moderate ID (n = 15) | Mild ID (n = 12) | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hour | Week | Hour | Week | Hour | Week | ||||||||
| M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | ||
| Recalling People | Name of doctor | 0.00 | 0.00 | 0.20 | 0.41 | 0.25 | 0.45 | 0.25 | 0.45 | 0.11 | 0.32 | 0.22 | 0.42 |
| Traits described | 1.80 | 1.15 | 2.00 | 1.36 | 2.83 | 1.03 | 2.83 | 1.33 | 2.26 | 1.19 | 2.37 | 1.39 | |
| Doctor's Clothes | 1.67 | 1.45 | 1.20 | 1.08 | 2.58 | 1.08 | 1.92 | 1.31 | 2.07 | 1.36 | 1.52 | 1.22 | |
| Recalling Actions | Where they were touched first | 0.47 | 0.52 | 0.40 | 0.51 | 0.50 | 0.52 | 0.58 | 0.51 | 0.48 | 0.51 | 0.48 | 0.51 |
| Standing up | 0.93 | 0.26 | 0.93 | 0.26 | 1.00 | 0.00 | 0.92 | 0.29 | 0.96 | 0.19 | 0.93 | 0.27 | |
| What happened next | 0.80 | 0.41 | 0.60 | 0.51 | 0.83 | 0.39 | 0.75 | 0.45 | 0.81 | 0.40 | 0.67 | 0.48 | |
| What happened to the clothes | 0.60 | 0.51 | 0.60 | 0.51 | 0.92 | 0.29 | 0.83 | 0.39 | 0.74 | 0.45 | 0.70 | 0.46 | |
| Taking shoes off | 1.00 | 0.00 | 1.00 | 0.00 | 1.00 | 0.00 | 1.00 | 0.00 | 1.00 | 0.00 | 1.00 | 0.00 | |
| What happened with the shoes | 1.87 | 0.99 | 1.73 | 0.80 | 2.42 | 0.79 | 2.50 | 1.09 | 2.11 | 0.93 | 2.07 | 0.99 | |
| Recalling Objects | Describing apparatus | 1.87 | 1.19 | 1.53 | 0.99 | 2.50 | 0.67 | 2.50 | 0.80 | 2.15 | 1.03 | 1.96 | 1.02 |
| Identifying Roles | Who arranges the clothes | 0.53 | 0.52 | 0.47 | 0.52 | 0.75 | 0.45 | 0.67 | 0.49 | 0.63 | 0.49 | 0.56 | 0.51 |
| Who takes off the shoes | 0.93 | 0.26 | 0.73 | 0.46 | 1.00 | 0.00 | 1.00 | 0.00 | 0.96 | 0.19 | 0.85 | 0.36 | |
| Touching | Body parts explored | 4.60 | 1.50 | 3.93 | .70 | 5.67 | 1.92 | 5.17 | 1.40 | 5.07 | 1.75 | 4.48 | 1.22 |
| Touching mouth | 0.80 | 0.41 | 0.60 | 0.51 | 0.83 | 0.39 | 0.75 | 0.45 | 0.81 | 0.40 | 0.67 | 0.48 | |
| Touching clothes | 0.93 | 0.26 | 0.87 | 0.35 | 1.00 | 0.00 | 1.00 | 0.00 | 0.96 | 0.19 | 0.93 | 0.27 | |
| Feelings | Upset | 0.53 | 0.52 | 0.80 | 0.41 | 0.92 | 0.29 | 0.92 | 0.29 | 0.70 | 0.46 | 0.85 | 0.36 |
| Discomfort | 0.93 | 0.26 | 0.87 | 0.35 | 0.92 | 0.29 | 0.83 | 0.39 | 0.93 | 0.27 | 0.85 | 0.36 | |
| Fear | 0.93 | 0.26 | 0.93 | 0.26 | 0.75 | 0.45 | 0.83 | 0.39 | 0.85 | 0.36 | 0.89 | 0.32 | |
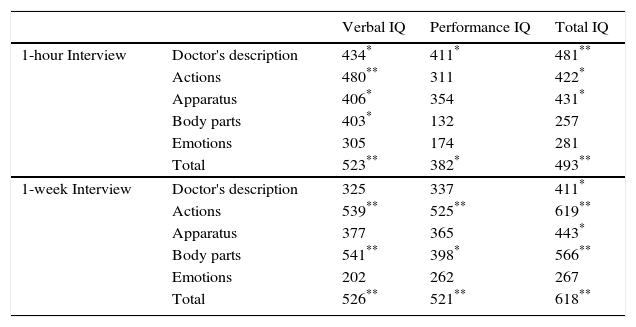
The analysis performed to determine the correlation between the memory index and IQ (see Table 3) revealed that the total IQ correlated significantly with the ability to describe the doctor that performed the exploration, the actions that took place, the apparatus used, and the total contribution of information, both at the 1-hour and the 1-week interviews. However, verbal IQ was significantly related to the ability to describe the doctor and the apparatus used only at the 1-hour interview. The parts of the body explored, the actions that took place, and the total information contributed correlated significantly with verbal IQ at both the 1-hour and the 1-week interviews. Finally, spatial IQ correlated with the ability to describe the doctor at the 1-hour interview; with the actions and the body parts explored at the 1-week interview; and with the total information contributed at both the 1-hour and the 1-week interviews. In all cases, the correlations were positive, thereby the higher the IQ, the greater the amount of accurate information provided.
Correlations (Pearson, bilateral) between Total, Verbal, and Performance IQ Scores and the Different Types of Information Recalled at the 1-Hour and the 1-Week Interviews.
| Verbal IQ | Performance IQ | Total IQ | ||
|---|---|---|---|---|
| 1-hour Interview | Doctor's description | 434* | 411* | 481** |
| Actions | 480** | 311 | 422* | |
| Apparatus | 406* | 354 | 431* | |
| Body parts | 403* | 132 | 257 | |
| Emotions | 305 | 174 | 281 | |
| Total | 523** | 382* | 493** | |
| 1-week Interview | Doctor's description | 325 | 337 | 411* |
| Actions | 539** | 525** | 619** | |
| Apparatus | 377 | 365 | 443* | |
| Body parts | 541** | 398* | 566** | |
| Emotions | 202 | 262 | 267 | |
| Total | 526** | 521** | 618** |
The emotions associated with the medical examination did not yield any correlation with either the total, verbal, or performance IQ.
Finally, no significant relationships were found between the different IQ scores and the age of the participants. That is, older people did not score more on total, performance, or verbal IQ.
DiscussionIn the present experiment with young people with mild and moderate intellectual disability, it was observed that time modifies their autobiographical memory of complex events in a heterogeneous way. The memories of the people involved, the apparatus used, and the parts of the body explored were maintained after a week had elapsed. However, time affected recalling of actions, the sequence, and the order of procedures. Although the information encoding processes regarding faces, body parts, and objects do not occur in the same way, and are even processed in different regions of the brain, in the present study their recall is similar in relation to the time elapsed between the event and the recovery task.
Thus, an applied aspect of this result is the fact that testimony should not be analyzed uniformly, in general. Inconsistencies may appear in certain contents, especially regarding the sequence of actions or procedures, as they are more sensitive to the effect of time. However, these inconsistencies do not entail that every testimony must be considered alike, as other contents of memory may remain stable despite the temporal distance between the event and the testimony.
On the other hand, IQ was found to be significantly related to the effectiveness of the testimony depending on the total recall and, specifically on the variables analyzed. The verbal IQ significantly correlated with memory in general, that is, the higher the verbal IQ, the better the recall, which is to be expected, as verbal skills influence the ability to produce a story and describe facts, objects, or people. However, this relationship is maintained after one week only for actions and body parts. The relationship between verbal IQ and the ability to describe people and objects, as well as with emotions, disappears one week after the event, in the same direction as the results found in other studies where IQ was found to be related to the ability to identify individuals (Manzanero, Recio, Alemany, & Martorell, 2011). The WAIS/WISC verbal scale evaluates aspects such as comprehension, vocabulary and arithmetic, and schooling may also become a factor when dealing with people with intellectual disabilities. However, this variable is ruled out in the present study's sample, as all participants were educated from an early age (approximately 5 years of age), in the same school where specialized care is provided.
In the case of performance IQ, it is also significantly related to overall memory at the 1-hour and the 1-week interviews. Depending on the type of information being recalled, the performance IQ after 1 hour had elapsed was only significantly related to the description of people and overall memory. After one week had elapsed, the relationship between performance IQ and memory mimics what happens with verbal IQ, that is, it is only significantly related to body parts and to actions.
The doctor's description and the memory of the actions or procedures are more sensitive to the effect of time according to IQ, both verbal and performance. This is important because these two aspects are usually evaluated in the testimonies and are related to the IQ at both the 1-hour and 1-week interviews.
The feelings or emotions associated with the event are stable over time at the 1-hour and 1-week interviews, with no significant relationship with IQ. Emotion is known to function as a memory modulator, which in this case minimizes the deterioration of memory over time. In the present study, an event that promoted negative emotions was used, within the ethical limits, which does not entail a highly emotional situation. Despite this fact, more than 70% of the participants expressed having felt fear, upset, and discomfort during the examination. Emotion has a powerful influence on learning and memory, as it compromises brain systems in different states of information processing. Emotional declarative memory studies show how frontotemporal regions of the brain act together to promote the retention of emotional events and to retrieve them from long-term memory storage (Manzanero & Álvarez, 2015).
ConclusionsThe Intelligence Quotient is an important factor to consider when predicting performance in a memory task regarding a complex event with a negative valence, such as a medical examination. In general terms, it can be concluded that the greater the ability, the better the performance when recalling people, objects, and especially actions. Moreover, the lower the ability, the more negatively time affects memory, yielding a more significant relationship between memory and IQ after one week has elapsed than immediately after the event has taken place, regardless of the specific level of disability in which the subjects are framed (mild or moderate). The only type of information that is free from the influence of time and intellectual ability is emotional information. In this way, it can be observed that emotions remain stable over time.
If the event in question had been an episode of sexual abuse instead of a medical examination, it should be taken into account that it is precisely the memory of the event that defines the abuse and its criminal nature, that could be compromised. Although it is true that the present study provides evidence in relation to aspects poorly studied in populations with ID, it would be advisable to further delve in these aspects with studies that expand the limited sample of the present research and can replicate the information found in relation to the stability of memory and the emotions associated with it.
Conflict of InterestThe authors of this article declare no conflict of interest.
This work is part of a research project on assessment of memories and psychological disorders associated to trauma, developed by UCM Research Group on Eyewitness Testimony (ref. 971672), in the framework of the project financed by Santander-Universidad Complutense de Madrid (PR26/16-20330).
