


The purpose of this study is to evaluate whether conformity with a traditional female role is related to the presence of anxiety symptoms in a sample of women (N = 234). To do so, symptoms of anxiety were evaluated through the Inventory of Situations and Responses of Anxiety (ISRA; Miguel-Tobal, & Cano-Vindel, 2002) and compliance with feminine gender roles was measured through the Inventory of Conformity to Feminine Norms (CFNI; Mahalik et al., 2005). Our results showed that higher levels of Cognitive Anxiety in women are related to higher compliance with the Thinness, Sexual Fidelity and Investment in Appearance dimensions of the CFNI. Also, a significant relationship was found between Total Anxiety and the Thinness dimension of the CFNI. These results suggest that some variables related to gender are related to anxiety responses, and that this relationship could occur through different interactions among cognitive variables.
El propósito de este estudio es evaluar si la conformidad con los roles femeninos tradicionales se relaciona con la presencia de síntomas de ansiedad en una muestra de mujeres (N = 234). Para ello, se evaluaron los síntomas de ansiedad a través del Inventario de Situaciones y Respuestas de Ansiedad (ISRA; Miguel-Tobal, & Cano-Vindel, 2002) y la aceptación de las normas de género femeninas se midió mediante el Inventario de Conformidad con las Normas de Género Femeninas (CFNI; Mahalik et al., 2005). Nuestros resultados mostraron que los niveles más altos de Ansiedad Cognitiva en las mujeres se relacionan con una mayor conformidad en las dimensiones de Delgadez, Fidelidad Sexual e Inversión en Apariencia del CFNI. Además, se encontró una relación significativa entre la Ansiedad Total y la dimensión de Delgadez del CFNI. Estos resultados sugieren que algunas variables relacionadas con el género están relacionadas con las respuestas de ansiedad, y que esta relación podría ocurrir a través de diferentes interacciones entre las variables cognitivas.
Universidad Complutense de Madrid
Influence of Feminine Gender Norms in Symptoms of Anxiety in the Spanish ContextGender differences in terms of prevalence and frequency of anxiety symptoms are considerable, and it has led to consider the female sex as a risk factor for developing anxiety symptoms (Alonso & Lepine, 2007; Valls-Llobet, Ojuel-Solsona, López-Carrillo, & Fuentes-Pujol, 2007). International epidemiological studies consistently show a higher prevalence of anxiety disorders in women, primarily in Western and industrialized countries. The European World Mental Health Surveys confirm this trend, showing that in seven out of ten European countries, women exhibit higher rates of anxiety symptoms compared to men. Among the countries studied, only Belgium, Germany and Romania did not follow the trend. The prevalence of anxiety disorders in Spain among women older than 16 is 19,1%, whereas in men this percentage is 8,1% (Rocha, Pérez Rodríguez-Sanz, Borrell, & Obiols, 2010; Ministry of Health & Social Policy, 2010).
In this study, anxiety is defined as an adaptive and complex emotional response that emerges from the interaction of individual factors and specific situations that appears when a threat or potential danger is perceived. The manifestation of anxiety is operationalized according to the three-dimensional theory of emotions, which consists in three response systems: cognitive-subjective, physiological, and motor or expressive. This understanding of anxiety has been widely accepted in areas of both empirical and theoretical research due to the implications for assessment and therapeutic intervention (Monteagudo, Saura, Cano-Vindel, & García-Fernández, 2012). In fact, anxiety symptoms are a central aspect of psychopathology because of their association with a wide variety of mental, psychophysiological, behavioral, and emotional disorders (Aldao & Nolen-Hoeksema, 2010; Cano-Vindel, 2011; Ramos, Piqueras, Martínez, & Oblitas, 2009). In addition, epidemiological studies systematically show different prevalence rates of specific mental disorders across genders, such as anxiety, which women are more like to suffer than men (e.g. Eaton et al., 2012; McLean, Asnaani, Litz, & Hoffman, 2011; Rodriguez del Toro, 2009).
The differences found between men and women in self-reported measures of physical and psychological symptoms of anxiety can be due to biological aspects linked to sex, as well as by gender differences (Diest, De Pauter, Eertmans, Bogaerts, Victoir, & Van den Bergh, 2005). Researchers have proposed several biomedical, epidemiological, socio-environmental, artefactual, and psychological mechanisms to explain these stark differences (Matud, Diaz, Aguilera, Rodriguez, & Matud, 2003; Montero et al., 2004). For instance, the biological approach states that differences in body morphology and hormonal functioning could explain some important differences in physiological responses to stress (Taylor, Klein, Lewis, Gruenewald, Gurung, & Updegraff, 2000), as well as differences in psychological variables relevant to the perception of symptoms (Van Diest et al., 2005). On the other hand, other studies have focused on the importance of the gender approach over the biological to explain gender differences in several variables (Moscovitch, Hofmann, & Litz, 2005), including anxiety (Pérez-Blasco & Serra-Desfilis, 1997; Sánchez-López, Aparicio, & Dresch, 2006) and mental health (Matud & Aguilera, 2009). Within the gender approach, one explanation that researchers have offered to account for gender differences in anxiety symptoms is focused on the socialization processes. Among the factors related to the gender differential socialization process, different interactions generating vulnerability have been proposed (e.g., Bem, 1981; Brody & Hall, 2008; Ferrer, Bosch, Navarro, Ramis, & García, 2008). For example, while boys are educated to be prepared when facing an anxiety situation, girls are socialized to focus more on emotions. In this line, Egloff and Schmukle (2004) propose that men tend to underreport anxiety states, while women are more honest in that aspect. Thus, differences in the prevalence of anxiety could be explained by the differential sincerity between men and women when they go through an anxiety situation and not because women are actually more prone to suffer anxiety symptoms. However, others studies failed to prove that differences regarding the report of anxiety symptoms justify the marked difference in the prevalence of anxiety symptoms (King & Gordon, 1998; McLean et al., 2011). Another research line within the gender approach has pointed out the importance of the traditional female role for explaining the higher rates of anxiety in women. The theory of Feminine Gender Role Stress (Gillespie & Eisler, 1992) states that the overstress that involves the acceptance of the feminine ideal constitutes a vulnerability factor for women. Many women dedicate their lives to the fulfillment of the traditional feminine gender role, which consists in engaging in stereotyped behaviors or thoughts as controlling the physical appearance, being disproportionately concerned to please others, being passive and/or being dependent of others. In this regard, some traits associated with femininity such as orientation towards emotion (warmth, understanding, emotional awareness) and interpersonal orientation (sensitivity to the needs of others, need for affiliation; Cyranowski, Frank, Young, & Shear, 2000) could increase the vulnerability of women to anxiety. Other studies have found that women with a sharp feminine profile and with traditional beliefs of their own gender evidence greater levels of anxiety (e.g. Matud et al., 2009; McLean et al., 2010; Pérez-Blasco et al., 1997; Styanova & Hope, 2012; Van Diest et al., 2005). Another important characteristic of the traditional feminine role is the importance of physical appearance and the importance of being thin. These traditional female roles are related to body image issues, weight control and poor nutrition in women (Malson & Burns, 2009; Smolak & Murnen, 2004). Body dissatisfaction, which is a characteristic related to the canons of beauty, perfection, and thinness, contributes to discomfort and manifests itself in anxiety (Barberousse, 2009; Smolak et al., 2004; Saltzberg & Chrisler, 2006). Empirical studies among women from different countries have found a relationship between a firm belief in the traditional female role and harmful behaviors (e.g., Anastasiadou, Aparicio, Sepúlveda, & Sánchez-Beleña, 2013), and others have identified a relationship between some dimensions of the Conformity to Feminine Norms Inventory (CFNI, Mahalik et al., 2005), namely the Thinness, Romantic Relationships and Investment in Appearance dimensions, and eating disorders symptoms (Green, Davids, Skaggs, Riopel, & Hallengren, 2008; Mahalik et al., 2005; Smolak & Murnen, 2008). Furthermore, the adherence to the Thinness aspect of the traditional feminine gender role not only predicts the development of eating disorders, but also increments the subjective perception of stress, worry and rumination, being these variables related to cognitive anxiety (Esteban-Gonzalo, Aparicio-García, & Esteban-Gonzalo, 2017; Giménez-Páez & Aparicio-García, 2017; Giménez-Páez, Aparicio-García, & Ramos-Cejudo, 2013). Therefore, the conformity to some dimensions of the feminine gender role could explain part of the differences in anxiety that emerge between genders.
In Spain, femininity research employs scales that have been formulated during the 70's (Fernández, Del Olmo, & Rodríguez, 2007; García & Freire, 2000; García-Vega, Fernández García, & Rico Fernández, 2005) obtaining results that support a multidimensional model, in accordance with Mahalik's model (2005) and not the dualist model (Fernández et al., 2007; Spence, 1985). The dualistic conception of gender considers masculinity and femininity as two independent sociocultural factors derived from the dimensions traditionally associated with masculinity (instrumentality) and femininity (expressiveness). This approach makes the fourfold typology (masculine, feminine, androgynous, and undifferentiated) possible, not based on sexual dimorphism but emphasizing the social reality of gender. For example, Bem's Sexual Inventory (Bem, 1974); California Psychological Inventory (Baucom, 1976); Personal Attributes Questionnaire (Spence, Helmreich & Stapp, 1974, 1975). Several studies have shown that the dualist model does not explain the diversity of the gender construct, and it is precisely due to that limitation that multidimensional perspectives (and scales) emerged (see Mahalik et al., 2005; Parent y Moradi, 2010, 2011). In this study we rely on the theory of conformity to feminine norms, which is part of a multidimensional concept that considers femininity as the degree of conformity with a heterogeneous set of social norms on behavior, attitudes and beliefs that are considered desirable in women (Mahalik et al., 2005).
As mentioned in the previous paragraphs, several studies have shown an association between conformity to feminine norms and psychological health status, in which a higher likelihood of reporting psychologic symptoms was found among women with medium-high conformity to feminine roles (Esteban Gonzalo, Aparicio-García, & Estaban-Gonzalo, 2017). Therefore, the first goal of this study is to measure the relationship between gender and anxiety considering previous studies examining anxiety as a function of gender roles. On the other hand, recent studies have indicated the relationship between conforming to the feminine gender norm of Thinness and subjective perception of stress, worry and rumination (Esteban-Gonzalo et al., 2017; Giménez-Páez, 2017; Giménez- Páez et al., 2017; Giménez-Páez et al., 2013). Because subjective perception of stress, worry and rumination are variables related to cognitive anxiety, we can hypothesize that conforming to the Thinness dimension will predict higher levels of cognitive and total anxiety. Therefore, our second goal is to explore whether the adherence to the Thinness dimension explains higher levels of cognitive and total anxiety and, in general, whether the diverse gender norms are associated differentially to the three dimensions of anxiety.
MethodParticipantsThe participants were 234 women, aged 18-65 (mean age = 33.62, standard deviation = 11.34), who volunteered to participate in the study. Regarding the marital status, 52.6% were single, 32.5% were married, and the 6.8%, 5.6% and 2.6% had a partner, were separated, and were divorced or widowed, respectively. As for the educational level, 52.2% of women had completed higher education, 37.1% had secondary education and 10.8% had primary studies. Regarding their current employment status, 65.3% of participants were employed, 16.0% worked at home, 16.9% were unemployed and 1.8% were retired or pensioners. Finally, 53.2% reported belonging to a medium-low socio-economic level, and the remaining 46.8% to a medium-high.
Instruments1. Anxiety was measured using the Inventory of Situations and Responses of Anxiety (ISRA; Miguel-Tobal et al., 2002). It includes situations and responses (S-R) that provide separate assessment of reactivity in the three response systems (Cognitive, Physiological and Motor Anxiety). It includes 22 situations, 24 responses and 224 items. Items are rated on a 5-point Likert-scale, from 0 (hardly ever) to 4 (nearly always). The ISRA shows an adequate internal consistency of .99 and test-retest reliability of 0.81 (Miguel-Tobal et al., 2002). Cronbach's alpha coefficients in the present study were .874 for the Cognitive component, .920 for Physiological, .921 for Motor, and .957 for the whole scale, indicating adequate internal consistency.
2. The Conformity to Feminine Norms Inventory (CFNI; Mahalik et al., 2005; Spanish adaptation of Flores, Sánchez López, & Dresch, 2011) is an 84-item scale that measures the degree of adherence to traditional female standards. Items are rated on a 4-point Likert-scale, from 0 (strongly disagree) to 3 (strongly agree). It includes 8 subscales: Nice in Relationships (e.g., It is important to let people know they are special), Care for Children (e.g., I would take care of the children for fun), Thinness (e.g., I would be happier if I were thinner), Sexual Fidelity (e.g., I would feel guilty if I had a one-night stand), Modesty (e.g., I always downplay my achievements), Romantic Relationships (e.g., Having a romantic relationship is essential in life), Domestic (e.g., I enjoy spending time making my living space look nice) and Investment in Appearance (e.g., I spend more than 30minutes a day doing my hair and makeup). Scoring high on the scale reflects a high adherence to a feminine traditional role, like pursuing the ideal in home care, children, physical appearance, etc. (Mahalik et al., 2005). The CFNI has an adequate total internal consistency (α = .86). Reliability ranges from .82 (Investment in Appearance) to .92 (Care of Children). In the present study, the total scale has a reliability of α = .81 and the reliability in the subscales ranges from .72 (Romantic Relationships) to .91 (Care of Children).
ProcedureParticipants were selected by probability snowball method. The questionnaires were distributed to psychology students and the personal network of the research team. The message communicated to female participants was: “We are conducting research in order to discover the relationship between specific cognitive, emotional and gender processes relevant to the health of people. Participation is completely voluntary and involves completing a series of questionnaires related to the variables mentioned above. All data obtained through these questionnaires is related to the variables analyzed in this study. The study will not seek irrelevant information. Anonymity and confidentiality of the data will always be respected in accordance with current legislation (Law 15/1999 of 13 December). The procedure was in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. The inclusion criteria were being a female over 18, encompassing a wide range of ages.
Data analysisPreliminary analyses were carried out in order to identify differences between the sample of psychology students (n = 122) and the rest of the sample (n = 112) in the variables of interest, namely the dimensions of ISRA and the dimensions of the CFNI. Several independent samples t-test analyses were done accordingly. Pearson correlation analyses were then conducted to examine the relationship among the criterion variables measured with CFNI and ISRA in order to test our first hypothesis. Regarding our second goal, ordinary least squares regressions were performed through the stepwise procedure, where the dimensions of the CFNI were introduced as predictors of the ISRA dimensions. Besides the CFNI dimensions, the main effect of age as well as the interactions between age and each of the CFNI dimensions were also introduced in the model, as itmay be possible that women conform differently to some dimensions depending on their age (e.g., recent advances in equality in Spain could have led to different conformity with gender roles in different age groups of women).
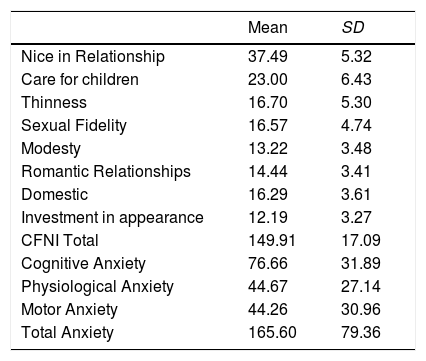
ResultsThe t-test analyses performed between the psychology students and the rest of the of the sample showed that there were no significant differences in any of the variables (Nice in Relationship, t = -1.45, p = .148; Care for children, t = 1.29, p = .196; Thinness, t = 0.95, p = .343; Sexual Fidelity, t = -0.52, p = .606; Modesty, t = 1.55, p = .121; Romantic Relationships, t = -0.17, p = .864; Domestic, t = 0.62, p = .537; Investment in Appearance, t = -0.70, p = .484; Total CFNI score, t = 0.46, p = .640; Cognitive Anxiety, t = 1.80, p = .074; Physiological Anxiety, t = 0.01, p = .989; Motor Anxiety, t = 1.05, p = .294; Total ISRA score, t = 1.14, p = .255). The descriptive statistics (mean and standard deviation) of the CFNI and ISRA dimensions are reported in Table 1.
Descriptive statistics of the ISRA and CFNI dimension.
| Mean | SD | |
|---|---|---|
| Nice in Relationship | 37.49 | 5.32 |
| Care for children | 23.00 | 6.43 |
| Thinness | 16.70 | 5.30 |
| Sexual Fidelity | 16.57 | 4.74 |
| Modesty | 13.22 | 3.48 |
| Romantic Relationships | 14.44 | 3.41 |
| Domestic | 16.29 | 3.61 |
| Investment in appearance | 12.19 | 3.27 |
| CFNI Total | 149.91 | 17.09 |
| Cognitive Anxiety | 76.66 | 31.89 |
| Physiological Anxiety | 44.67 | 27.14 |
| Motor Anxiety | 44.26 | 30.96 |
| Total Anxiety | 165.60 | 79.36 |
Notes. CFNI = Conformity to Feminine Norms Instrument.
Regarding our first hypothesis, Table 2 shows the Pearson correlation coefficients between the CFNI and the ISRA dimensions. As can be seen, the total score in the CFNI questionnaire significantly correlated with Cognitive Anxiety (r = .136), indicating that women with higher adherence to gender norms in CFNI are more likely to suffer from Cognitive Anxiety. The Cognitive Anxiety variable had the greatest relationship to compliance with the feminine gender role, specifically, Thinness (r = .213) and Sexual Fidelity (r = .152). Furthermore, Total Anxiety correlated positively with the gender norm referring to Thinness (r = .157).
Pearson correlations between CFNI and Anxiety scores.
| Anxiety | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | CFNI Total |
|---|---|---|---|---|---|---|---|---|---|
| Cognitive | .037 | .029 | .213** | .152* | .091 | .054 | -.067 | -.052 | .136* |
| Physiological | .003 | .038 | .070 | -.014 | .088 | .079 | -.100 | .014 | .048 |
| Motor | .062 | .029 | .122 | -.088 | .025 | .084 | -.112 | -.057 | .031 |
| Total | .040 | .036 | .157** | .022 | .077 | .081 | -.105 | -.038 | .083 |
Note: *p < .05; ** p < .01. CFNI = Conformity to Feminine Norms Instrument; (1) Nice in Relationship; (2) Care for children; (3) Thinness; (4) Sexual Fidelity; (5) Modesty; (6) Romantic Relationships; (7) Domestic; (8) Invest in appearance.
Regarding the second hypothesis, regression analyses showed that only Cognitive Anxiety and Total Anxiety were significantly predicted by some CFNI sub-dimensions, while neither Physiological nor Motor Anxiety were explained by any of the CFNI dimensions. The best equation for predicting Total Anxiety was the model including Thinness as a predictor variable. The regression equation for this model is: Total Anxiety = 127.339 + 2.396 (Thinness). The coefficient of determination is .026, which means conforming to the Thinness dimensions explains 2% of the variance of the Total Anxiety. Regarding Cognitive Anxiety, three dimensions of the CFNI scale resulted relevant: Thinness, Sexual Fidelity and Investment in Appearance, yielding the following regression equation: Cognitive Anxiety = 51.224 + 1.510 (Thinness) + 1.022 (Sexual Fidelity) - 1.336 (Investment in Appearance). The coefficient of determination was .091, which implies that Sexual Fidelity, Thinness and Investment in Appearance explains 9% of the variance of Cognitive Anxiety.
DiscussionThe aim of this study was to explore the relationship between the conformity to traditional feminine norms and expressions of anxiety. The correlation analyses showed that the Thinness dimension correlated with two dimensions of anxiety, namely Cognitive and Total Anxiety. These results support the finding of previous empirical studies that have highlighted how the importance of being concerned and attempting to maintain a slim and slender appearance encourages the experience of anxious symptoms among women (e.g., Giménez- Páez, 2017; Giménez- Páez et al.; Green et al., 2008; Mahalik et al., 2005; Smolak et al., 2008). Another significant relationship was found between the dimension Sexual Fidelity and Cognitive Anxiety. Previous studies have already linked Sexual Fidelity and Anxiety in situations where an important relationship is seriously threatened (Burchell & Ward, 2011; García-Leiva, Gómez-Jacinto, & Canto-Ortíz, 2001; Miller & Maner, 2009; Takahashi, Matsuura, Yahata, Koeda, Suhara & Okubo, 2006). However, this is the first time, as far as we know, that a relationship between the Sexual Fidelity dimension measured with the CFNI and Cognitive Anxiety has been found. This result suggests that women who conform more with the norm of being faithful to their partners, that is, women who do not frequently change sexual partner and maintain long-term relationships over time, suffer more cognitive symptoms of anxiety. This could be due to the fear that involves the possible loss of sexual exclusivity, where the loss of commitment and intimacy threaten the health of the relationship, and due to the intersexual hypervigilance referred to the attractiveness (Mane, Miller, Rouby & Gailliot, 2009).
Regarding the regression analysis, a first result showed that age did not moderate the relationships between any of the CFNI subdimensions and anxiety. These results are in line with the findings of López-Saéz, Morales and Lisbona (2008), who found that the adherence to gender norms related to femininity, especially the norms associated to familiar relationships, do not decrease across the life span, whereas stereotypes related to work tend to diminish markedly. A second result was that Total Anxiety was significantly explained by the Thinness dimension of the CFNI, indicating that women who tend to conform to the feminine role of Thinness report higher levels of Total Anxiety (e.g., negative thoughts, worry, physiological arousal, or motor activity). Although the explained variance is rather low (2%), these results support previous findings where the endorsement of the Thinness dimension was linked to anxiety symptoms, not measured at scale level (Esteban Gonzalo et al., 2017; Sánchez-López, Saavedra, Dresch, & Limiñana, 2014). Also in this line, conforming to the Thinness dimension has been found to systematically predict a poorer psychological health (anxious and depressive symptoms and social maladjustment) and aspects related to vulnerability to anxiety, such as subjective stress perception and ruminative response style (Giménez-Páez, 2017).
The second regression analysis showed that women who conform to the Thinness and Sexual Fidelity dimension, and do not conform to Investment on Appearance dimension, exhibited higher levels of Cognitive Anxiety (e.g., easily becoming worried, having negative thoughts about oneself, feeling insecure). Regarding the Thinness dimension, other research projects (e.g. King et al., 1998; Matud et al., 2009; McLean et al., 2010; Styanova et al., 2012) have already found that conforming to feminine norms related to body image issues lead to a greater vulnerability to anxiety symptoms (e.g., Barberousse, 2009; Cyranowski et al., 2000; Esteban-Gonzalo et al., 2017; Giménez-Páez et al., 2017; Pérez-Blasco et al., 1997; Sánchez & Crocker, 2005; Rood, Roelofs, Bögels, & Meesters et al., 2012; Smolak et al., 2004). As for the Sexual Fidelity dimension, we have already explained in the beginning of this section that the need for exclusivity, commitment and intimacy regarding the sexual life may increase the cognitive anxiety due to the fear of infidelity and due to the hypervigilance of physical attractiveness compared to other women.
Finally, regarding the Investment in Appearance dimension, a previous study has found a positive link between spending time caring about one‘s physical look and experiencing higher levels of anxiety, depression and low self-esteem (Neckenig, 2017). However, our results go in the opposite direction: it seems that having a high score in the Investment in Appearance dimension leads to lower levels of Cognitive Anxiety. A plausible explanation can be found in the theory of Feminine Gender Role Stress (Gillespie et al., 1992), which proposes that the overstress that involves the attainment of traditional feminine roles constitutes a vulnerability factor. Many women might dedicate their lives to the fulfillment of some traditional feminine gender roles, such as controlling their physical appearance. Therefore, not investing enough time in physical appearance care could contribute to the increase of feelings of inadequacy with respect to gender stereotypes congruent with the ideals of beauty.
The fact that high conformity to the traditional feminine norm of Thinness and Sexual Fidelity and the low conformity to Investment in Appearance norm contributes to greater Cognitive Anxiety, allows us to relate our results to other empirical findings that found a higher tendency to be concerned (Zalta & Chambless, 2008) and to ruminate (Aldao et al., 2010) in women. A higher conformity to the traditional feminine roles increases the worry for reaching those standards and the rumination. These two cognitive processes affect the processing of emotional information, and therefore lead to anxiety symptoms. Hence, conforming to a traditional feminine standard might lead to higher levels of Cognitive Anxiety through the worry and the rumination processes (Cano-Vindel & Miguel-Tobal, 2001; Eysenck & Eysenck, 2007).
However, it should be kept in mind that the determination coefficients of both regression models are rather low: .026 for Total Anxiety and .091 for Cognitive Anxiety. A possible explanation is that, according to the cognitive models of emotion and stress (Lazarus & Folkman, 1987) and vulnerability to emotional disorders (e.g., Barlow; 2000; Barlow, Allen, Choate, 2004; Beck, 1987), there are many other variables that also explain why people suffer from anxiety symptoms, as for instance having dysfunctional attitudes and beliefs, engaging in behavioral and cognitive avoidance behaviors or thoughts (e.g., worry), experiencing cognitive biases that increase the perception of threat in ambiguous situations, etc. Because these variables have a greater influence on the development of anxiety disorders, and given the low determination coefficients obtained in this study, we could conclude that although gender variables have a low contribution to the explanation of the manifestation of anxiety symptoms among women, they still add relevant information to an integrative model.
On the other hand, we expected to find some relationships that were not actually present. For instance, other studies have found an empirical relationship between Thinness and Physiological Anxiety (e.g., sweating, tension, stomach pain) and Motor Anxiety (e.g., tendency to shun or avoid a situation or repetitive movements) (e.g., Brunet, Sabiston, Dorsch, & McCreary, 2010; Berg, Thompson, Obremski-Bradon, & Coovert, 2002). However, in our study this relationship is not clear, since Thinness only explains part of the variance of the Cognitive and Total Anxiety. This contradictory result could be explained by the fact that CFNI does not measure behavior but beliefs or thoughts about the female role, so the dimension of anxiety in which we would expect more significant relationships is the one more related to thoughts, that is, Cognitive Anxiety.
The influence of variables related to gender in anxiety responses could occur through different interactions among cognitive variables, such as beliefs or expectations, and behavioral variables that, across socialization processes, participates in the gender typing, generating models of femininity. These femininity models might modulate intellective and emotional processes (García et al., 2000), leading to subjective factors that shape attitudes and lifestyles. The interactions between different biological, psychological and social components in anxiety responses and salutogenic potential require further evaluation of the different explanatory factors proposed regarding gender and sex differences with implications for the prevention and therapeutic approach optimizing, for example, therapeutic strategies related to the management and reduction of stress, and orientations for change inaccurate and unrealistic beliefs concerning femininity (APA, 2007; Borrell et al., 2008; Matud et al., 2009; Mussap, 2007).
Finally, this study has some limitations. The first one is related to the sampling technique: we used the snowball technique, and this type of sampling can generate mowed used estimators due to the bias of social distance, the island model and forced bias field, which affects the representativeness of the sample and results, limiting their extrapolation to the general population. However, no differences were found among psychology students and general population in any of the variables of interest. A second limitation is the cross-sectional design employed in this study that makes the establishment of causal relationships impossible.
For future studies, we suggest the use of longitudinal designs in order to analyze the effect that life events in women have in the gender and anxiety variables. Another suggestion is to further explore the relationship between feminine norms and relevant cognitive variables, such as worry and rumination, including their interaction with stressful stimuli, which are more prevalent in women.